Lymphatic system of upper and lower limbs in human body
•
1 like•426 views

Lymphatic drainage- Upper limb and Lower limb, Lymph nodes and their location and function.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Lymphatic system of upper and lower limbs in human body
Similar to Lymphatic system of upper and lower limbs in human body (20)
More from Dr Usha (Physio)
More from Dr Usha (Physio) (20)
Recently uploaded
Recently uploaded (20)
Lymphatic system of upper and lower limbs in human body
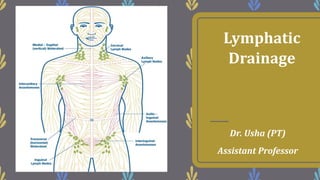
- 1. Lymphatic Drainage Dr. Usha (PT) Assistant Professor
- 2. • When circulating blood reaches the capillaries, part of its fluid content passes through them into the surrounding tissue as tissue fluid. Most of this tissue fluid re-enters the capillaries at their venous ends. Some of it is, however, returned to the circulation through a separate set of lymphatic vessels. These vessels begin as lymphatic capillaries which drain into larger vessels. • Along the course of these lymph vessels there are groups of lymph nodes.
- 3. • Lymph vessels are difficult to see and special techniques are required for their visualization. • Lymph nodes are small bean-like structures that are usually present in groups. These are not normally palpable in the living subject. • However, they often become enlarged in disease, particularly by infection or by malignancy in the area from which they receive lymph. They then become palpable and examination of these nodes provides valuable information regarding the presence and spread of disease.
- 4. Lymph Nodes In Upper Limb
- 5. Lymph Nodes In Upper Limb – The main lymph nodes of the upper limb are the axillary lymph nodes. These comprise anterior, posterior, lateral, central and apical groups. – Other nodes are: 1. The infraclavicular nodes 2. The deltopectoral node 3. The superficial cubital or supratrochlear nodes
- 6. 4. A few other deep lymph nodes lie in the following regions. i. Along the medial side of the brachial artery. ii. At the bifurcation of the brachial artery (deep cubital lymph node). iii. Occasionally along the arteries of the forearm.
- 7. Axillary Lymph Nodes – The axillary lymph nodes are scattered in the fibrofatty tissue of the axilla. They are divided into five groups. 1. The nodes of the anterior (pectoral) group lie along the lateral thoracic vessels, i.e. along the lower border of the pectoralis minor. They receive lymph from the upper half of the anterior wall of the trunk, and from the major part of the breast.
- 9. 2. The nodes of the posterior (scapular) group lie along the subscapular vessels, on the posterior fold of the axilla. They receive lymph from the posterior wall of the upper half of the trunk, and from the axillary tail of the breast. 3. The nodes of the lateral group lie along the upper part of the humerus, medial to the axillary vein. They receive lymph from the upper limb.
- 10. 4. The nodes of the central group lie in the fat of the upper axilla. They receive lymph from the preceding groups and drain into the apical group. They receive some direct vessels from the floor of the axilla. The intercostobrachial nerve is closely related to them. 5. The nodes of the apical or infraclavicular group lie deep to the clavipectoral fascia, along the axillary vessels. They receive lymph from the central group, from the upper part of the breast, and from the thumb and its web. The lymphatics from the thumb accompany the cephalic vein.
- 11. Infraclavicular Nodes – The infraclavicular nodes lie in or on the clavipectoral fascia along the cephalic vein. They drain the upper part of the breast, and the thumb with its web.
- 13. Deltopectoral Node – The deltopectoral node lies in the deltopectoral groove along the cephalic vein. It is a displaced node of the infraclavicular set, and drains similar structures.
- 14. Superficial Cubital Or Supratrochlear Nodes – The superficial cubital or supratrochlear nodes or epitrochlear nodes lie just above the medial epicondyle along the basilic vein. They drain the ulnar side of the hand and forearm.
- 15. Lymphatics Superficial lymphatics – Superficial lymphatics are much more numerous than the deep lymphatics. They collect lymph from the skin and subcutaneous tissues. Most of them ultimately drain into the axillary nodes, except for: i. A few vessels from the medial side of the forearm which drain into the superficial cubital nodes. ii. A few vessels from the lateral side of the forearm which drain into the deltopectoral or infraclavicular nodes.
- 16. • The dense palmar plexus drains mostly into the lymph vessels onto the dorsum of the hand, where these continue with the vessels of the forearm. • Lymph vessels of the back of forearm and arm curve round their medial and lateral surfaces and ascend up to reach the floor of the axilla. • Thus, there is a vertical area of lymph shed in the middle of back of forearm and arm.
- 18. – Deep Lymphatics • Deep lymphatics are much less numerous than the superficial lymphatics. They drain structures lying deep to the deep fascia. • They run along the main blood vessels of the limb, and end in the axillary nodes. • Some of the lymph may pass through the deep lymph nodes present along the axillary vein.
- 19. Clinical Anatomy • Inflammation of lymph vessels is known as lymphangitis, In acute lymphangitis, the vessels may be seen through the skin as red, tender (painful to touch) streaks. • Inflammation of lymph nodes is called lymphadenitis. It may be acute or chronic. The nodes enlarge and become palpable and painful.
- 21. • Obstruction to lymph vessels can result in accumulation of tissue fluid in areas of drainage. This is called lymphoedema. This may be caused by carcinoma. Infection with some parasites like filaria, or because of surgical removal of lymph nodes. • Pain along the medial side of upper arm is due to pressure on the intercostobrachial nerve by enlarged central group of axillary lymph nodes.
- 22. Lymph Nodes In Lower Limb
- 23. – Most of the lymph from lower limb drains into the inguinal lymph nodes, either mostly directly or partly indirectly through the popliteal and anterior tibial nodes. – The deep structures of the gluteal region and the upper part of the back of the thigh drain into the internal iliac nodes along the gluteal vessels.
- 24. Classification I. Lymph nodes a) Superficial inguinal lymph nodes b) Deep • Deep inguinal lymph nodes • Popliteal lymph nodes • Anterior tibial lymph nodes II. Lymphatics a) Superficial b) Deep
- 25. Superficial Inguinal Lymph Nodes – These are very important because they drain the skin and fasciae of the lower limb; the perineum and the trunk below the umbilical plane. They are divided into three sets. • The superficial inguinal lymph nodes are variable in their number and size. • There arrangement is T- shaped, there being a lower vertical group and an upper horizontal group. • The upper nodes can be subdivided into the upper lateral and upper medial groups.
- 26. 1. The lower vertical group is placed along both sides of the terminal part of the great saphenous vein, and contains about four or five nodes. Lower vertical group drains lymph from most of the lower limb. They drain the skin and fasciae of the lower limb (great saphenous territory), except the buttock and the short saphenous territory. A few lymphatics, accompanying the short saphenous vein, cross the leg, accompany the great saphenous vein, and drain into this group of nodes.
- 28. 2. The upper lateral group is placed below the lateral part of the inguinal ligament, and contains about two or three nodes. They drain the skin and fasciae of the upper part of the lateral side of the thigh, the buttock, the flank and the back below the umbilical plane. Upper lateral group drains lymph from infra-umbilical part of anterior abdominal wall and gluteal region.
- 29. 3. The upper medial group is placed below the medial end of the inguinal ligament. One or two nodes may lie above the inguinal ligament along the course of the superficial epigastric vessels. The group contains two to three nodes. They drain: a. The anterior abdominal wall below the level of the umbilicus. b. The perineum, including extemal genitalia, except the glans, the anal canal below the pectinate line, the vagina below hymen and the penile part of the male urethra. c. The superolateral angle of the uterus, via the round ligament.
- 30. – Efferents from all superficial inguinal nodes pierce the cribriform fascia, and terminate in the deep inguinal nodes. A few may pass directly to the external iliac nodes.
- 31. Deep Inguinal Lymph Nodes – These are about four to five in number, and lie medial to the upper part of the femoral vein. The most proximal node of this group; gland of Cloquet or of Rosenmtiller, lies in the femoral canal. These nodes receive afferents from: – 1 The superficial inguinal nodes. – 2 The popliteal nodes. – 3 Glans penis or clitoris. – 4 The deep lymphatics of the lower limb accompanying the femoral vessels. – Their efferents pass to the external iliac nodes.
- 32. Popliteal Lymph Nodes – These nodes lie near the termination of the small saphenous vein, deep to the deep fascia. One node lies between the popliteal artery and the oblique popliteal ligament. They receive afferents from: 1. The territory of the small saphenous vein. 2. The deep parts of the leg (through vessels running along the anterior and posterior tibial vessels). 3. The knee joint. – Their efferents run along the popliteal and femoral vessels, and terminate in the deep inguinal nodes.
- 33. Anterior Tibial Lymph Nodes – One inconstant node may lie along the upper part of the anterior tibial artery. When present it collects lymph from the anterior compartment of the leg, and passes it on to the popliteal nodes.
- 34. Lymphatics Superficial lymphatics – These lymph vessels are larger and are more numerous than the deep lymphatics. They run in the superficial fascia and ultimately form two streams. The main stream follows the great saphenous vein, and ends in the lower vertical group of superficial inguinal lymph nodes. – The accessory stream follows the small saphenous vein and ends in the popliteal lymph nodes.
- 36. Deep Lymphatics – These are smaller and fewer than the superficial lymphatics, although they drain all structures lying deep to the deep fascia. They run along the principal blood vessels, and terminate mostly into the deep inguinal nodes, either directly or indirectly through the popliteal nodes. – The deep lymphatics from the gluteal region and from the upper part of the back of the thigh accompany the gluteal vessels and end in the internal iliac nodes.
- 37. Clinical Anatomy – Elephantiasis: Lymphatic obstruction caused by the parasite filaria is very common in the lower limb. This results in great hypertrophy of the skin and of subcutaneous tissue (elephantiasis). – The commonest cause of a swelling in the inguinal area is enlargement of the inguinal lymph nodes. This can be caused by infection, or carcinoma, anywhere in the area drained by these nodes
- 39. Thank you