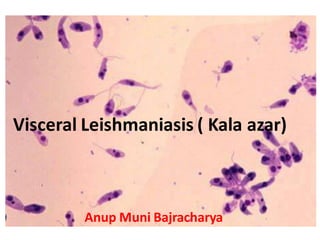
Visceral leishmaniasis ( kala azar)
•
10 recomendaciones•2,406 vistas

Visceral leishmaniasis (VL), also known as kala-azar, is the most severe form of leishmaniasis caused by the protozoan parasite Leishmania donovani and transmitted by the infected sandflies. It characterized by irregular bouts of fever, substantial weight loss, swelling of the spleen and liver, and anaemia.

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Visceral leishmaniasis ( kala azar)
Similar a Visceral leishmaniasis ( kala azar) (20)
Más de Anup Bajracharya
Más de Anup Bajracharya (20)
Último
Último (20)
Visceral leishmaniasis ( kala azar)
- 1. Visceral Leishmaniasis ( Kala azar) Anup Muni Bajracharya
- 2. Key facts • There are 3 main forms of leishmaniases – visceral (also known as kala- azar, which is and the most serious formof the disease), cutaneous (the most common), and mucocutaneous. • Leishmaniasis is caused by the protozoanLeishmania parasites which are transmitted by the bite of infectedfemale phlebotomine sandflies. • The disease affects some of the poorestpeople on earth, and is associatedwith malnutrition, population displacement, poor housing, a weak immune systemand lack of financial resources. • Leishmaniasis is linked to environmental changes such as deforestation, building of dams, irrigationschemes, and urbanization. • An estimated700 000 to 1 millionnew cases occur annually. • Only a small fraction of those infectedby Leishmania parasites will eventually developthe disease. Source- https://www.who.int/news-room/fact-sheets/detail/leishmaniasis A.B
- 3. A.B
- 4. The cutaneous form presents with skin ulcers. The mucocutaneous form presents with ulcers of the skin, mouth, and nose. The visceral form starts with skin ulcers and then later presents with fever, low red blood cells, and enlarged spleen and liver. Visceral Leishmaniasis A.B
- 6. Habitat • Promastigote forms of the parasite are found in sand fly. • Intracellular Amastigote forms are found in human in reticuloendothelial cells of the spleen, bone marrow, liver, intestinal mucosa and mesenteric lymph nodes. A.B
- 7. Geographical distribution • Visceral leishmaniasis (VL), also known as kala-azar is fatal if left untreatedin over 95% of cases. • It is characterized by irregular bouts of fever, weight loss, enlargement of the spleen and liver, and anaemia. • Most cases occur in Brazil, East Africa and in India. An estimated 50 000 to 90 000 new cases of VL occur worldwide annually, with only between 25 to 45% reported to WHO. • In 2018, more than 95% of new cases reported to WHO occurred in 10 countries: Brazil, China, Ethiopia, India, Iraq, Kenya, Nepal, Somalia, South Sudan and Sudan. A.B
- 9. Morphology: • The parasite exists in two forms: • Amastigote and Promastigote. A.B
- 10. Amastigote • Aflagellar stage of the parasite. • found in man and other mammalian hosts. • found inside monocytes, polymorphonuclear leucocytes or endothelial cells. • small, round to oval bodies measuring 2-3 µm in length. • known as LD (Leishman Donovan) bodies. • A rod –shaped kinetoplast lies at the right angles to the nucleus. • It comprises of DNA containing body and a mitochondrial structure. A.B
- 11. Promastigote • found in the digestive tract of sand fly (vector) and in the culture media. • are long, slender and splindle-shaped. • measure 15 to 25 µm in length and 1.5 to 3.5 µm in breadth. • A single nucleus is situated centrally. • The kinetoplast lies transversely near the anterior end. • The flagellum is single, delicate and projecting from front. A.B
- 12. Life cycle of Leishmania donovani • The parasite has two stages in its life cycle: • Amastigote form: occurring in humans and mammals. • Promastigote form: occurring in sandfly. • • Initiation - by the bite of infected female phlebotomine sand flies. • Injection of infective stage (i.e., promastigotes) proboscis during blood meals. • Promastigotes phagocytized by macrophages and other types of mononuclear phagocytic cells. • Promastigotes transform into amastigotes in these cells. • Amastigotes multiply in infected cells and affect different tissues, depending in part on the Leishmania species • Sandflies become infected during blood meals on an infected host when they ingest macrophages infected with amastigotes • In the sandfly's midgut, the parasites convert promastigotes , which multiply and migrate to the proboscis . A.B
- 14. Mode of transmission • The infection is transmitted to Human mainly by the bite of vector sandfly (Phlebotomus argentipes). • Less frequently the infection is transmitted by: • Blood transfusion, congenitial infection, accidental inoculation of cultured promastigotes in the lab workers. • Males are affected more due to increase exposure through the occupation and leisure activities. A.B
- 15. Pathogenicity • Visceral leishmaniasis, traditionally known as kala-azar ("black fever", particularly in India), because of its characteristic symptoms. • highly lethal if not treated properly. • Incubation period - 3 to 6 months, and in some cases may be over a year. • In Indian leishmaniasis, incubation can be as short as 10 days. • Target cells - mononuclear phagocyte system or reticuloendothelial system • The two main tissues of infection are spleen and liver. • Clinical symptoms include • pyrexia (recurring high fever which may be continuous or remittent), • enlargement of spleen and liver, and • heavy skin pigmentation which darkens the physical appearance (the reason for naming "black fever"). A.B
- 16. Pathogenicity • To a lesser extent - mucosa of the small intestine and lymph nodes are also invaded by the parasite. • Morphological symptoms are noticeable particularly on facial and abdominal regions. • Skin becomes coarse and hard. • In African infections, warty eruptions are common. • In a fully developed stage, the patient shows emaciation and anaemia. A.B
- 18. Laboratory diagnosis of leishmaniasis: • Specimens: • Splenic aspiration • Bone marrow aspirations • Lymph node aspiration • Peripheral blood A.B Source
- 19. Laboratory diagnosis of leishmaniasis: • Microscopy: smear preparation • The amastigotes of Leishmania donovan is known as LD bodies which can be demonstrated in the smears of bone marrow, liver, lymph node and peripheral blood smear stained with leishman, stains. • LD bodies are seen within macrophages. • Some of LD bodies can also be demonstrated free released from the cells ruptures during making of the smear. A.B
- 20. Laboratory diagnosis of leishmaniasis: • Culture • About 1-2 ml of blood (also splenic and bone marrow aspiration, other tissue and buffy coats of blood) is taken aseptically and diluted with 10ml of citrated saline solution. • The cells are then either allowed to settle in a cool incubator (22°C) overnight or centrifuged. • At the end of each week, a drop of condensation fluid is examined for promastigote forms. • In a positive culture, motile promastigotes can be demonstrated microscopically in a few days to 4 weeks. A.B
- 21. Laboratory diagnosis of leishmaniasis: • Detection of antibodies • Various serological test have been developed to detect circulating specific antibodies for diagnosis of VL. • This include • immunoenzymatic technique, • immunoblot, • IFA, • ELISA, • Westem blot. A.B
- 22. Direct Agglutination test (DAT) • Widely used serological test for diagnosis of kala-azar • Antigen used- trypsin treated, stained and formalin preserved promastigotes. • Positive reaction – agglutination with specific antibodies from VL positive patient A.B
- 23. • The rk39 based immunochromatgraphic test (ICT): • Rapid dip stick test • Antigen - recombinant k39 protien. • K39 is an epitope apparently conserved on amastigotes of leishmenia spp • Circulating anti-k39 IgG is detectable in 95-100% patients who have kala-azar, irrespective of geographical region. • Result can be obtained within 5 min. • The test is found in dipstick format that are more suitable for field case. A.B
- 24. Treatment-Antileishmanial medicines • Several medications are available. • Commonly used medicines include • Pentavalent antimonials (Meglumine antimoniate and Sodium stibogluconate-also known as Pentostam) • Amphotericin B, paromomycin, and miltefosine (Impavido).
- 25. Prevention & Control • The best way for travelers to prevent infection is to protect themselves from sand fly bites. • To decrease the risk of being bitten, follow these preventive measures: • Avoid outdoor activities, especially from dusk to dawn, when sand flies generally are the most active. • When outdoors (or in unprotectedquarters): • Minimize the amount of exposed (uncovered) skin. • Wear long-sleeved shirts, long pants, and socks • Apply insect repellent to exposed skin and under the ends of sleeves and pant legs. • The most effective repellents generally are those that contain the chemical DEET (N,N- diethylmetatoluamide).
- 26. Prevention & Control • When indoors: • Stay in well-screened or air-conditioned areas. • Sand flies are much smaller than mosquitoes and therefore can get through smaller holes. • Spray living/sleeping areas with an insecticide to kill insects. • Use a bed net and tuck it under mattress. If possible, use a bed net that has been soaked in or sprayed with a pyrethroid-containing insecticide. • The same treatment can be applied to screens, curtains, sheets, and clothing (clothing should be retreated after five washings).