
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a cardiopulmonary bypass
Similar a cardiopulmonary bypass (20)
Último
Último (20)
cardiopulmonary bypass
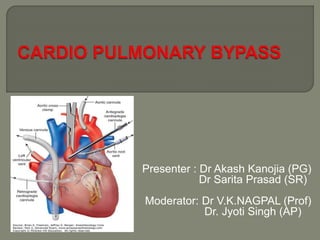
- 1. Presenter : Dr Akash Kanojia (PG) Dr Sarita Prasad (SR) Moderator: Dr V.K.NAGPAL (Prof) Dr. Jyoti Singh (AP)
- 2. CPB is a technique that diverts venous blood away from the heart (most often from one or more cannulas in the right atrium), adds oxygen, removes CO2 , and returns the blood through a cannula in a large artery (usually the ascending aorta). As a result, nearly all blood bypasses the heart and lungs.
- 3. The first successful open heart procedure on a human using bypass machine was performed by John Gibbon on May 6, 1953 in Philadelphia. The operation was correction of an ASD on an 18 years old girl.
- 5. • To provide a stilled bloodless heart with blood flow temporarily diverted to an extra corporeal circuit that functionally replaces the heart and lungs. • Respiration Ventilation Oxygenation • Circulation. • Temperature regulation
- 6. Even though perfusionist is responsible for the safe conduct of CPB, the anesthesiologist is particularly responsible for:- Acid base management Anticoagulation maintenance Delivery of cardioplegia Maintenance of arterial pressure (use of vasodilators, vasoconstrictors) Use of inhalational agents Cerebral protection, especially when deep hypothermia and circulatory arrest are employed.
- 7. Coronary Artery Disease (CAD) Valve Disease Congenital Heart Defects Aneurysms :-Aortic, ventricular, giant cerebral Transplants :- Heart, lung.
- 8. Venous cannula. Aortic cannula. Blood reservoir. Oxygenators. Heat Exchanger. Arterial Pump. Filters. Circuits. Accessory Devices. Cardiotomy Suction LV vent Cardioplegic Pump. Ultra-Filter. Prime
- 11. Drains blood from patient into the CPB circuit. One or two cannula are used, depending on the type of cardiac surgical procedure or surgeons preference. Drain blood by the effect of gravity.
- 12. These cannula return the blood from the CPB circuit to the patient. Commonly ascending aorta is cannulated. Axillary or femoral artery can be used in cases of :- Dissecting aortic aneurisms. Patients who require re-operation. In emergencies.
- 13. This stores the blood. It provides a 5-10 second reserve of blood in case venous return is temporarily interrupted. Two type: Venous reservoir Arterial reservoir.
- 14. It is an apparatus where O2 and Co2 exchange takes place. Types Bubble oxygenator Membrane oxygenator
- 16. Used when CPB is needed for less than 2hours. O2 is directly infused into a column of systemic venous blood through a diffusion plate. Gas exchange occurs across a thin film at the blood gas interface around each bubble. Co2 diffuses into the bubble and O2 diffuses into the plasma. Co2 transfer is proportional to total gas flow O2 transfer is dependent on bubble size Advantages: Easy to assemble and operate Lower cost Need relatively small amount of priming solution. Disadvantages: Blood cell trauma Micro embolization of air and particular material Platelet destruction/ impaired platelet activity Denaturation of blood proteins.
- 17. Used when CPB is needed for more than 2-3 hours. Gas doesn't come in direct contact with the blood. A membrane, made up of silicon rubber or polypropylene or Teflon, separates blood and gas compartments. O2 tension is controlled by the FIO2 of the inspired gas and Co2 is regulated by total gas flow. Advantages: Less blood cell trauma Better platelet preservation Allows independent control of PaCO2 and PaO2 Decreased protein denaturation. Disadvantages: More expensive Canʼt tolerate perfusion pressures > 125mmHg and gas exchange capacity deteriorates after 5 hours of continuous use.
- 18. It adjusts the temperature of the perfusate to provide moderate systemic hypothermia during the period of cardiac repair and gradually rewarms the blood during the discontinuation of CPB. Water circulates within the heat exchanger in a counter current fashion to the flow of blood at temperatures between 1-2°C and 42°C. The temperature gradient between the water and blood is kept at 10°C or less and the water temperature is not allowed to exceed 42°C during the rewarming phase to avoid injury to blood proteins.
- 19. These are the devices used to generate the pressure required to return the perfusate to the patient. Types : Roller pump Centrifugal pump.
- 23. Filters Trap particulate matter and gaseous emboli. Sites: Suction line Arterial filter Circuits The tubings used in the circuit should have the following characteristics. Non-thrombogenic and chemically inert. Smooth internal finish with non-wettable luminal surface and low surface tension Durable enough to withstand the use of roller pump and high pressures on the arterial side. Polyvinyl chloride tubings.
- 24. Cardiotomy suction Aspirates the blood from the surgical field and returns it to the main pump reservoir and hence avoids blood losses. Excessive suction pressure can damage RBCs. A cell saver suction device which returns to a separate reservoir can also be used instead of cardiotomy suction.
- 25. Left ventricular vent Blood keeps on accumulating in the L.V, because of direct opening of thebasian veins and bronchial arteries into the L.V. Compromise myocardial preservation by removing cardioplegia solution and warming the myocardium. Blood is removed by a catheter inserted into the L.V via the right superior pulmonary vein and left atrium.
- 26. Cardioplegic pump • It provides optimal control over the cardioplegia infusion pressure and temperature. • Separate heat exchanger ensure accurate control of temperature of cardioplegia solution. Ultra-filter • Used to increase patient's hematocrit without blood transfusion. • Contain hollow semipermeable fibers, hydrostatic pressure force water and electrolytes across the membrane. • Effluent of up to 40ml/min can be removed.
- 27. It is the fluid used for priming of CPB circuit. Its composition should be close to that of ECF. The prime for most adult perfusions contains a balanced salt solution. Other components which are added are : Albumin or hetastarch (to increase oncotic pressure) Mannitol (to promote diuresis) Heparin Bicarbonate Calcium In neonates, children and adults with significant preoperative anemia, in whom profound haemodilution might decrease O2 carrying capacity; blood is used as priming solution. 1500-2000ml of prime is added to the patientʼs blood volume because of priming. This will lead to acute normovolaemic haemodilution. Hct of 20-30% is the acceptable limit. Blood is added if the Hct is < 25% after dilution.
- 28. CPB attempts to simulate the functions of the patients heart and lungs. But it is a complete departure from the normal circulation. The physiological effects of this are summarized as follows : 1. Circulation Cardiac output Systemic blood flow is controlled by the revolution of the pump. Optimal flow rates 2.2-2.5 lt/min/m2 in anesthetized, normothermic patients. The flow may be reduced by 7% for each degree Celsius decrease in body temperature as the BMR falls by 8% per degree Celsius decrease in body temperature. Arterial pressure wave The normal pulsatile flow replaced by non pulsatile flow. ABP controlled by flow rate and by infusion of peripheral vasodilators/ vasoconstrictors.
- 29. Systemic vascular resistance After the initial fall, SVR gradually rises to above normal levels. Changes in BP are mainly determined by SVR changes. Venous tone Gradually increases during CPB .
- 30. 2. Respiration • Lung is by passed. Ventilation done by oxygenator. Acceptable ABG values include PaO2 should be >85mmHg. pH = 7.4 PCO2 = 35-45mmHg. High inspired oxygen concentration and flow rate are required.
- 31. 3. Haemodilution Fall in the blood viscosity (Decrease Hct) Increase in the blood flow Ensures peripheral capillary circulation in body. Ensures uniform Hypothermia all over the body. O2 carrying capacity of the blood is reduced. Tissue hypoxia is not a problem if Hct > 20%. Dilutes blood constituents e.g., coagulation factors Volume of distribution of all drugs increases.
- 32. 4. Effects of hypothermia Decreased metabolic rate Decreased O2 requirement Increased blood viscosity For each degree decrease in temperature pH increase by 0.0147units Shift of ODC to the left. RS:↓ MV
- 33. CVS: ↓myocardial O2 uptake (MMRO2) ↓ BP ventricular dysrrhythmias. Liver:↓ metabolism, ↓ blood flow, ↑ coagulation time. Kidney:↓ blood flow, O2 consumption GFR (at later stages). CNS:↓ metabolism (CMRO2) Better tolerates Hypoxia.
- 34. Cooling techniques: Surface cooling - immersion (40C water) (for correction of cardiac abnormalities within 8min) Evaporation Cooling blanket Core cooling - extracorporeal circuit Monitoring: Heart temp: mid esophageal probe Brain temp: nasopharyngeal or tympanic membrane. Temperature gradient: rectal
- 35. Pre bypass preparations Initiating CPB Maintenance of extracorporeal circulation Weaning from CPB
- 36. The heart lung machine should be partially assembled 45-60min before bypass is scheduled to begin. The system is primed with priming solution and recirculated for several minutes through a sterile 0.5u filter to remove all air bubbles and particulate emboli from the system. The calculated flows are written down for easy reference. The patient positioned in trendlenberg position Anesthesia induced. The surgeon prepares the sites for arterial and venous cannulation.
- 37. Bypass circuits are thrombogenic, Systemic anticoagulation is a must before initiating bypass. Heparin 300-400U/kg or 2-3 mg/kg given into the central vein / directly into the right atrium. Activated clotting time is measured 2-5minutes later and additional heparin given as required. ACT for CPB = > 480 sec. Supplemental dose of heparin given every hourly at the dose of 1/3 - 1/2 of initial dose. Heparin top-ups – ACT value guided.
- 38. Heparin resistance is seen in : Ongoing active coagulation Antithrombin III deficiency Prior heparin therapy Drug interactions (OCPʼs) Drug error Advanced age IV nitroglycerin
- 39. Treatment: • Increase the dose of heparin up to 800U/kg • FFP to increase AT III levels. • Anti-Thrombin III concentrates. • Use Alternate Anticoagulants e.g. • Ancrod (cleaves fibrinogen) • Hirudin ( inhibit thrombin)
- 40. After full heparinization, cannulas are placed. Aortic cannula is usually placed first because, it is technically more difficult to do and after placement, the perfusionist can give additional volume via the arterial cannula to support the patients BP. The ascending aorta is most often used. Reduction of systemic BP to 90-100mm Hg systolic facilitates placement of aortic cannula. Once the aortic cannula is placed, it is then connected to the arterial tubing from the bypass machine and a careful search is done for any air bubbles left in the tubing. Even a small amount of air may lead to cerebral air embolus and cause neurological consequences.
- 41. Dopplar to confirm carotid flow. High arterial inline pressures may indicate, • Improper positioning of the arterial cannula or • Can be an initial warning sign of an aortic dissection Once the surgeon, perfusionist and anesthesiologist are satisfied with the functioning and placement of the aortic cannula, the venous cannula is then placed. Two cannula one in SVC and another in IVC or a single cannula in the right atrium are used. Single cannula often has 2 ports 1 in the RA and other in the IVC Placement of the venous cannula may be associated with episodes of hypotension that usually occur secondary to impaired venous return or an atrial arrhythmia. (PAC, Atrial fibrillation, SVT) Usually these situations resolve quickly without intervention, but occasionally IV medications, cardio version or the rapid placement of the patient on bypass may be necessary.
- 42. Calibrate all monitoring transducers Empty the bladder to accurately track urine output while on bypass Inspect the patientʼs eyes for Conjunctival edema and pupil size discrepancies. Anesthetic agents and adjuvants are supplemented to overcome the dilution effect of CPB and the consequent lightening of the anesthetic state.
- 43. Bypass begins when the surgeon unclamps the venous lines, and blood begins to enter the extracorporeal circuit. As the blood starts to fill up the venous reservoir of the oxygenator, the arterial pump is turned on. The perfusionist gradually increases the bypass flow rates until all systemic perfusion is machine generated. Addition doses of Narcotics, Sedative and Muscle relaxant are given to compensate dilutional effect. The TEE is turned off All IV fluids are turned off. Ventilation Turned off.
- 44. Hypotension - decrease >30mmHg • Treatment = vasoconstrictors, increase pump flow. Hypertension due to inadequate anesthesia/excessive vasoconstriction from elevated catecholamine levels. • Treatment: Decrease pump flow or add isoflurane/ vasodilator therapy. Inadequate venous drainage -because of catheter malposition /kink/airlock. Inadequate oxygenation Asymmetric swelling or discoloration of the face or eye indicating arterial cannula obstruction. Elevated inflow line pressures and dampened distal arterial pressures - indicate aortic dissection.
- 45. Elevated CVP due to • Inadequate venous drainage • Kinking of catheter. Air embolism • Inattention to venous reservoir levels • Failure by the perfusionist to act quickly enough to prevent air from being pumped into the arterial cannula.
- 46. Primary Goal Desired levels of hypothermia Attain Cardioplegia. Maintain Line pressure. Maintain adequate systemic perfusion Ensure appropriate tissue oxygenation Manage arterial blood gases. Maintain Anticoagulation.
- 47. Hypothermia of 20-30°C is routinely used for CPB. • Mild = 35-280C • Moderate = 21-270C • Deep = < 200C • Arrhythmias at 300C • Ventricular fibrillation at 280C • Apnea at 230C O2 consumption is reduced 5-7% per degree centigrade decrease in the temperature. 10°C drop in temperature will halve the BMR. Advantages: • Lower pump flow rates, • better organ protection, • less blood trauma • improved myocardial protection. Maintain uniform temperature during CPB. Avoid temperature gradients. ( two temperature probes)
- 48. To provide motionless field – heart is arrested in diastole. ↓ myocardial O2 consumption by 90% Substrate – Crystalloid/blood For initial arrest dose approximately 1000 to 1500 mL of “high-K” solution is used. Perfusion of the heart is suspended for a period of 10 to 40 minutes while the surgeon works on the heart. Then, periodically throughout the procedure, 200- to 500-mL doses of “low-K” solution are administered to deliver nutrients to the cells and maintain the potassium concentration.
- 50. Method of injection: Antegrade fashion- into the coronary arteries via the aortic root, through a needle placed between the aortic clamp and the aortic valve. Retrograde fashion- into the coronary veins, via a balloon-tipped cannula placed in the coronary sinus. Mechanism of action: Increased extracellular potassium ↓ Decrease in transmembrane potential ↓ Impairment of Na+ transport ↓ Abolition of action potential generation ↓ Cardiac arrest in diastole
- 51. Before CPB there is electrical activity on the EKG Pulsatile central venous flow. pulsatile arterial blood pressure. On CPB, the hearts electrical activity is suspended. Nonpulsatile arterial blood pressure . Non-pulsatile central venous pressure.
- 52. Acid base management during CPB is done by two methods Alpha stat method pH stat method
- 53. Alpha stat method • It considers the alkaline pH seen during CPB is physiological. • Increased solubility of carbon dioxide seen during hypothermia raises the pH. • No additional measures to correct the pH/ Pco2 levels are undertaken. • More commonly used method and it appears to preserve cerebral autoregulation & improve myocardial preservation. PH stat method • PH & Pco2 are maintained at normal values regardless of the body temperature. • In order to maintain Pco2, Co2 is added to the ventilating gas mixture. • This method is not preferred because patients tend to have higher CBF because of increase in Co2 content and there will be loss of cerebral auto regulation. • More flow, more chances of micro-embolization. • Recommended for pediatric surgery
- 54. A 50-60 ml/kg/min of flow rate maintains mean arterial pressure at 40-60 mmHg. To preserve CNS function MAP should be maintained >50mmHg. As the patient is re-warmed, the MAP should also be increased accordingly, to ensure adequate CBF. In patients with peripheral vascular diseases MAP should be maintained at 60mmHg with hypothermia. Renal function is maintained with pump flows of ≥ 1.6L/min.
- 55. Line pressure. Arterial pressure. CVP Temperatures. ECG Urine output Arterial Blood gases Mixed venous saturation (optional) Hematocrit Level of anticoagulation.
- 56. Line pressure: Higher pressures: • Kinking of circuit. • Awake patient. • Defective pump. Lower pressure: Failure of arterial pump. Leakage in circuit. Disconnected cannula.
- 57. Arterial pressure. Hypotension • Venous cannula—kink, malposition, clamp, air lock • Inadequate venous return (bleeding, hypovolemia, IVC obstruction,) • Pump—poor occlusion, low flows • Arterial cannula— misdirected, kinked, partially clamped,-dissection • Vasodilation—anesthetics, haemodilution, idiopathic • Transducer or monitor malfunction, stopcocks the wrong way Hypertension • Pump - ↑ flow • Arterial cannula—misdirected • Vasoconstriction—light anesthesia, response to temperature changes • Transducer or monitor malfunction
- 58. CVP Increased CVP = compromises cerebral circulation. Temperatures- Rectal and nasopharyngeal (near to brain temperature) ECG Should show a flat line that is complete absence of activity. Any electrical activity suggest need for cardioplegia top up. Urine output: maintained at or more than 1ml/kg/hr. It is an indirect evidence of organ perfusion. Blood gases and mixed venous Po2 are also monitored. Hematocrit monitoring: Should be maintained at 20-30%
- 59. Level of anticoagulation: To be monitored and maintained at optimal levels. The methods include, ACT (Activated Clotting Time) >480sec. High dose thrombin time (HITT) Thromboelastography: Gives information about the quality of the clot and dynamics of its formation. Heparin concentration: correlates with anti factor X a activity.
- 60. Goals of weaning. Re-warming Revived electrical activity of heart. Revived mechanical activity of heart. Restoration of spontaneous circulation. ABG management. Reversal of Anti-coagulation. Restarting ventilation.
- 61. • When the surgeon begins the last phase of the procedure, the perfusionist begins to rewarm the patient. • The rewarming should be done gradually. • Anesthesiologist should ensure amnesia of the patient by administering additional doses of benzodiazepines, as the amnesic effect of hypothermia is lost. • Avoid inhalational agents as they have negative inotropic property.
- 62. • Upon completion of the surgical repair, any residual air in the ventricles to be removed. • The anesthesiologist vigorously inflates the lungs to remove air from the pulmonary veins and aids in filling of the cardiac chambers. • TEE assesses the effectiveness of desiring process. • The aortic clamp removed to resume myocardial perfusion • The field is tidied up and preparations are made to separate from cardiopulmonary bypass.
- 63. Ensure adequate re-warming and myocardial contractility. If necessary, heart rate and rhythm can be regulated either pharmacologically/ electrically with appropriate pacing. Defibrillation is done by internal paddles with energy started at 2.5 joules and increased in 2.5 or 5 J increments. Rule out hyperkalemia and treat accordingly. Ventilation begun with 100%-O2 Blood and Blood products are transfused . Fluid replacement and inotropic support started.
- 64. Venous drainage lines are gradually occluded, allowing, arterial return to progressively raise the circulating volume. When sufficient volume has been transformed to optimize preload, blood pressure and cardiac output. Venous cannulas are removed following a satisfactory interval of stable hemodynamic functions.
- 65. Done with Protamine. At this point aortic cannula will be still present. 1-1.3mg of protamine per 100 units (1mg) of heparin is administered slowly over 5-10 mins Adv effects: hypotension, bronchospasm, rash, or anaphylaxis. Continue protamin infusion till ACT return to baseline value. Arterial cannulas remain in place for continued transfusion of pump contents. When this is completed and bleeding is controlled, the arterial cannula is removed and the chest is closed.
- 68. Injury to the ventricles by over distention Low output state. Abnormal heart rate and rhythm Asystole / heart block Supraventricular tachyarrhythmias Recurrent ventricular tachycardia or fibrillation. Air embolism to the brain, or heart or into the coronary arteries
- 69. Complication of heparin neutralization(Protamine) Myocardial depression leading to hypotension Histamine release Systemic vasodilation Pulmonary vasoconstriction Anaphylactic/ anaphylactic reactions Bronchospasm Pulmonary edema Deficient platelets and clotting factors
- 70. Patient should be shifted to the ICU, kept on mechanical ventilatory support (2-12hr) Monitored for his hemodynamic stability and cardiac electrical activity. Correct electrolyte and fluid imbalance. Adequate sedation and analgesia. Chest tube drain in 1st two hr of >250-300ml/hr in the absence of hemostatic effect→ surgical re exploration. Extubation considered when muscle paralysis has been worn off and patient is hemodynamically stable.