

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a 12 22-2012 depression-2
Similar a 12 22-2012 depression-2 (20)
Más de Chau Nguyen
Más de Chau Nguyen (20)
12 22-2012 depression-2
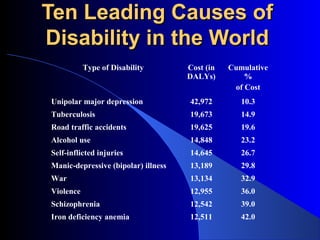
- 1. Ten Leading Causes of Disability in the World Type of Disability Cost (in Cumulative DALYs) % of Cost Unipolar major depression 42,972 10.3 Tuberculosis 19,673 14.9 Road traffic accidents 19,625 19.6 Alcohol use 14,848 23.2 Self-inflicted injuries 14,645 26.7 Manic-depressive (bipolar) illness 13,189 29.8 War 13,134 32.9 Violence 12,955 36.0 Schizophrenia 12,542 39.0 Iron deficiency anemia 12,511 42.0
- 2. Episode Disorder *Major depression episode *Major depression disorder *Major depression episode+ *Bipolar disorder, Type I manic/mixed episode *Manic/mixed episode *Bipolar disorder, Type I *Major depressive episode+ *Bipolar disorder, Type II hypomanic episode *Chronic subsyndromal *Dysthymic Disorder depression *Chronic fluctuations between subsyndromal *Cyclothymic disorder depression & hypomania
- 3. “If I had __________, I’d be depressed to.”
- 4. Definitions • Mood - a person’s sustained emotional state • Affect – the outward manifestation of a person’s feelings, tone, or mood
- 5. Major Depression • Syndromal classification with disturbances of mood, neurovegetative and cognitive functioning
- 6. Major Depression At least 5 of the following symptoms present for at least 2 weeks (either #1 or #2 must be present): 1) depressed mood 2) anhedonia – loss of interest or pleasure 3) change in appetite 4) sleep disturbance
- 7. Major Depression 5) psychomotor retardation or agitation 6) decreased energy 7) feeling of worthlessness or inappropriate guilt 8) diminished ability to think or concentrate 9) recurrent thoughts of death or suicidal ideation
- 8. Major Depression • Symptoms cause marked distress and/or impairment in social or occupational functioning. • No evidence of medical or substance- induced etiology for the patient’s symptoms. • Symptoms are not due to a normal reaction to the death of a loved one.
- 9. Bereavement and Late Life Depression • 25 – 35% of widows/widowers meet diagnostic criteria for major depressive disorder at 2 months. • ~15% of widows/widowers meet diagnostic criteria for major depressive disorder at one year. • This figure remains stable throughout the second year.
- 10. Subtypes of Depression • Atypical Reverse neurovegetative symptoms Mood reactivity Hypersensitivity to rejection MAO-I’s and SSRI’s are more effective treatments
- 11. Subtypes of Depression Psychotic (~10% of all MDD) • Delusions common, may have hallucinations • Delusions usually mood congruent • Combined antidepressant and antipsychotic therapy or ECT is necessary
- 12. Subtypes of Depression Melancholic • No mood reactivity • Anhedonia • Prominent neurovegetative disturbance • More likely to respond to biological treatments
- 13. Subtypes of Depression Seasonal • Onset in Fall, remission in Spring • Hypersomnia is typical • Less responsive to medications • A.M. light therapy (>2,500 lux) is effective
- 14. Subtypes of Depression Catatonic • Motoric immobility (catalepsy) • Mutism • Ecolalia or echopraxia
- 15. Epidemiology Point prevalence 6 – 8% in women 3 – 4% in men Lifetime prevalence 20% in women 10% in men
- 16. Epidemiology Age of Onset Throughout the life cycle, typically from the mid 20’s through the 50’s with a peak age of onset in the mid 30’s
- 17. Epidemiology Genetics More prevalent in first degree relatives 3-5x the general population risk Concordance is greater in monozygotic than dizygotic twins Increased prevalence of alcohol dependence in relatives
- 18. Etiology Original, clearly over simplistic theories regarding norepinephrine and serotonin Deficiency states depression States of excess mania
- 19. Problems with initial theories Inconsistentfindings when studying measures of these systems: MHPG (3 methoxy 4 hydroxyphenolglycol) and 5HIAA (5 hydroxy indoleacetic acid) in the urine and CSF. Treatments block monoamine uptake acutely, however the positive effects occur in 2-4 weeks.
- 21. Receptor theory more useful Antidepressant treatment causes a down regulation in central adrenergic and serotonergic receptors – This change corresponds temporally to the antidepressant response
- 22. Neuroendocrine Hyperactivity of HPA axis: – Elevated cortisol – Nonsuppression of cortisol following dexamethasone – Hypersecretion of CRF Blunting of TSH response to TRH Blunting of serotonin mediated increase in plasma prolactin Blunting of the expected increase in plasma growth hormone response to alpha-2 agonists
- 23. Functional Neuroimaging (PET,SPECT) demonstrates decreased metabolic activity in Dorsal prefontal cortex – Anterolateral (concentration, cognitive processing) – Cingulate (regulation of mood and affect) Subcortical – Caudate (psychomotor changes)
- 25. Psychosocial Risk Factors – Poor social supports – Early parental loss – Introversion – Female gender – Recent stressor (especially medical illness)
- 26. Psychosocial Cognitive Theory – Patients have distorted perceptions and thoughts of themselves, the world around them and the future Possible to treat by restructuring
- 27. Secondary Causes of Depression Toxic Endocrine Vascular Neurologic Nutritional Neoplastic Traumatic Infectious Autoimmune
- 28. Depression – Differential Diagnosis Other Mood Disorders Adjustment Disorder with Depressed Mood – Maladaptive and excessive response to stress, difficulty functioning, need support not medicines, resolve as stress resolves – Dysthymic Disorder – Bipolar Disorder Other Psychotic Disorders – if psychotic subtype Personality Type – “glass is half empty type” overall pessimistic, depressed outlook. Chronic and longstanding with no change in function.
- 30. Treatment Biologic Tricylclic antidepressants Monoamine oxidase inhibitors Second generation antidepressants – SSRI’s, Venlafaxine, bupropion, martazapine Electoconvulsive therapy
- 31. Treatment Psychosocial Treatments Education Specific pscychotherapies Vocational training Exercise
- 32. Treatment When to Refer? Question regarding suicide risk Presence of psychotic symptoms Past history of mania Lack of response to adequate medication trial
- 33. Treatment Course One episode – 50% chance of reoccurence Two episodes – 70% chance of reoccurence Three or more episodes - >90% chance of reoccurence
- 34. Dysthymic Disorder Characteristics Chronically depressed mood for most of the day, more days than not, for at least two years. Can be irritable mood in children and adolescents for 1 year While depressed, presence of at least two of the following – Poor appetite or overeating – Sleep disturbance – Low energy or fatigue – Low self esteem – Poor concentration – Feelings of hopelessness
- 35. Dysthymic Disorder Never without depressive symptoms for over 2 months No evidence of an unequivocal Major Depressive Episode during the first two years of the disturbance (1 year in children and adolescents) No manic or hypermanic episodes Not superimposed on a chronic psychotic disorder Not due to the direct physiologic affects of a substance or a general medical condition
- 36. Epidemiology More prevalent in women, 4% prevalence in women, 2% in men Onset is usually in childhood, adolescence or early adulthood Often is a superimposed Major Depression High prevalence of substance abuse in this group
- 37. Differential Diagnosis Other mood disorders Mood disorder due to a general medical condition
- 38. Treatment Ifno superimposed Major Depression – Psychotherapy Some evidence suggest responsiveness to antidepressant medication
- 39. Course Prognosis is not as good as Major Depression in terms of total symptoms remission
- 41. Bipolar Disorder Characteristics of a Manic Episode A distinct period of abnormally and persistently elevated, expansive or irritable mood During the period of mood disturbance, at least three of the following symptoms have persisted (four if the mood is only irritable) and have been persistent to a significant degree – Inflated self esteem or grandiosity – Decreased need for sleep – More talkative than usual or pressure to keep talking – Flight of ideas or subjective experience that thoughts are racing
- 42. Characteristics (Cont.) – Distractability, i.e. attention too easily drawn to unimportant or irrelevant external stimuli – Increase in goal-directed activity or psychomotor agitation – Excessive involvement in pleasurable activities which have a high potential for painful consequences, e.g. unrestrained buying sprees, sexual indiscretions, or foolish business investments
- 43. Characteristics (Cont.) Mood disturbance sufficiently severe to cause marked impairment in occupational functioning or in usual social activities or relations with others, or to necessitate hospitalization to prevent harm to self or others At no time during the disturbance have there been delusions or hallucinations for as long as two weeks in the absence of prominent mood symptoms Not superimposed on schizophrenia, schizophreniform disorder, or delusional disorder or psychotic disorder NOS The disturbance is not due to the physiologic effects of a substance or general medical disorder
- 44. Presentations of Bipolar Disorder Manic Depressed Mixed
- 45. Types TypeI - manic/mixed episode +/- major depressive episode TypeII - hypomanic episode + major depressive episode
- 46. Epidemiology Lifetime prevalence Type I - 0.7 - 0.8% Type II - 0.4 - 0.5% – Equal in males and females – Increased prevalence in upper socioeconomic classes Age of Onset – Usually late adolescence or early adulthood. However some after age 50. Late onset is more commonly Type II.
- 47. Genetics Greaterrisk in first degree relatives (4-14 times risk) Concordance in monozygotic twins >85% Concordance in dyzygotic twins – 20%
- 48. Secondary Causes of Mania Toxins Drugs of Abuse – Stimulants (amphetamines, cocaine) – Hallucinogens (LCD, PCP) Prescription Medications – Common: antidepressants, L-dopa, corticosteroids Neurologic Right-sided CVA Right frontotemporal tumors Huntington’s Disease Multiple Sclerosis
- 49. Secondary Causes of Mania (Cont.) Infectious Neurosyphilis HIV Endocrine Hypothyroidism Cushing’s Disease Cyclothymic Disorder Other Psychotic Disorders
- 50. Treatment Education and Support Medication 1. Lithium 2. Carbamazepine 3. Valproate 4. Lamotrigine 5. ECT
- 51. Course Acute Episode – Manic - 5 weeks – Depressed - 9 weeks – Mixed - 14 weeks Long Term – Variable - most cover fully – Mean number of lifetime episodes 8-9
- 52. Cyclothymic Disorder Characteristics For at least two years (one for children and adolescents) presence of numerous Hypomanic Episodes and numerous periods with depressed mood or loss of interest or pleasure that did not meet criterion A of a Major Depressive Episode During a two year period (one year in children and adolescents) of the disturbance, never without hypomanic or depressive symptoms for more than a two month time
- 53. Characteristics (Cont.) No clear evidence of a Major Depressive Disorder, or Manic Episode during the first two years of the disturbance (or one year for children and adolescents) Not superimposed on a chronic psychotic disorder, such as schizophrenia or Delusional Disorder Not due to the direct physiologic affects of a substance or a general medical condition
- 54. Epidemiology Lifetimeprevalence 0.4 – 1.0 % same for males and females Age of onset – Usually in adolescence or early adulthood Genetics – Major Depression and Bipolar Disorder more common in first degree relatives
- 55. Cyclothymic Disorder Secondary causes of cyclothymic disorder Bipolar Disorder Mood disorders due to a general medical condition Treatment Initiationof biologic treatment is dependent on the degree of impairment If treatment is indicated, it is similar to that of Bipolar Disorder
- 56. Episode Disorder *Major depression episode *Major depression disorder *Major depression episode+ *Bipolar disorder, Type I manic/mixed episode *Manic/mixed episode *Bipolar disorder, Type I *Major depressive episode+ *Bipolar disorder, Type II hypomanic episode *Chronic subsyndromal *Dysthymic Disorder depression *Chronic fluctuations between subsyndromal *Cyclothymic disorder depression & hypomania