CRESCER CRIANÇA/INFANTIL/JUVENIL:INTERFERÊNCIA DO GH E DO TSH
•Descargar como DOCX, PDF•
0 recomendaciones•698 vistas

Os hormônios da hipófise anterior são regulados pelo hipotálamo e liberando hormônios inibitórios e pelo feedback negativo dos hormônios alvo glandulares na hipófise e os níveis hipotalâmicos. Entre os hormônios da pituitária, só a secreção de prolactina é aumentada na ausência de influência do hipotálamo, porque é sobretudo subtônico na supressão de dopamina, o principal fator inibitório.

Recomendados
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a CRESCER CRIANÇA/INFANTIL/JUVENIL:INTERFERÊNCIA DO GH E DO TSH
Similar a CRESCER CRIANÇA/INFANTIL/JUVENIL:INTERFERÊNCIA DO GH E DO TSH (20)
Más de Van Der Häägen Brazil
Más de Van Der Häägen Brazil (20)
CRESCER CRIANÇA/INFANTIL/JUVENIL:INTERFERÊNCIA DO GH E DO TSH
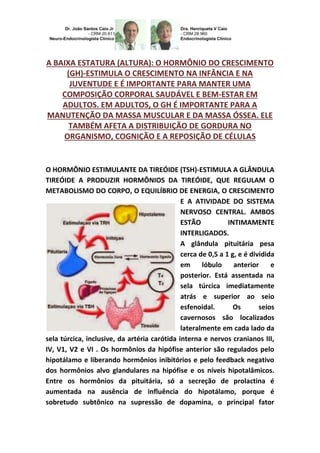
- 1. A BAIXA ESTATURA (ALTURA): O HORMÔNIO DO CRESCIMENTO (GH)-ESTIMULA O CRESCIMENTO NA INFÂNCIA E NA JUVENTUDE E É IMPORTANTE PARA MANTER UMA COMPOSIÇÃO CORPORAL SAUDÁVEL E BEM-ESTAR EM ADULTOS. EM ADULTOS, O GH É IMPORTANTE PARA A MANUTENÇÃO DA MASSA MUSCULAR E DA MASSA ÓSSEA. ELE TAMBÉM AFETA A DISTRIBUIÇÃO DE GORDURA NO ORGANISMO, COGNIÇÃO E A REPOSIÇÃO DE CÉLULAS O HORMÔNIO ESTIMULANTE DA TIREÓIDE (TSH)-ESTIMULA A GLÂNDULA TIREÓIDE A PRODUZIR HORMÔNIOS DA TIREÓIDE, QUE REGULAM O METABOLISMO DO CORPO, O EQUILÍBRIO DE ENERGIA, O CRESCIMENTO E A ATIVIDADE DO SISTEMA NERVOSO CENTRAL. AMBOS ESTÃO INTIMAMENTE INTERLIGADOS. A glândula pituitária pesa cerca de 0,5 a 1 g, e é dividida em lóbulo anterior e posterior. Está assentada na sela túrcica imediatamente atrás e superior ao seio esfenoidal. Os seios cavernosos são localizados lateralmente em cada lado da sela túrcica, inclusive, da artéria carótida interna e nervos cranianos III, IV, V1, V2 e VI . Os hormônios da hipófise anterior são regulados pelo hipotálamo e liberando hormônios inibitórios e pelo feedback negativo dos hormônios alvo glandulares na hipófise e os níveis hipotalâmicos. Entre os hormônios da pituitária, só a secreção de prolactina é aumentada na ausência de influência do hipotálamo, porque é sobretudo subtônico na supressão de dopamina, o principal fator
- 2. inibitório. A DGH-deficiência de GH em crianças faz com que a criança apresente baixa estatura longitudinal ou linear, pois este hormônio faz com que uma criança cresça. A DGH pode estar presente ao nascimento (congênita), ou pode ser o resultado de uma condição médica. Lesões cerebrais severas também podem causar DGH. Crianças com defeitos físicos da face e do crânio, como o lábio leporino ou fenda palatina, podem ter DGH. Na maioria das vezes, a causa da DGH é desconhecida. Invariavelmente ocorrerá uma baixa estatura (altura) longitudinal ou linear. O crescimento lento pode primeiramente ser notado na infância e continuar ao longo da infância, juventude e adolescência. O pediatra, o endocrinologista ou o neuroendocrinologista geralmente desenha a curva de crescimento da criança em um gráfico de crescimento. Crianças com DGH tem um ritmo lento ou simplesmente não ocorre o crescimento adequadamente. O lento crescimento pode não aparecer até que a criança tenha entre 2 ou 3 anos de idade. A criança será muito menor do que a maioria das crianças da mesma idade e sexo. A criança ainda terá proporções normais do corpo, embora a construção do seu corpo possa ser de aspecto gordinho. Muitas vezes o rosto da criança parece mais jovem do que as crianças da mesma idade. A criança geralmente tem inteligência normal. Em crianças mais velhas, a puberdade pode chegar atrasada ou pode não ocorrer em tudo, dependendo da causa. Os sintomas de DGH em adultos são sutis, composta por diminuição da força muscular, redução da tolerância ao exercício e redução da sensação de bem-estar (por exemplo, diminuição da libido, isolamento social, diminuição cognitiva e até osteoporose). Os pacientes com DGH têm aumento da gordura
- 3. corporal, principalmente na região abdominal, diminuição da massa corporal magra, e eles podem ter diminuição da densidade mineral óssea (DMO). Medições aleatórias do fator de crescimento semelhante à insulina I (IGF-I), os níveis de gênero ajustado por idade e GH não são confiáveis para diagnosticar a DGH, porque a secreção de GH é pulsátil, e até 65% dos pacientes com DGH tem um nível de normalidade do IGF-I. Portanto, a DGH é mais bem avaliada por testes dinâmicos. Durante alguns anos, a pesquisa no campo da endocrinologia do crescimento foi focada principalmente em GH. No entanto, verificou-se que o GH nem sempre controlava a taxa de crescimento. Por ex., não é claramente uma influência no crescimento intrauterino, além disso, embora os resultados de GRF ou administração de GH seja convincente, assim como, “ in vitro” o GH nem sempre claramente estimula a produção de somatomedina C, particularmente na presença de restrição alimentar e incluído este problema na vida fetal, e no hipotireoidismo as vezes ligadas ao gênero. Em tais situações, esse fenômeno está associado a uma produção de T3 (triiodotironina) reduzida, sugerindo uma influência significativa da função da tireóide na ação do GH e, mais genericamente, sobre o crescimento do corpo. De fato, inúmeros dados demonstram que os hormônios da tireóide estão fortemente envolvidos na regulação do crescimento do corpo. Em espécies com baixa maturidade ao nascimento, como nos roedores, T4 e T3 afetam o crescimento pós-natal onze dias mais cedo do que o aparecimento da influência de GH. A maior parte dos hormônios da tireóide em circulação no sangue está ligada para transportar proteínas. Só uma fração muito pequena da circulação hormonal é livre (não é ligada) e biologicamente ativa, portanto, a medição das concentrações de hormônios tireoidianos livres é de grande valor diagnóstico.
- 4. Quando o hormônio da tireóide está vinculado, não é ativo, de modo que a quantidade de T3/T4 livres é o que é importante. Por esta razão, a medição total de tiroxina no sangue pode ser enganadora. Além de seus efeitos metabólicos complexos envolvidos nos mecanismos gerais de crescimento do corpo, os hormônios da tireóide estimulam a produção de fatores de crescimento, particularmente o EGF e o NGF. Por outro lado, afetam a produção de GH e somatomedina C e também a sua atividade nos tecidos. Todos estes resultados sugerem fortemente que seria difícil estudar regulação do GH e seus efeitos fisiológicos, sem levar em conta a função da tireóide. GROWTH CHILD/INFANT/YOUTH: INTERFERENCE GH AND TSH. CAIO JR., DR., CAIO, DRA., HENRIQUETA V. THE LOW HEIGHT: THE GROWTH HORMONE (GH) - STIMULATES GROWTH CHILDHOOD AND YOUTH AND IT IS IMPORTANT TO MAINTAIN A HEALTHY BODY COMPOSITION AND WELFARE IN ADULTS. IN ADULTS, THE GH IS IMPORTANT FOR THE MAINTENANCE OF MUSCLE MASS AND BONE MASS. IT AFFECTS THE DISTRIBUTION OF FAT IN THE BODY, MAINLY ABDOMINAL FAT, COGNITION AND REPLACEMENT OF CELLS AS WELL. THE THYROID STIMULATING HORMONE (TSH) - ENCOURAGES THYROID GLAND TO PRODUCE THYROIDS HORMONES, WHICH REGULATE THE BODY'S METABOLISM, ENERGY BALANCE, GROWTH AND ACTIVITY OF THE CENTRAL NERVOUS SYSTEM. BOTH ARE CLOSELY LINKED.
- 5. PHYSIOLOGY-ENDOCRINOLOGY-NEUROENDOCRINOLOGY-GENETICS- ENDOCRINE-PEDIATRICS (SUBDIVISION OF ENDOCRINOLOGY): DR. JOÃO SANTOS CAIO JR ET DRA. HENRIQUETA VERLANGIERI CAIO. The pituitary gland weights about 0.5 to 1 g, and is divided into anterior and posterior lobes. It sits in the sella immediately behind and above the sphenoid sinus saddle. Cavernous sinuses are located laterally on each side of the saddle, including the internal carotid artery and cranial nerves III, IV, V1, V2 and VI. Anterior pituitary hormones are regulated by hypothalamic releasing and inhibitory hormones and the negative feedback of the target glands hormones in the pituitary and hypothalamic levels. Among the pituitary hormones, only prolactin secretion is increased in the absence of influence of the hypothalamus, particularly because it is under tonic dopamine in the suppression of the major inhibitory factor. GHD in children causes the low longitudinal or linear statures in children because this hormone promotes a child grow. A GHD may be present at birth (congenital) or can be the result of the medical condition. Severe brain injuries can also cause GHD. The children of the face and skull physical defects, such as cleft lip or cleft palate may have decreased levels of GH. Most often, the cause of GHD is unknown. Invariably the low height longitudinal or linear occurs. Slow growth may first be noticed in childhood and continue throughout childhood, adolescence and youth. The pediatrician, endocrinologist or neuroendocrinologist usually draws the curve of growth of the child on a growth chart. The children with GHD have a
- 6. slow pace or simply do not occur properly growth. The slow growth may not appear until the child is between 2 and 3 years old. The child will be much smaller than most children of the same age and sex. The child will still have normal body proportions, although his body building can be chubby appearance. Often the child's face looks younger than children of the same age. The children usually have normal intelligence. In older children, puberty may get delayed or may not occur at all, depending on the cause. The symptoms of GHD in adults are subtle, consisting of decreased muscle strength, reduced exercise tolerance and reduced sense of well-being (e.g., decreased libido, social isolation, cognitive decline and even osteoporosis). Patients with GHD have increased body fat mainly the abdominal fat, decreased lean body mass, and they may have decreased bone mineral density. Random measurements factor-I (IGF-I) levels of gender and similar age-adjusted insulin and GH are unreliable for diagnosing GHD because GH secretion is pulsatile, and up to 65% of patients with GHD have a level of normalcy in IGF-I. Therefore, GHD is best assessed by dynamic tests. For several years, research in the field of endocrinology of growth has been mainly focused on GH. However, it appears that GH does not always control the rate of growth. For example, it is clearly an influence on intrauterine growth: moreover, although the results of GRF or GH administration are convincing, and GH “in vitro” are not always clearly stimulates the production of somatomedin C, particularly in the presence of food restriction and included this problem in fetal life, and sometimes hypothyroidism linked to gender. In such situations, this phenomenon is associated with a reduced production of T3 (triiodotironina), suggesting a significant influence of thyroid function in GH action and, more generally, on the growth of the body. Indeed, numerous data show that the thyroid hormone is heavily involved in the regulation of body growth. In species with low maturity at birth as in rodents, T3/T4 affect postnatal growth eleven days earlier than the appearance of the influence of GH. Most thyroid hormones circulating in the blood is bound to transport proteins. Only a very small fraction of the circulating hormone is free (unbound) and biologically active, hence measuring concentrations of free thyroid hormones is of great diagnostic value. When the thyroid hormones are bound, they are not active, so that the amount of T3/T4 free is what is
- 7. important. For this reason, measurement of total thyroxine in blood can be misleading. In addition to its complex metabolic effects involved in general mechanisms of body growth, thyroid hormone stimulates the production of growth factors, particularly EGF and NGF. On the other hand, affects the production of somatomedin C, GH and also its activity in tissues. All these results strongly suggest that it would be difficult to study GH regulation and physiological effects, without regard to thyroid function. Dr. João Santos Caio Jr. Endocrinologia – Neuroendocrinologista CRM 20611 Dra. Henriqueta V. Caio Endocrinologista – Medicina Interna CRM 28930 Como saber mais: 1. Na criança, infantil e juvenil com deficiência de hormônio do crescimento (DGH), sabe-se que a dose de reposição de hormônio do crescimento (GH), quando efetuado nesta fase e com uma duração do
- 8. tratamento prolongada, pode influenciar significativamente na altura final do adulto... http://hormoniocrescimentoadultos.blogspot.com 2. Presentemente, a dosagem de hormônio do crescimento (GH), administrada a crianças de estatura baixa longitudinal ou linear é mantida a uma taxa constante por toda a puberdade... http://longevidadefutura.blogspot.com 3. As taxas de produção de GH aumentaram acentuadamente durante a puberdade humana, principalmente como um fenômeno de amplitude modulada... http://imcobesidade.blogspot.com AUTORIZADO O USO DOS DIREITOS AUTORAIS COM CITAÇÃO DOS AUTORES PROSPECTIVOS ET REFERÊNCIA BIBLIOGRÁFICA. Referências Bibliográficas: Caio Jr, João Santos, Dr.; Endocrinologista, Neuroendocrinologista, Caio,H. V., Dra. Endocrinologista, Medicina Interna – Van Der Häägen Brazil, São Paulo, Brasil; Lindgren AC, Hagenas L, Muller J, Blichfeldt S, Rosenborg M, Brismar T et al. Effects of growth hormone treatment on growth and body composition in Prader-Willi syndrome: a preliminary report. The Swedish National Growth Hormone Advisory Group. Acta Paediatr Suppl 1997;423:60-2; Lindgren AC, Hagenas L, Muller J, Blichfeldt S, Rosenborg M, Brismar Tet al. Growth hormone treatment of children with Prader-Willi syndrome affects linear growth and body composition favourably. Acta Paediatr 1998;87(1):28-31; Whitman BY, Myers S, Carrel A, Allen D. A treatment/control group study of growth hormone treatment: Impact on behavior - A preliminary look. Endocrinologist 2000; 10(4 SUPPL.1):31S-7S; McCaughey ES, Mulligan J, Voss LD, Betts PR. Randomised trial of growth hormone in short normal girls. Lancet 1998;351(9107):940-4; Idiopathic short stature:results of a one-year controlled study of human growth hormone treatment. Genentech Collaborative Study Group. J Pediatr1989;115(5 Pt 1):713-9; McCaughey ES, Mulligan J, Voss LD, Betts PR. Growth and metabolic consequences of growth hormone treatment in prepubertal short normal children. Archives of Disease in Childhood 1994;71(3):201-6; Barton JS, Gardiner HM, Cullen S, Hindmarsh PC, Brook CGD, Preece MA. The growth and cardiovascular effects of high-dose growth hormone therapy in idiopathic short stature. Clinical Endocrinology 1995;42(6):619-26; Volta C, Bernasconi S, Tondi P, Salvioli V, Ghizzoni L, Baldini A et al. Combined treatment with growth hormone and luteinizing hormone releasing hormone- analogue (LHRHa) of pubertal children with familial short stature. J Endocrinol Invest 1993;16(10):763- 7; Cowell CT. Effects of growth hormone in short, slowly growing children without growth hormone deficiency. Australasian Paediatric Endocrine Group. Acta Paediatr Scand Suppl 1990;366:29-30; Ackland FM, Jones J, Buckler JM, Dunger DB, Rayner PH, Preece MA. Growth hormone treatment in
- 9. non-growth hormone-deficient children: effects of stopping treatment. Acta Paediatr Scand Suppl 1990;366:32-7; Cutfield W, Lindberg AWK, Chatelain P, Ranke M, Wilton P. Final height in idiopathic growth hormone deficiency: The KIGS experience. Acta Paediatr Int J Paediatr Suppl 1999;88/428:72- 5; August G, Julius J, Blethen S. Adult height in children with growth hormone deficiency.Pediatrics1998;102:512-6. Contato: Fones: 55 11 5087-4404 ou 96197-0305 Nextel: ID:111*101625 Rua Estela, 515 - Bloco D - 12º andar - Conj. 121/122 Paraiso - São Paulo - SP - Cep 04011-002 e-mails: drcaio@vanderhaagenbrasil.com drahenriqueta@vanderhaagenbrasil.com vanderhaagen@vanderhaagenbrasil.com Site Van Der Häägen Brazil www.vanderhaagenbrazil.com.br www.clinicavanderhaagen.com.br www.crescimentoinfoco.com www.obesidadeinfoco.com.br http://drcaiojr.site.med.br http://dracaio.site.med.br Joao Santos Caio Jr http://google.com/+JoaoSantosCaioJr Video http://youtu.be/woonaiFJQwY Google Maps: http://maps.google.com.br/maps/place?cid=5099901339000351730&q=Van+Der+Haagen+Brasil&hl= pt&sll=-23.578256,46.645653&sspn=0.005074,0.009645&ie =UTF8&ll=-23.575591,- 46.650481&spn=0,0&t = h&z=17