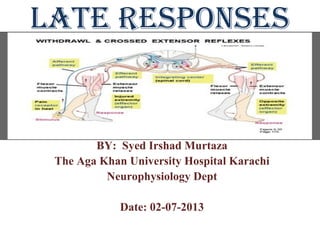
Late Responses (F-wave and H.Reflex)
•Download as PPT, PDF•
149 likes•51,907 views

This document provides information about late responses in nerve conduction studies, including F-waves, H-reflexes, and axon reflexes. It discusses the mechanisms, characteristics, and clinical applications of each response. The F-wave results from antidromic stimulation of motor neurons and evaluates more proximal nerve segments. The H-reflex is a monosynaptic stretch reflex that is reliably measured in the lower limbs. Axon reflexes occur due to terminal nerve branching and suggest reinnervation. Late responses provide valuable information about radiculopathies and plexopathies that cannot be observed with distal nerve studies alone.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Late Responses (F-wave and H.Reflex)
Similar to Late Responses (F-wave and H.Reflex) (20)
More from Murtaza Syed
More from Murtaza Syed (18)
Recently uploaded
Recently uploaded (20)
Late Responses (F-wave and H.Reflex)
- 1. LATE RESPONSES BY: Syed Irshad Murtaza The Aga Khan University Hospital Karachi Neurophysiology Dept Date: 02-07-2013
- 2. Introduction to late responses • Nerve conduction studies are basically performed to study the distal segment involvement. The late responses are preformed to study the more proximal segment involvement(plexus and roots). There are 3 different late responses: 1.F wave response 2.H reflex & 3- The axon reflex. Out of these late responses H reflex and F wave are preformed to study the proximal regions of nerves.
- 3. Introduction to F-wave Response • The name F wave is derived from the first time in the intrinsic muscles of foot by Magladery and McDougal in 1950. The F-wave is a long latency muscle action potential seen after supramaximal stimulation to a nerve. • It results from antidromic stimulation of motor neurons involving conduction to and from spinal cord and occurs at the interface between peripheral and central nervous system.
- 4. Cont’d • The afferent and efferent for F waves are alpha motor neurons. They are produced at the supramaximal stimulus. • It is generally accepted that the F-wave is elicited when the stimulus travels antidromically along the motor fibers and reaches the anterior horn cell at a critical time to depolarize it.
- 6. Variability of F-wave Response • The F-wave is a variable response and is obtained infrequently after nerve stimulation. • So each f- response varies slightly in latency, configuration and amplitude because a different population of anterior horn cells is activated with each stimulation. • At least ten trains of F-waves should be obtained and the shortest latency F-wave among them is used.
- 7. F-Response
- 8. Characteristics of f-wave • The properties of F waves are as follows: • a). Latency • b). Chronodispersion • c). Amplitude • d). Persistence • e). F-Estimation • f). F wave ratio
- 9. Characteristics of F-Wave Latency: In the upper extremity, the F response usually occurs at a latency of 25 to 32 ms while in the lower extremity, the F response usually occurs at a latency of 45 to 56 ms. Chronodispersion: The chronodispersion is basically the maximal F-response latency minus minimal F response latency. Normal chronodispersion is up to 4 ms in the upper extremities and up to 6 ms in the lower extremities. F responses can be obtained from any motor nerve. Amplitude: The F response is actually a small CMAP, representing 1% to 5% of the muscle fibers.
- 10. Cont’d Persistency: Normal F wave persistence usually is 80% to 100% and always above 50%. F-Estimate: The F estimate takes into account the distal motor latency, the conduction velocity, and the patient‘s limb length to determine whether a prolonged F response is truly due to a lesion of the proximal nerve segment or merely reflects an abnormal distal motor latency or conduction velocity or an unusually tall patient. F estimate = (2D/CV) x 10 + 1 ms + DL
- 11. How to elicit F-Response F responses may be absent in sleeping or sedated patients. In these situations, absent or impersistent F responses are not necessarily a sign of pathology. If F responses are not obtained, first ensure that the nerve has been stimulated supramaximally. Second, the Jendrassik (reinforcement) maneuver Can be of help in "priming" the anterior horn cells. The patient can be asked to make a fist with the contralateral hand or clench the teeth prior to each stimulation. This maneuver often will elicit an F response where one was not present at rest.
- 12. Anodal blocking Although F responses typically can be obtained with the stimulator in the standard position (cathode distal), there is the theoretical possibility of anodal block (wherein the nerve hyperpolarizes under the anode, blocking antidromic travel of the action potential from the depolarization site under the cathode).
- 13. MACHINE SETTINGS FOR F-RESPONSE Several adjustments must be made to the EMG machine to record F responses, however. The gain should be increased to 200uV (because the amplitude of the F response is quite low), and the sweep speed should be increased to 5 or 10 ms, depending on the length of the nerve being studied. Supramaximal simulation must always be used, and often it is advisable to turn the stimulator around so that the cathode is more proximal.
- 14. H. REFLEX
- 15. Introduction to H-Reflex • The H-reflex is the electrical equivalent of the monosynaptic stretch reflex and is normally obtained in only a few muscles. • The H (Hoffmann's) reflex, named after German neurologist Johann Hoffmann • who first evoked the response in 1918.
- 16. G1 G2 G2 G3 G3
- 17. What is H-Reflex? • The H-reflex (or Hoffmann's reflex) is a reflectory reaction of muscles after electrical stimulation of type Ia sensory fibers (Primary Afferent Fibers which constantly monitor how fast a muscle stretch changes) in their innervating nerves. The H-wave, is the expression of a monosynaptic reflex, which runs in afferents from the muscle and back again through efferents of the same muscle. • OR
- 18. H-reflex Definition • It is elicited by selectively stimulating the sensory Ia fibres (Primary Afferent Fibers which constantly monitor how fast a muscle stretch changes) of the posterior tibial or median nerve.
- 19. Cont’d • The stimulus travels along the Ia fibers, through the dorsal root ganglion, and is transmitted across the central synapse to the anterior horn cell which fires it down along the alpha (large lower motor neurons of the brainstem and spinal cord) motor axon to the muscle.
- 20. H-Reflex •
- 21. Location and stimulation • The H-Reflex which is monosynaptic reflex consistently obtained in normal adults only, by stimulating the tibial nerve sub-maximally, generally in the popliteal fossa, while recording from either gastrocnemius or soleus muscle, similar to the clinically elicited Achilles reflex. • The H.Reflex can also be recorded in median nerve recording from the FCR muscle and stimulating in elbow, and from femoral nerve recording from quadriceps muscles (VM, RF, VL, VI)
- 22. Anatomical location Although the H reflex can be recorded over any portion of the gastrocnemius and soleus muscles, the optimal location that yields the largest H reflex has been studied. If one draws a line from the popliteal fossa posteriorly to the Achilles tendon where the medial malleolus flares out and then divides that line into eight equal parts, the optimal location is at the fifth or sixth segment distally, over the soleus.
- 23. Anatomical localization of H.Reflex
- 24. Application of Electrodes • To record the H-Reflex, • G1 (active recording electrode) is placed 2-3 fingerbreadths distal to the soleus over the two bellies of the gastrocnemius muscle and • G2 (Reference Electrode) is placed over the Achilles tendon (usually 14cm distal to G1). • Ground electrode is generally placed between G1 and Stimulating electrode (stimulator cathode).
- 25. Normal Values for H.Reflex In normal subjects the latency of H.Wave should be ≤34ms, while recording from tibial nerve, depending on the length of the leg. The side to side onset latency difference shouuld be ≤1.5 ms. H/M ratio (maximal H / maximal M amplitude) should be ≤ 50%
- 26. RECORDING AND STIMULATING SITES
- 29. H-Reflex
- 30. Axon Reflex • An axon reflex is a small motor potential that is identical in latency, configuration with each successive stimulation and occurs between the F- response and direct motor (M) response with submaximal stimulations. • It is not a true reflex. • Axon reflexes, unlike F responses, superimpose perfectly on one another. Axon reflexes typically are seen in reinnervated nerves, especially when a submaximal stimulus is given.
- 31. Cont’d As a nerve is stimulated, the action potential travels both distally and proximally. If the proximally traveling antidromic pulse passes a terminal branching point, the pulse might then travel back down that branching nerve fiber to the muscle to create an axon reflex, which occurs after the M potential but before the F response.
- 32. Axon response
- 33. Axon Response
- 34. QUESTIONS: • 1. In severe C5, C6 radiculopathy, what would be the F.response if recording from APB? (Normal, Abnormal) • 2. In sever T1 radiculopathy what would be the F-response if recorded from Ulnar nerve ? (Normal, Abnormal) • 3. In radiculopathy of L5, S1 the f-response of tibial nerve recorded from (AH) will be? (normal, Abnormal) • 4. Radiculopathy that involves S2,S3 only, the f-response would be _____ if recorded from EDB? (Normal, Abnormal) • 5. Which of the following radiculopathies does H.Reflex help in the most? (L4, L5, S1, S2) • 6. H.Reflex is elicited by_____technique(Orthrodomic, antidromic) • 7. Axon Reflex (A.Response) is a____response (Normal, Abnormal) • 8. Axon reflex is a sign of? Denervation,Reinnervation,Demyelination
- 35. Thank you