
Recomendados
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (20)
Similar a Obstet gynecol surv 67 (426 35) 2012
Similar a Obstet gynecol surv 67 (426 35) 2012 (20)
Obstet gynecol surv 67 (426 35) 2012
- 1. 20 CME REVIEW ARTICLE Volume 67, Number 7 OBSTETRICAL AND GYNECOLOGICAL SURVEY Copyright * 2012 by Lippincott Williams & Wilkins CHIEF EDITOR’S NOTE: This article is part of a series of continuing education activities in this Journal through which a total of 36 AMA/PRA Category 1 Creditsi can be earned in 2012. Instructions for how CME credits can be earned appear on the last page of the Table of Contents. Obstetric Hemorrhage and Coagulation: An Update. Thromboelastography, Thromboelastometry, and Conventional Coagulation Tests in the Diagnosis and Prediction of Postpartum Hemorrhage Natascha M. de Lange, MD,* Marcus D. Lance, MD,† Renee de Groot, MD,‡ ´ ´ Erik A.M. Beckers, MD, PhD,§ Yvonne M. Henskens, PhD,¶ and Hubertina C.J. Scheepers, MD, PhD|| *Resident in Gynecology, Department of Obstetrics and Gynecology, Orbis Medical Centre, Sittard; †Anesthesiologist, Departments of Anesthesiology and Pain Treatment, ‡Resident in Prenatal Diagnosis, Department of Obstetrics and Gynecology, §Hematologist, Department of Internal Medicine-Hematology, ¶Clinical Chemist, Hematological Laboratory, ||Gynecologist, GROW School for Oncology and Developmental Biology and Department of Obstetrics and Gynecology, Maastricht University Medical Center, Maastricht, the Netherlands Globally, postpartum hemorrhage (PPH) is the leading cause of maternal morbidity and mortality. In the current treatment of severe PPH, first-line therapy includes transfusion of packed cells and fresh- frozen plasma in addition to uterotonic medical management and surgical interventions. In persistent PPH, tranexamic acid, fibrinogen, and coagulation factors are often administered. Secondary coa- gulopathy due to PPH or its treatment is often underestimated and therefore remains untreated, potentially causing progression to even more severe PPH. In most cases, medical and transfusion therapy is not based on the actual coagulation state because conventional laboratory test results are usually not available for 45 to 60 minutes. Thromboelastography and rotational thromboelastometry are point-of-care coagulation tests. A good correlation has been shown between thromboelastometric and conventional coagulation tests, and the use of these in massive bleeding in nonobstetric patients is widely practiced and it has been proven to be cost-effective. As with conventional laboratory tests, there is an influence of fluid dilution on coagulation test results, which is more pronounced with colloid fluids. Fibrinogen seems to play a major role in the course of PPH and can be an early predictor of the severity of PPH. The FIBTEM values (in thromboelastometry, reagent specific for the fibrin polymerization process) decline even more rapidly than fibrinogen levels and can be useful for early guidance of interventions. Data on thromboelastography and thromboelastometry in pregnant women are limited, particularly during the peripartum period and in women with PPH, so more research in this field is needed. Target Audience: Obstetricians & Gynecologists, Family Physicians Learning Objectives: After participating in this CME activity, physicians should be better able to manage postpartum hemorrhage and to evaluate the possible uses of thromboelastography and thromboelastometry to treat obstetric hemorrhage. All authors and staff in a position to control the content of this CME VII and procoagulative agents for the treatment of obstetric hem- activity and their spouses/life partners (if any) have disclosed that orrhage as discussed in this article. Please consult the product’s they have no financial relationships with, or financial interests in, any labeling for approved information. commerical organizations pertaining to this educational activity. Correspondence requests to: Natascha M. de Lange, MD, Poli The authors have disclosed that the US Food and Drug Admin- gynaecologie/Oost 11, Postbus 5500, 6130 MB Sittard, the istration has not approved the use of recombinant activated factor Netherlands. E-mail: nataschadelange@gmail.com. www.obgynsurvey.com | 426 Copyright © 2012 by Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
- 2. Obstetric Hemorrhage and Coagulation: Update & CME Review Article 427 PRACTICE PEARLS because specific pregnancy- and peripartum-related hemodynamic and hemostatic changes are likely to in- & The usefulness of conventional laboratory clot- fluence TEG/TEM results. For a correct interpretation ting tests is very limited in immediate situations of TEG/TEM in women with PPH, reference values such as PPH. for pregnancy have yet to be determined. The aim of & Do not underestimate coagulopathy (by dilution) this narrative review was to discuss: in the course and treatment of PPH. & Thromboelastography or thromboelastometry might 1) hemostasis and hemostatic changes during pregnancy, be helpful in the treatment of PPH once normal 2) definitions and management of PPH, values and evaluated cutoff values for intervention 3) coagulation and PPH, have been defined. 4) the principles of TEG and ROTEM, and 5) the use of TEG and ROTEM in obstetric hemorrhage. Globally, obstetric hemorrhage is the leading cause of maternal morbidity and mortality, with approxi- Hemostasis and Hemostatic Changes mately 25% of all maternal deaths caused by excessive During Pregnancy blood loss and inadequate treatment or resources.1 Berg et al2 reported that 40% of pregnancy-related Hemostasis is vital for preventing major blood loss deaths are potentially preventable, particularly deaths because it seals sites of injury in the vascular system; that occur as a consequence of hemorrhage. Obstetric however, it must be controlled to prevent blood from hemorrhage currently causes 7% of maternal deaths coagulating within the vasculature and restricting in the Netherlands.3 In addition to mortality, severe normal blood flow. In the last decades, our knowledge morbidity may occur after postpartum hemorrhage of coagulation has grown with development of the (PPH), that is, loss of fertility, Sheehan syndrome, cell-based model of coagulation.14,15 There has been a and multiple-organ failure due to hypovolemic shock.4 transition in knowledge, whereby the intrinsic and Taking these numbers and consequences into consid- extrinsic coagulation pathways are recognized to be eration, there is a need to improve the care around PPH. not redundant but as parallel generators of factor Xa The most common cause of massive PPH is uterine that occurs on different cell surfaces. atony; other causes include surgical incisions, lacera- The cell-based model of coagulation consists of tions, and coagulation disorders. Abnormal placen- initiation, amplification, and propagation phases. New tation, such as placenta previa or placenta accreta, is a in vivo models have identified tissue factor (TF) as the known risk factor for PPH, with an increasing inci- sole initiator of coagulation. Tissue factor is expres- dence mainly because of the rising rate of cesarean sed on cells outside the vascular system; once an in- deliveries. jury occurs, the TF-bearing cells are exposed to blood Coagulation disorders may present as a primary or and circulating factor VIIa immediately binds to TF. secondary cause of massive PPH; the latter is often This results in the generation of a small amount of underestimated and undertreated. Secondary coagu- factor IXa and thrombin, which then diffuse to the lation disorders may result from dilution (dilutional platelets. In the amplification phase, thrombin relea- coagulopathy) or depletion of clotting factors or sub- ses von Willebrand factor (vWF) and leads to gen- strates such as erythrocytes or platelets (consumptive eration of activated forms of factors V, VIII, and XI. coagulopathy). The development of secondary coag- In the propagation phase, the various factors and ulation disorders with delay in obstetric management enzymes assemble on the surface of the activated is a crucial prognostic factor for the severity of PPH.5 platelet to form the tenase complex and to generate Many guidelines and flowcharts have been published factor Xa, the prothrombinase complex is formed, and to optimize the management of PPH.6Y9 In these guide- thrombin generation takes places on the platelet sur- lines, conventional laboratory tests and vital parameters face. This process leads to generation of fibrin from are used to guide transfusion. The use of thromboelas- fibrinogen.15,16 tography (TEG) or thromboelastometry (ROTEM) in During pregnancy, plasma volume increases by massive bleeding in nonobstetric patients is widely 40% and the erythrocyte count increases by 25%. As a practiced and has been proven to be cost-effective. result, hemoglobin levels and hematocrit decrease be- Current guidelines for the treatment of massive hemor- cause of this physiological hemodilution.17 In addition, rhage in patients with injury from trauma recommend platelet levels drop because of both hemodilution and the use of TEG or TEM.10Y13 However, TEG/TEM increased consumption in the uteroplacental unit.17,18 results in patients with injury from trauma cannot be In contrast, levels of many coagulation factors in- easily compared with those from women during labor crease during pregnancy, including vWF, factors Copyright © 2012 by Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
- 3. 428 Obstetrical and Gynecological Survey VII and VIII, as well as fibrinogen and factor IX. The most common cause of PPH is uterine atony, Other factors, such as factors XII and V, remain un- which should be treated immediately by emptying changed.19,20 Natural coagulation inhibitors, such as the bladder and administering pharmacological agents protein S, decrease, and the fibrinolytic system is such as oxytocin, ergometrine, or misoprostol.7 Other negatively influenced by the increased plasminogen causes of blood loss, such as retained products of activator inhibitor and thrombin-activatable fibrino- conception, uterine, or birth canal trauma, or pre- lysis inhibitor. Overall, these changes result in a state existing coagulation problems must be considered as of hypercoagulability and hypofibrinolysis, which is well. Management should include the following steps: protective against excessive blood loss at delivery but (1) Laboratory evaluation: hemoglobin level, hemat- also leaves pregnant women more prone to throm- ocrit, platelet count, and fibrinogen concentration, as boembolic events. well as PT and aPTT. (2) Volume resuscitation: ini- Fibrinogen levels rise significantly from week 28 to tially fluid resuscitation, followed if necessary by twice the nonpregnant levels by term and remain el- transfusion of red blood cells to ensure rapid correc- evated throughout the first postpartum days.17,18,21Y23 tion of oxygen carrying capacity. The risk of dilu- The rise in fibrinogen levels is likely to be caused by tional coagulopathy due to fluid resuscitation should an increase in synthesis due to hormonal changes, be considered. (3) Correction of coagulation factors: particularly elevated estrogen levels.24 depending on laboratory results and the clinical D-Dimer values increase progressively during preg- condition of the patient, fresh-frozen plasma (FFP), nancy, peaking at the first day postpartum and de- fibrinogen, platelets, or tranexamic acid can be ad- creasing thereafter. This rise in D-dimers occurs with ministered. The off-label use of recombinant activated a simultaneous increase in circulating fibrinogen and factor VII should be considered only in refractory cases other procoagulant factors during pregnancy. Despite with ongoing bleeding after sufficient correction of all hypofibrinolysis, the excess fibrin deposition results deficiencies has been achieved. (4) Surgical measures: in an increase in tissue plasminogen activator and evacuation of retained placental fragments, balloon higher D-dimer values.17Y20,24,25 tamponade, selective embolization of the uterine artery, Despite these hemostatic alterations in pregnancy, uterine compression sutures (B-lynch), or hysterecto- laboratory studies show unchanged or only slightly my as necessary and as clinically indicated.6Y9 decreased levels of activated partial thromboplastin Above all, it is important to note that massive PPH time (aPTT), prothrombin time (PT), and interna- is potentially life threatening and requires a multi- tional normalized ratio (INR); all of these remain disciplinary approach, including all staff working at a within reference limits for nonpregnant women.20 labor ward, anesthesia, and hematology. The Confi- These overall hypercoaguable hemostatic changes dential Enquiry into Maternal and Child Health in contribute to the physiological preparation for deliv- the Netherlands strongly recommends the develop- ery and prevention of excessive blood loss postpar- ment of multidisciplinary massive hemorrhage guide- tum. An alteration in this equilibrium may influence lines, adapted to the hospital. Such protocols are widely the course of PPH. used in trauma medicine to simplify and expedite the delivery of blood products to hemorrhagic patients.13,29,30 In obstetrics, there are few publica- tions regarding the implementation of massive hem- Definitions and Management of PPH orrhage guidelines in clinical practice.31Y34 However, Definitions for PPH vary. In general, PPH is defined several publications report an improved maternal as blood loss of more than 500 mL within 24 hours outcome after the introduction of a multidisciplinary after vaginal delivery or 1000 mL after cesarean de- protocol and approach in PPH, despite more cases of livery. Blood loss more than 1500 mL, a decline in PPH.35,36 The use of these protocols and regular local hemoglobin of 4 g/dL or more, transfusion of at least drill is recommended; review of procedures for 4 units of red blood cells, or the need for a hemostatic management of PPH through regular courses can also (embolization) or operative intervention indicates be useful.7,34 severe PPH. Massive blood loss is defined as the loss of 1 blood volume, the loss of 50% of blood volume within 3 hours, or a loss rate of 150 mL/min.26 It is Coagulation Factors in PPH important to note that the amount of blood loss in PPH is very difficult to assess clinically and is usually Primary coagulation disorders are not frequently underestimated.27,28 identified as a cause of PPH, except in women on Copyright © 2012 by Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
- 4. Obstetric Hemorrhage and Coagulation: Update & CME Review Article 429 anticoagulation medication or with a known history of aPTT (to detect deficiencies of coagulation factors bleeding disorders.5 Case series have shown a higher VIII, IX, XI, and/or XII) and PT (to detect deficiencies incidence of PPH in women with inherited bleeding of coagulation factors X, VII, V, and II) only measure disorders such as von Willebrand disease (risk ratio, the plasma component of the coagulation cascade and 1.5Y3.0).37Y39 Other causes that have been indepen- were initially developed as laboratory tests to monitor dently associated with a significant risk of severe anticoagulant treatment, including heparin and vita- PPH include low levels of fibrinogen (even without min K antagonists, respectively. reaching levels of deficiency), vWF antigen, factor Transfusion with fluids, packed red blood cells, and XI, or platelet CD42b; TRAP-induced increase of FFP will aggravate dilutional coagulopathy as has platelet CD41a; nbd high values of serum residual been demonstrated in cardiac surgery.50 Such pro- prothrombin activity and blood group O. The presence ducts do not correct coagulation disorders completely of 2 or more independent risk factors showed an odds because even FFP contains insufficient amounts of ratio of 16.4 for severe PPH.40 coagulation factors. Most PPH protocols advocate the General screening of the pregnant population for transfusion of 4 FFP for every 6 units of packed red disorders of coagulation would not be cost-effective blood cells or if PT/aPTT is greater than 1.5 times or informative because of the low prevalence and normal, according to guidelines for management of insufficient data on reference ranges in pregnancy, as bleeding after major trauma. In recent years, there well as limited data on therapeutic algorithms based have been several publications that suggest a better on such screening results. In women with clinical outcome and fewer transfusions when transfusing PPH, however, primary coagulation disorders should packed red blood cells and FFP on a 2:3 or even on a be considered. Most patients with PPH due to a coa- 1:1 ratio and early transfusion of FFP; however, such gulopathy will have a history that points to bleeding studies are mainly retrospective.13,51Y53 tendency (bruising, hematoma, bleeding with teeth In persistent PPH, fibrinogen, coagulation factors, brushing, and/or heavy menstrual bleeding).41 and tranexamic acid are often administered. Tra- Severe PPH may result in secondary coagulopathy, nexamic acid has an antifibrinolytic effect and acts by similar to what is seen in massive blood loss in blocking the conversion of plasminogen to plasma. It patients with injury from trauma. This may be due to is effective in reducing perioperative and postopera- the consumption of coagulation factors, dilution, ac- tive blood loss54,55 and in reducing heavy menstrual idosis, or hypothermia. Resuscitation with crystalloid bleeding.56 During delivery of the placenta, there is fluids in large amounts may induce dilutional acido- rapid degradation of fibrinogen and fibrin, as well as sis, formation of interstitial edema, and impairment of activation of plasminogen activators and production microcirculation.42 Colloid fluids, in particular syn- of fibrin degradation products due to the activation of thetic colloids such as hydroxyethyl starch solutions the fibrinolytic system. The antifibrinolytic effect of (HESs), may impair clot formation and therefore in- tranexamic acid could theoretically reduce blood loss crease blood loss.43,44 Even new-generation medium- in the third stage of labor, although at present, there is molecular-weight HES disturbs fibrin polymerization insufficient evidence to support its use in this set- in patients undergoing spine surgery, and the presence ting.57 In addition, a study by Charbit et al found no of HES or gelatin solutions in patients with fibrino- evidence of hyperfibrinolysis in patients with PPH lysis leads to faster clot disintegration.45,46 Progressive because of severe uterine atony.48 The WOMAN Trial dilutional coagulopathy, hypothermia, and metabolic (World Maternal Antifibrinolytic Trial), a randomized acidosis have been referred to as the lethal triad in controlled trial in which tranexamic acid is compared nonpregnant patients with massive blood loss.47,48 to placebo in women with PPH, might resolve this In current guidelines for management of severe issue.58 PPH, transfusion of packed cells, FFP, and platelets, The off-label use of procoagulative agents such as in addition to uterotonic therapy, fluid resuscitation, recombinant factor VIIa is only indicated and effec- and surgical measures, is regarded as first-line ther- tive in the presence of adequate substrate for coagu- apy.6Y9 In most cases, therapy of PPH cannot be lation (fibrinogen and platelets) and is not without based on the actual hemostatic competence because risk; a meta-analysis reported significantly more ar- regular conventional coagulation tests typically re- terial thrombotic events in patients receiving recom- quire 45 to 60 minutes for results to be available and binant factor VIIa.59,60 Possible adverse effects of are nonspecific.49 One logistical challenge is the time uncontrolled administration of blood products and needed to prepare plasma from anticoagulant whole factor concentrates also include thrombosis and vol- blood samples. Another clinical challenge is that ume overload. Copyright © 2012 by Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
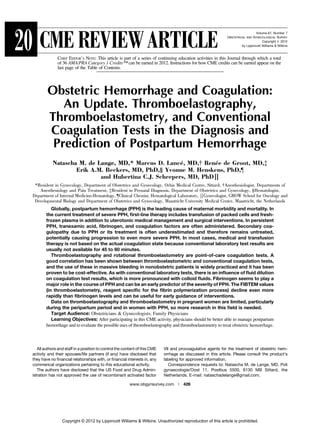
- 5. 430 Obstetrical and Gynecological Survey The absence of quick and specific laboratory tests vere bleeding. Although data are limited, results to monitor PPH and assess the development of a consistently favor the early administration of fibrin- secondary coagulopathy can result in excessive and ogen over FFP in bleeding patients.66 avoidable usage of blood products. A preferred ap- proach would be the selective administration of blood products and clotting factors according to deple- Principles of TEG and TEM tion.61,62 The general protocols and guidelines used Both TEG and ROTEM are so-called dynamic, for the nonpregnant patient are likely not adequate or viscoelastic coagulation tests, which represent the appropriate for peripartum women. In pregnancy, the whole coagulation process from the initiation of clot relative hypercoagulable state makes uncontrolled formation through fibrinolysis. The tests are per- treatment potentially more dangerous. In addition, formed on whole blood instead of plasma, which there are no clear therapeutic thresholds defined for saves time and means that these tests represent the peripartum women. It is unclear whether treatment interaction between cellular and plasma clotting fac- should be aimed at achieving minimal levels de- tors. These point-of-care devices have several sepa- scribed for nonpregnant subjects or whether preg- rate channels, allowing multiple samples to be run nancy normal values should be the goal. Evaluation of simultaneously or sequentially. fibrinogen levels presents a good example of this Thromboelastography was introduced by Hartert issue; Charbit et al63 investigated different coagula- in 1948 in a trial setting. Clinically, it was first used in tion parameters during PPH and found that PT, INR, 1985 in hepatic and cardiothoracic surgery. The TEG aPTT, fibrinogen, D-dimer, prothrombin, and factor V mechanism consists of a plastic pin attached to a were significantly lower in a group of women with torsion wire that is immersed in a rotating cup. After severe PPH compared to women with milder PPH. In clot formation, an electrical signal is traced as a curve both groups, however, the fibrinogen values were over time (Fig. 1). The outcome of a TEG tracing is within the reference range for nonpregnant subjects presented as 5 parameters: (2Y4 g/L). In the peripartum period, however, normal fibrinogen values are above what is considered normal & R: Period from initiation of the test to the initial and vary from 3.5 to 6.5 g/L.20 Consequently, values fibrin formation and pin movement (seconds) used to guide interventions might differ from non- & K: Time from the beginning of clot formation pregnant levels. until the amplitude of the TEG reaches 20 mm Fibrinogen is of importance in forming a firm clot (seconds) and is the first parameter to decrease during massive & > angle: Angle between the line in the middle of bleeding, due to increased fibrinogen consumption as the TEG tracing and the line tangential to the well as hemodilution resulting from fluid adminis- developing ‘‘body’’ of the TEG (degrees) tration. Fibrinogen is the only parameter that has been & Maximal amplitude (MA) = Greatest amplitude shown to be significantly lower and independently of the TEG tracing (mm) associated with progress toward severe bleeding. Fi- & LY30 = Rate of amplitude reduction 30 minutes brinogen levels of 2 g/L or lower have been reported to after MA have a positive predictive value of 100% and therefore could be an early predictor of severe PPH.63 Gayat et al64 published a retrospective cohort on the pre- dictors of severe PPH; in a univariate analysis, fi- brinogen levels less than 2 g/L and prothrombin time less than 50% were significant predictors of severe PPH, whereas in the multivariate analysis only fi- brinogen levels less than 2 g/L remained significant. Bell et al65 presented 6 cases of obstetric hemorrhage associated with hypofibrinogenemia (all fibrinogen levels G1.5 g/L) that was treated with fibrinogen; co- agulation test results rapidly normalized and severe hemorrhage improved. Notably, however, all patients also received platelets, FFP, and packed red blood cells. In contrast to obstetrics, many surgical specialties use early administration of fibrinogen in cases of se- Fig. 1. Result of TEG. Copyright © 2012 by Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
- 6. Obstetric Hemorrhage and Coagulation: Update & CME Review Article 431 Alterations of the normal TEG pattern and varia- ferentiate between the related pathways (extrinsic tions in the different parameters provide information and intrinsic pathway respectively). regarding alterations in the dynamic coagulation 2. Insufficient substrate for clot formation due to process. Alterations in the R value are related to co- platelet and fibrinogen deficiency: CT is normal, agulation factor activation, K and > angle parameters CFT is slightly prolonged, and the clot amplitude are related to coagulation factor amplification, MA (CA) and MCF are reduced. Platelets are inhibited reflects platelet aggregation, and LY30 reflects fibri- in FIBTEM, implying that FIBTEM evaluates the nolysis at different points in time (LY30 is 30 minutes specific fibrinogen component. after maximum amplitude is reached). 3. Hyperfibrinolysis: Formation and strength are Thromboelastometric tests can be run in native normal, but the clot lysis index is increased. This whole blood. However, it is common to use activators can be confirmed by the APTEM12,68,69 (Fig. 2). to speed up the process and standardize the tests and to simulate different pathways of activation. Tissue Use of TEG or ROTEM in Obstetrics factor and kaolin can be incorporated into the TEG cuvette, and heparinase and platelet GpIIb/IIIa inhi- There have been several publications on the use of bitors can also be used to provide more detailed in- TEG and less on the use of ROTEM in pregnancy. formation in specific clinical settings67 (Fig. 1). Some studies have compared pregnant women to Thromboelastometry is based on the same princi- nonpregnant subjects, confirming the hypercoaguable ples as TEG, but its mechanism is a rotating plastic pin state of parturients with TEG.70,71 Other studies fo- fixed on a steel axis that is immersed into a cup. The cused on specific situations during pregnancy and movement of the pin is converted to an optical signal delivery. In this review, we focus on normal preg- and transferred to a graphical display. The outcome of nancy, normal delivery, and PPH. a TEM tracing is very similar to the TEG with results also presented as 5 parameters: Comparing Pregnant With Nonpregnant Women & Clotting time (CT): Time from start of mea- Armstrong et al72 compared the TEM coagulation surement until initiation of clotting (seconds) parameters of healthy pregnant women to healthy non- & Clot formation time (CFT): Time from initiation pregnant female controls and clearly demonstrated the of clotting until a clot firmness of 20 mm is hypercoaguable state of normal pregnancy. Although detected (seconds) it was concluded that ROTEM could be a helpful ad- & > angle: Angle between the line in the middle of junct to conventional laboratory testing in reducing the TEM tracing and the line tangential to the delays in instituting appropriate treatment, reference developing ‘‘body’’ of the TEM (degrees) values for pregnant women were lacking. Huissoud & Maximum clot firmness (MCF): Firmness of the et al73 showed a significant increase in MCF, clot clot (mm) amplitude at 5 seconds (CA5) and clot amplitude at & Maximum lysis (ML): Reduction of the clot 15 seconds (CA15) (INTEM, EXTEM, and FIBTEM) firmness after MCF in relation to MCF (%) in the second and third trimesters in healthy pregnant Different coagulation activators (reagents) are used women. This is again in concordance with and confirms to catalyze the process. In the INTEM assay Ca2+, the hypercoaguable state of pregnancy. The CT and phospholipids and ellagic acid are used to activate and clot lysis index at 30 (CLI30) do not change during assess the coagulation process via the intrinsic path- pregnancy. There is a significant correlation between way. Tissue factor is used in EXTEM assays for ac- thromboelastometric and conventional coagulation tivation and assessment of the extrinsic pathway. Besides TF, a platelet inhibitor (cytochalasin) is added to the blood sample in the FIBTEM assay to differentiate between platelet dysfunction and the fi- brin polymerization process. In APTEM, a fibrino- lysis inhibitor (aprotinin) is used together with TF to confirm or to rule out hyperfibrinolysis. Abnormali- ties can occur in 3 areas: 1. Initial clotting abnormality due to clotting factor deficiency: CT and CFT are prolonged and the angle of the curve is reduced. EXTEM and INTEM dif- Fig. 2. Result of ROTEM. Copyright © 2012 by Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
- 7. 432 Obstetrical and Gynecological Survey tests, and a strong correlation between fibrinogen to a control group from a preliminary study and showed concentration and clot amplitude in the FIBTEM that in ROTEM, the FIBTEM- clotting amplitudes were analysis was found. These data combined with the significantly lower in the PPH group compared with results of Charbit et al suggested that TEG could be the control group without abnormal bleeding. A used as a rapid diagnostic tool to detect a decrease in limitation of the publication is that it is not completely fibrinogen in cases of severe bleeding.63 clear at what time the blood samples were taken and Oudghiri et al74 defined reference values for TEM the degree of blood loss at that moment. A strong parameters in the postpartum period in uncomplicated and significant correlation between fibrinogen levels deliveries. As was previously shown, a strong corre- and the FIBTEM parameters is presented for the PPH lation between thromboelastometric and conventional group as well as for the control group. The fibrinogen coagulation parameters was found, especially be- threshold of 2 g/L corresponded to a CA5-FIBTEM of tween fibrinogen concentration and FIBTEM CA5. 6 mm and a CA15 of 8 mm, both with 100% sensi- Unfortunately, the study excluded women with PPH, tivity and with 87% and 84% specificity, respectively. making the data of uncertain applicability to that In an unpublished study by Dr Doucloy-Bouters group, and also lacked an adequate sample size. et al (expert meeting, Munich, April 2010), the cutoff values for the FIBTEM were evaluated at 30 minutes Dilution postpartum in a small number of women (12 PPH and The effect of dilution on thromboelastometric 30 controls). Again, it is not clear what the degree of parameters in both nonpregnant and pregnant women blood loss was at the time of the blood sample. Fi- has been studied. In pregnant women, most studies brinogen levels less than 4 g/L and MCF less than 19 were done before elective cesarean delivery, that is, mm were seen in 10 of 12 patients in the PPH group before the occurrence of any peripartal changes and and fibrinogen levels of 4 g/L or greater and MCF before the onset of any blood loss. Butwick and greater than 19 mm in 25 of 30 patients in the control Carvalho75 demonstrated that preloading with 500 mL group, which led them to conclude that one must be of HES resulted in mild coagulation effects in R and aware of the risk of PPH when the fibrinogen level is K time when measured with TEG, whereas no effect less than 4 g/L or FIBTEM MCF is less than 19 mm. was observed after preloading with 1500 mL of lac- Furthermore, fibrinogen values less than 2 g/L and tated Ringer’s solution. Turker et al76 showed a mild correlating MCF values lower than 12 mm may be hypocoaguable effect on TEG parameters (shorter R high-risk cases. time and lower MA, the > angle was only significantly Another small study by Bauters et al80 compared decreased after preloading with HES) in healthy laboratory results of 23 patients with PPH and 31 parturients after preload with HES or succinylated women without PPH. They defined PPH as blood loss gelatin before elective cesarean delivery, although the more than 800 mL, and the first blood sample was results were not significant. Ansari and Riad77 dem- obtained at the moment of diagnosis, another sample onstrated that in vitro dilution to 60% with lactated was obtained 2 hours later. In patients with PPH, they Ringer’s or lactated Ringer’s solution/HES causes observed a decrease in FIBTEM A15 values 2 hours significant changes in all coagulation parameters earlier than the decrease in fibrinogen, suggesting a measured by TEM, with the latter solution causing a coagulopathy that was confirmed 2 hours later by fi- more pronounced effect. brinogen decrease. There are no studies available in PPH patients that assess or define cutoff values that can be used for Use of TEG or ROTEM in guiding therapy. The lack of predefined TEG/TEM Obstetric Hemorrhage target values hampers its routine use in the clinical A number of studies have assessed the utility of setting. Testing without proper guidance on how to TEG or metric testing in pregnancy. Butwick et al78 interpret the results can therefore not be recom- assessed the correlation between TEG parameters and mended outside a research setting. blood loss in elective cesarean delivery. They showed a weak association between clot strength (maximum Limitations amplitude) and blood loss and a modest reduction in the degree of maternal hypercoagulability in the early As with any laboratory test, TEG and ROTEM postpartum period. have some limitations. Adequate training and quality In a prospective observational study focused on controls are required for the successful performance PPH, Huissoud et al79 compared 51 women with PPH of these tests. Furthermore, thromboelastometric tests Copyright © 2012 by Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
- 8. Obstetric Hemorrhage and Coagulation: Update & CME Review Article 433 are not useful in patients on platelet aggregation in- 2) study different cutoff values for intervention to de- hibitor treatment. The added coagulation activators termine whether treatment should start at FIBTEM induce thrombin formation, which may conceal the (with correlating fibrinogen levels) for nonpregnant extent of inhibition of antithrombotic medication on subjects or at lower values for pregnant women, and platelet aggregation.81 Thus, it is not possible to dis- 3) study the effectiveness and the cost-effectiveness criminate between thrombocytopenia and disorders of of TEG/ROTEMYbased care compared with cur- platelet function.82,83 Also, treatment with fibrinogen rent care in PPH. may increase MCF in INTEM and EXTEM and dis- guise thrombocytopenia.84 Another limitation is temperature. Both TEG and REFERENCES TEM analyses are routinely performed at 37-C; therefore, the effect of hypothermia might not be 1. World Health Organisation. The World Health Report 2005VMake Every Mother and Child Count. Geneva, recognized and may be left untreated.85,86 Finally, Switzerland: World Health Organisation; 2005. fibrinogen is a well-known acute phase protein, which 2. Berg C, Harper M, Atkinson S, et al. Preventability of is also important in cases of PPH. However, to what pregnancy-related deaths: results of a state-wide review. Obstet Gynecol. 2005;106:1228Y1234. extent the FIBTEM is influenced by acute-phase 3. Schutte J, Steegers E, Schuitemaker N, et al. Rise in maternal proteins is not known. mortality in the Netherlands. Br J Obstet Gynaecol. 2010;117:399Y406. 4. American College of Obstetricians and Gynecologists. ACOG Practice Bulletin: Clinical Management Guidelines for Obstetrician-Gynecologists Number 76, October 2006: CONCLUSIONS postpartum hemorrhage. Obstet Gynecol. 2006;108: 1039Y1047. Conventional coagulation tests are time-consuming 5. McLintock C. Obstetric haemorrhage. Thromb Res. 2009; 123(suppl 2):S30YS34. and inefficient in acute situations and cannot predict 6. Leduc D, Senikas V, Lalonde AB, et al. Active management of the course of massive blood loss. As a consequence, the third stage of labour: prevention and treatment of in many cases, uncontrolled administration of blood postpartum hemorrhage. J Obstet Gynaecol Can. 2009;31: 980Y993. products occurs, which may be risky and expensive. 7. Wise A, Clark V. Strategies to manage major obstetric In contrast, TEG and TEM are rapid tests that can help haemorrhage. Curr Opin Anaesthesiol. 2008;21:281Y287. differentiate potential causes of hemostatic failure. 8. Ahonen J, Stefanovic V, Lassila R. Management of post- partum haemorrhage. Acta Anaesthesiol Scand. Results of TEM correlate well with conventional lab- 2010;54:1164Y1178. oratory results. As with conventional laboratory tests, 9. Knight M, Callaghan WM, Berg C, et al. Trends in postpartum there is an influence of fluid dilution on coagulation hemorrhage in high resource countries: a review and recommendations from the International Postpartum Hemorrhage test results, which is more pronounced when colloid Collaborative Group. BMC Pregnancy Childbirth. 2009;9:55. fluids are administered. FIBTEM values decline ear- 10. Theusinger OM, Spahn DR, Ganter MT. Transfusion in trauma: lier than fibrinogen levels do in women with PPH. why and how should we change our current practice? Curr Opin Anaesthesiol. 2009;22:305Y312. Although there are some data regarding the use of 11. Spalding G, Hartrumpf M, Sierig T, et al. Cost reduction of TEG and ROTEM in pregnant women, knowledge of perioperative coagulation management in cardiac surgery: normal reference values is lacking or incomplete. value of ‘bedside’ thrombelastography (ROTEM). Eur J Cardiothorac Surg. 2007;31:1052Y1057. Although TEG and TEM are promising tests to guide 12. Innerhofer P, Streif W, Kuhbacher G, et al. Monitoring individual therapeutic strategies, either cutoff values of perioperative dilutional coagulopathy using the ROTEM have not been defined or therapeutic intervention has analyzer: basic principles and clinical examples [in German]. Anasthesiol Intensivmed Notfallmed Schmerzther. 2004; not been evaluated. 39:739Y744. The evidence available at this moment does not 13. Rossaint R, Bouillon B, Cerny V, et al. Management of bleeding support the use of TEG or TEM to screen for coag- following major trauma: an updated European guideline. Crit Care. 2010;14:R52. ulation disorders in healthy women to predict PPH. 14. Hoffman M, Monroe DM. Coagulation 2006: a modern view of Secondary coagulopathy as a consequence of PPH is hemostasis. Hematol Oncol Clin North Am. 2007;21:1Y11. often underestimated and therefore remains untreated. 15. Hoffman M. Remodeling the blood coagulation cascade. J Thromb Thrombolysis. 2003;16(1Y2):17Y20. Fibrinogen seems to play an important role in the 16. Smith SA. The cell-based model of coagulation. J Vet Emerg course of PPH and could be an early predictor on the Crit Care (San Antonio). 2009;19:3Y10. severity of PPH. 17. Abbassi-Ghanavati M, Greer LG, Cunningham FG. Pregnancy and laboratory studies: a reference table for clinicians. Obstet Future research should be directed to Gynecol. 2009;114:1326Y1331. 18. Cerneca F, Ricci G, Simeone R, et al. Coagulation and 1) establish normal values for TEG/ROTEM in un- fibrinolysis changes in normal pregnancy. Increased levels of complicated deliveries, procoagulants and reduced levels of inhibitors during Copyright © 2012 by Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
- 9. 434 Obstetrical and Gynecological Survey pregnancy induce a hypercoagulable state, combined with a are risk factors for severe postpartum hemorrhages. J Thromb reactive fibrinolysis. Eur J Obstet Gynecol Reprod Biol. Haemost. 2008;6:2067Y2074. 1997;73:31Y36. 41. Chee YL, Crawford JC, Watson HG, et al. Guidelines on the 19. Franchini M. Post-partum hemorrhage: new therapeutic assessment of bleeding risk prior to surgery or invasive options [in Italian]. Recenti Prog Med. 2007;98:7Y11. procedures. British Committee for Standards in Haematology. Br 20. Szecsi PB, Jorgensen M, Klajnbard A, et al. Haemostatic J Haematol. 2008;140:496Y504. reference intervals in pregnancy. Thromb Haemost. 2010; 42. Fries D, Innerhofer P, Schobersberger W.. Time for changing 103:718Y727. coagulation management in trauma-related massive 21. Choi J, Pai S. Tissue plasminogen activator levels change with bleeding. Curr Opin Anaesthesiol. 2009;22:267Y274. plasma fibrinogen concentrations during pregnancy. Ann 43. Kozek-Langenecker SA. Effects of hydroxyethyl starch Hematol. 2002;81:611Y615. solutions on hemostasis. Anesthesiology. 2005;103:654Y660. 22. Francalanci I, Comeglio P, Liotta AA, et al. D -Dimer 44. Westphal M, James MF, Kozek-Langenecker S, et al. concentrations during normal pregnancy, as measured by Hydoxylethyl starches. Anesthesiology. 2009;111:187Y202. ELISA. Thromb Res. 1995;78:399Y405. 45. Mittermayr M, Streif W, Haas T, et al. Hemostatic changes after 23. O’Riordan MN, Higgins JR. Haemostasis in normal and crystalloid od colloid fluid administration during major abnormal pregnancy. Best Pract Res Clin Obstet Gynaecol. orthopedic surgery: the role of fibrinogen administration. 2003;17:385Y396. Anesth Analg. 2007;105:905Y917. 2 4 . Fr a n c a l a n c i I , C o m e g l i o P , L i o t t a A , e t a l . D - D i m e r 46. Mittermayr M, Streif W, Haas T, et al. Effect of colloid and concentrations durig normal pregnancy, as measured by crystalloid solutions on endogenous activation of fibrinolysis ELISA. Thromb Res. 1995;78:399Y405. and resistance of polymerized fibrin to recombinant tissue 25. Kline J, Williams G, Hernandez-Nino J. D-Dimer concentrations plasmingen activator added ex vivo. Br J Anaesth. 2008; in normal pregnancy: new diagnostic thresholds are needed. 100:307Y314. Clin Chem. 2005;51:825Y829. 47. Spahn DR, Rossaint R. Coagulopathy and blood component 26. MacPhail S, Talks K. Massive post-partum haemorrhage and transfusion in trauma. Br J Anaesth. 2005;95:130Y139. management of disseminated intravascular coagulation. Curr 48. Cosgriff N, Moore EE, Sauaia A, et al. Predicting life-threatening Obstet Gynaecol. 2004;14:123Y131. coagulopathy in the massively transfused trauma patient: 27. Hamilton-Davies C, Mythen MG, Salmon JB, et al. Comparison hypothermia and acidoses revisited. J Trauma. 1997;42:857Y861; of commonly used clinical indicators of hypovolaemia with discussion 861Y862. gastrointestinal tonometry. Intensive Care Med. 1997;23: 49. Kitchens CS. To bleed or not to bleed? Is that the question for 276Y281. the PTT? J Thromb Haemost. 2005;3:2607Y2611. 28. Stafford I, Dildy GA, Clark SL, et al. Visually estimated and 50. Schols SE, Lance MD, Feijge MA, et al. Impaired thrombin calculated blood loss in vaginal and cesarean delivery. Am J generation and fibrin clot formation in patients with dilutional Obstet Gynecol. 2008;199:519.e1Y519.e7. coagulopathy during major surgery. Thromb Haemost. 29. Johansson PI, Ostrowski SR, Secher NH. Management of 2010;103:318Y328. major blood loss: an update. Acta Anaesthesiol Scand. 51. Zink KA, Sambasivan CN, Holcomb JB, et al. A high ratio of plasma 2010;54:1039Y1049. and platelets to packed red blood cells in the first 6 hours of 30. Spahn DR, Cerny V, Coats TJ, et al. Management of bleeding massive transfusion improves outcomes in a large multicenter following major trauma: a European guideline. Crit Care. 2007; study. Am J Surg. 2009;197:565Y570; discussion 570. 11:R17. 52. Duchesne JC, Hunt JP, Wahl G, et al. Review of current blood 31. Burtelow M, Riley E, Druzin M, et al. How we treat: management transfusions strategies in a mature level I trauma center: were of life-threatening primary postpartum hemorrhage with a we wrong for the last 60 years? J Trauma. 2008;65:272Y276; standardized massive transfusion protocol. Transfusion. 2007; discussion 276Y278. 47:1564Y1572. 53. Duchesne JC, Islam TM, Stuke L, et al. Hemostatic resuscitation 32. Al Kadri HM. Obstetric medical emergency teams are a step during surgery improves survival in patients with traumatic- forward in maternal safety! J Emerg Trauma Shock. 2010;3: induced coagulopathy. J Trauma. 2009;67:33Y37; discussion 337Y341. 37Y39. 33. Merien AE, van de Ven J, Mol BW, et al. Multidisciplinary 54. Reid RW, Zimmerman AA, Laussen PC, et al. The efficacy of team training in a simulation setting for acute obstetric tranexamic acid versus placebo in decreasing blood loss in emergencies: a systematic review. Obstet Gynecol. 2010; pediatric patients undergoing repeat cardiac surgery. Anesth 115:1021Y1031. Analg. 1997;84:990Y996. 34. Howell C, Grady K, Cox C, eds. The MOET Course Manual: 55. Dryden PJ, O’Connor JP, Jamieson WR, et al. Tranexamic acid Managing Obstetric Emergencies and Trauma. 2nd ed. reduces blood loss and transfusion in reoperative cardiac London, UK: RCOG Press; 2009. surgery. Can J Anaesth. 1997;44:934Y941. 35. Skupski DW, Lowenwirt IP, Weinbaum FI, et al. Improving 56. Lethaby A, Farquhar C, Cooke I. Antifibrinolytics for heavy hospital systems for the care of women with major obstetric menstrual bleeding. Cochrane Database Syst Rev. 2000; hemorrhage. Obstet Gynecol. 2006;107:977Y983. (4):CD000249. 36. Varatharajan L, Chandraharan E, Sutton J, et al. Outcome of the 57. Novikova N, Hofmeyr GJ. Tranexamic acid for preventing management of massive postpartum hemorrhage using the postpartum haemorrhage. Cochrane Database Syst Rev. algorithm ‘‘HEMOSTASIS.’’ Int J Gynaecol Obstet. 2011;113: 2010;(7):CD007872. 152Y154. 58. Shakur H, Elbourne D, Gulmezoglu M, et al. The WOMAN trial 37. James AH. More than menorrhagia: a review of the obstetric (World Maternal Antifibrinolytic trial): tranexamic acid for the and gynaecological manifestations of bleeding disorders. treatment of postpartum haemorrhage: an international Haemophilia. 2005;11:295Y307. randomised, double blind placebo controlled trial. Trials. 38. James AH, Jamison MG. Bleeding events and other complications 2010;11:40. during pregnancy and childbirth in women with von Willebrand 59. Mercier FJ, Bonnet MP. Use of clotting factors and other disease. J Thromb Haemost. 2007;5:1165Y1169. prohemostatic drugs for obstetric hemorrhage. Curr Opin 39. Al-Zirqi I, Vangen S, Forsen L, et al. Prevalence and risk factors Anaesthesiol. 2010;23:310Y316. of severe obstetric haemorrhage. BJOG. 2008;115:1265Y1272. 60. Levi M, Levy JH, Andersen HF, et al. Safety of recombinant 40. Chauleur C, Cochery-Nouvellon E, Mercier E, et al. Some activated factor VII in randomized clinical trials. N Engl J hemostasis variables at the end of the population distributions Med. 2010;363:1791Y1800. Copyright © 2012 by Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
- 10. Obstetric Hemorrhage and Coagulation: Update & CME Review Article 435 61. Pacheco LD, Saade GR, Gei AF, et al. Cutting-edge advances preloading on thromboelastography prior to cesarean in the medical management of obstetrical hemorrhage. Am J delivery. Can J Anaesth. 2007;54:190Y195. Obstet Gynecol. 2011;205:526Y532. 76. Turker G, Yilmazlar T, Mogol EB, et al. The effects of colloid 62. Ickx BE. Fluid and blood transfusion management in obstetrics. pre-loading on thromboelastography prior to caesarean Eur J Anaesthesiol. 2010;27:1031Y1035. delivery: hydroxyethyl starch 130/0.4 versus succinylated 63. Charbit B, Mandelbrot L, Samain E, et al. The decrease of gelatine. J Int Med Res. 2011;39:143Y149. fibrinogen is an early predictor of the severity of postpartum 77. Ansari T, Riad W. The effect of haemodilution with 6% hemorrhage. J Thromb Haemost. 2007;5:266Y273. hydroxyethyl starch (130/0.4) on haemostasis in pregnancy: 64. Gayat E, Resche-Rigon M, Morel O, et al. Predictive factors of an in-vitro assessment using thromboelastometry. Eur J advanced interventional procedures in a multicentre severe Anaesthesiol. 2010;27:304Y305. postpartum haemorrhage study. Intensive Care Med. 2011; 78. Butwick A, Ting V, Ralls LA, et al. The association between 37:1816Y1825. thromboelastographic parameters and total estimated blood 65. Bell SF, Rayment R, Collins PW, et al. The use of fibrinogen loss in patients undergoing elective cesarean delivery. concentrate to correct hypofibrinogenaemia rapidly during Anesth Analg. 2011;112:1041Y1047. obstetric haemorrhage. Int J Obstet Anesth. 2010;19:218Y223. 79. Huissoud C, Carrabin N, Audibert F, et al. Bedside assessment 66. Kozek-Langenecker S, Sorensen B, Hess J, et al. Clinical of fibrinogen level in postpartum haemorrhage by effectiveness of fresh frozen plasma compared with fibrinogen thrombelastometry. BJOG. 2009;116:1097Y1102. concentrate: a systematic review. Crit Care. 2011;15:R239. 80. Bauters A, Ducloy-Bouthors A, Lejeune C, et al. ROTEM 67. Available at: http://www.haemonetics.com. thromboelastometry in obstetric: near patient-test as an early 68. Luddington RJ. Thrombelastography/thromboelastometry. predictor of post-partum hemorrhage (PPH). J Thromb Clin Lab Haematol. 2005;27:81Y90. Haemost. 2007;5(suppl 2). Abstract P-S-220. 69. Available at: http://www.rotem.de/. 81. Swallow RA, Agarwala RA, Dawkins KD, et al. Thromboelastography: 70. Polak F, Lips M, Bedrichova H, et al. The use of thrombelastography potential bedside tool to assess the effects of antiplatelet in evaluation of coagulation in females with physiological or therapy? Platelets. 2006;17:385Y392. pathological gravidity [in Czech]. Cas Lek Cesk. 2007; 82. Larsen OH, Fenger-Eriksen C, Christiansen K, et al. Diagnostic 146:396Y400. performance and therapeutic consequence of thromboelastometry 71. Sharma SK, Philip J, Wiley J. Thromboelastographic changes activated by kaolin versus a panel of specific reagents. in healthy parturients and postpartum women. Anesth Analg. Anesthesiology. 2011;115:294Y302. 1997;85:94Y98. 83. Scharbert G, Auer A, Kozek-Langenecker S. Evaluation of the 72. Armstrong S, Fernando R, Ashpole K, et al. Assessment of platelet mapping assay on rotational thromboelastometry coagulation in the obstetric population using ROTEM ROTEM. Platelets. 2009;20:125Y130. thromboelastometry. Int J Obstet Anesth. 2011;20:293Y298. 84. Lang T, Johanning K, Metzler H, et al. The effects of fibrinogen 73. Huissoud C, Carrabin N, Benchaib M, et al. Coagulation levels on thromboelastometric variables in the presence of assessment by rotation thrombelastometry in normal thrombocytopenia. Anesth Analg. 2009;108:751Y758. pregnancy. Thromb Haemost. 2009;101:755Y761. 85. Johansson PI, Stissing T, Bochsen L, et al. Thrombelastography 74. Oudghiri M, Keita H, Kouamou E, et al. Reference values for and tromboelastometry in assessing coagulopathy in trauma. rotation thromboelastometry (ROTEM) parameters following Scand J Trauma Resusc Emerg Med. 2009;17:45. non-haemorrhagic deliveries. Correlations with standard 86. Douning LK, Ramsay MA, Swygert TH, et al. Temperature haemostasis parameters. Thromb Haemost. 2011;106:176Y178. corrected thrombelastography in hypothermic patients. 75. Butwick A, Carvalho B. The effect of colloid and crystalloid Anesth Analg. 1995;81:608Y611. Copyright © 2012 by Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.