
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Temporomandibular Joint (TMJ )
Similar a Temporomandibular Joint (TMJ ) (20)
Más de Dr Monika Negi
Más de Dr Monika Negi (18)
Último
Último (20)
Temporomandibular Joint (TMJ )
- 1. DR MONIKA NEGI MDS ORAL PATHOLOGY, MICROBIOLOGY & FORENSIC ODONTOLOGY TEMPOROMANDIBULAR JOINT
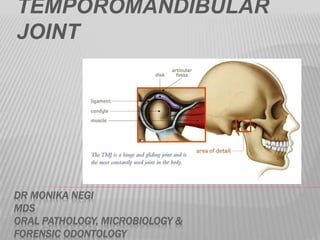
- 2. INTRODUCTION The TMJ is a complex and precisely integrated bilateral joint structure . Formed by the articulation of lower jaw with cranium and the upper facial skeleton . BONES TAKING PART ARE –MANDIBULAR +TEMPORAL BONES = TEMPOROMANDIBULAR JOINT . The head of the condyle of the mandible articulates with the articular fossa and articular eminence of the temporal bone . It functions in speech ,mastication and deglutition . The downward and forward sliding action of the condylar heads can be felt opening and closing the mouth and during symmetric protrusion and retrusion and asymmetric lateral shift .
- 3. MANDIBLE
- 4. TEMPOROMANDIBULAR JOINT (TMJ ) ANATOMY The TMJ is a synovial bilateral joint that permits the mandible to move as a unit with 2 functional patterns (gliding and hinge movements) The TMJ is a ginglymoarthrodial joint, a term that is derived from ginglymus, meaning a hinge joint, allowing motion only backward and forward in one plane, and arthrodia, meaning a joint of which permits a gliding motion of the surfaces..
- 5. The common features of the synovial joints exhibited by this joint include a disk, bone, fibrous capsule, fluid, synovial membrane, and ligaments. However the features that differentiate and make this joint unique are its articular surface covered by fibrocartilage instead of hyaline cartilage.
- 6. PECULIARITY OF TMJ 1. Bilateral diarthrosis– right & left function together 2. Articular surface covered by fibrocartilage instead of hyaline cartilage 3. Only joint in human body to have a rigid end point of closure that of the teeth making occlusal contact.
- 7. COMPONENTS (Bone/Hard components ) Mandibular condyle Glenoid fossa of the temporal bone Articular eminence (Soft tissue components ) Capsule Articular disc Ligaments Muscular component
- 8. The mandibular condyle articulates with the glenoid fossa and articular eminence of the temporal bone. An articular disc separates the articular surfaces so that 2 cavities are present: Upper compartment between the disc and temporal bone. Lower compartment between the condyle and the disc
- 9. The joint capsule is attached below to the articular margin of the head of the condyle, and above to the margins of the glenoid fossa and articular eminence. The inner aspect of the capsule is lined by a synovial membrane.
- 10. At the sides, the capsule is strengthened by collateral ligaments of which the lateral temporomandibular ligament is the strongest. The lateral temporo-mandibular ligament is attached above to the zygoma, and below, it is attached to the lateral surfaces and posterior border of the neck of the mandible.
- 11. There are 2 accessory ligaments associated with the TMJ: The stylomandibular ligament attaches to the styloid process and to the posterior border of the ramus. The sphenomandibular ligament extends between the spine of the sphenoid bone and the lingula of the mandible. These ligaments limit the range of movement of the condyle preventing it from coming in contact with the tympanic plate behind and passing beyond the articular eminence in front.
- 12. THE MANDIBULAR CONDYLE It’s the articulating surface of the mandible. It is convex in all directions but wider latero-medially than antero-posteriorly. It has lateral and medial poles: The medial pole is directed more posteriorly. The long axis of the two poles deviate posteriorly and meets at the anterior border of the foramen magnum.
- 13. HISTOLOGY Composed of cancellous bone covered by a thin layer of compact bone. Trabeculae: of the cancellous bone is arranged in a radiating manner from the neck to reach the surface of the condyle at a right angle (to give maximum strength.) Bone marrow is of myeloid or cellular type and becomes fatty with age.
- 14. Outer layer of compact bone is covered by thick layers of fibrous tissues composed of: Superficial layer : network of strong collagen fibers, chondrocytes and fibroblasts. Deep layer: thin collagen fibers rich in chondroid cells during growth period (hyaline cartilage). Growth occur by apposition from the deepest layer – the deepest surface of the cartilaginous plate is replaced by bone. Growth continues till 21 years of age. Remnants of cartilage may persist in old age.
- 15. MANDIBULAR (GLENOID) FOSSA AND ARTICULAR EMINENCE Glenoid fossa: Posteriorly limited by the squamotympanic fissure. Anterioly bounded by the articular eminence. Roof: thin layer of compact bone separating the middle cranial fossa. Articular eminence: Composed of: Spongy bone covered by thin layer of compact bone. Chondroid tissues commonly seen in the eminence.
- 16. Fibrous layer covering the articulating surface of temporal bone. Thin on the articular fossa and thickens on the posterior slope of the eminence Over the eminence the fibrous tissues are arranged in 3 zones: Inner zone – fibers arranged at right angle to surface Outer zone – fibers run parallel to the bone surface Intermediate zone – transitional zone. Fibers are interlaced.
- 17. INTERARTICULAR DISC (MENISCUS) Disk is fibrous, avascular, non inverted plate Shape is oval, biconcave in sagittal section. It is thin in central part and thick at posterior borders.
- 18. Attachment: Medial and lateral poles of the condyle by medial and lateral ligaments. Divide the joint into: Upper (larger) compartment and lower (smaller) compartment.
- 19. Anterior border divides into upper and lower lamellae that run forward. The upper lamella fuses with the anterior slope of the articular eminence. The lower lamella attaches to the front of the neck of the condyle. Fibers of the superior head of the lateral pterygoid muscle is attached to the anterior border.
- 20. Posterior border divides into upper and lower lamellae The upper lamella is fibrous and elastic and fuses with the capsule and is inserted in the squamotympanic fissure. The lower lamella, non elastic, attaches to the back of the condyle.
- 21. HISTOLOGY Composed of dense fibrous tissue containing: Straight and tightly packed collagenous fibers Few elastic fibers. Some chondroid cells appear with age. Chondrocytes may be seen. The space between upper and lower posterior is filled with highly vascular loose connective tissue.
- 22. ARTICULATING CAPSULE AND LIGAMENTS AND SYNOVIAL MEMBRANE The whole TMJ is enclosed in a fibrous capsule. It is attached to: Articular tubercle (in front) Lips of squamous tympanic fissure (posteriorly) Borders of articulating glenoid fossa Neck of the mandible. (below) It is lined by synovial membrane. Laterally, the capsule is reinforced by TMJ ligaments.
- 23. HISTOLOGY Consists of 2 layers: Outer fibrous capsule – strengthen laterally to form the temporomandibular ligament. Inner synovial layer – composed of thin connective tissue layer lined with: Synovial cells Type A : secretes hyaluronic acid Type B : produces protein rich secretion. Synovial folds and villi protrude from the surface into the joint cavity. Synovial layer of cells line the entire capsule of both upper and lower joint spaces. Synovial membrane is very rich in blood supply and contains lymphatic vessels.
- 24. SYNOVIAL FLUID It is clear, straw-colored viscous fluid. It diffuses out from the rich cappillary network of the synovial membrane. Contains: Hyaluronic acid which is highly viscous May also contain some free cells mostly macrophages. Functions: Lubricant for articulating surfaces. Carry nutrients to the avascular tissue of the joint. Clear the tissue debris caused by normal wear and tear of the articulating surfaces.
- 25. BLOOD SUPPLY 4 arteries supply the joint: Superficial temporal Deep auricular Anterior tympanic Ascending pharyngeal Branches from the 4 approach the joint and penetrate the capsule.
- 26. NERVE SUPPLY Branches from the mandibular nerve Auriculotemporal nerve Masseteric nerve Deep temporal nerves Supply all surfaces of the head, fossa, capsule and part of the disk.
- 27. DEVELOPMENT OF TMJ Ontogenetically & Phylogenitically TMJ is a secondary joint. i.e it is developed from primary reptilian type .in reptilian type ,the TMJ is formed at dorsal end of meckel’s cartilage ,which in humans appear as joint between malleus and incus bones of the middle year showing adaptation of bones of primitive jaw to sound conduction. Meckel’s cartilage forms and provide skeletal support for developing lower jaw . Cartilage extends backward and dorsally and terminates as malleus 7th week - Articulation between malleus and incus at the dorsal end of Meckel’s cartilage – PRIMARY JOINT . • 8th week- Membranous Bone laid down in a plate like form lateral to Meckels cartilage. • 10 week (IU) -from 2 widely separated centers that grow toward each other evidence of future joint as mesenchyme between the condylar cartilage & developing temporal bone.
- 28. 12 week: A pair of clefts appears in the mesenchyme between developing squamous portion of temporal bone And develops into upper and lower joint cavity Joint capsule is formed from condensation of mesenchyme (which progressively isolates the joint with its linning synovial membrane ) Condylar grows dorsolaterally Ossification of temporal blastema Inferior joint cavity Differentiation of condylar into cartilage & Sup.joint cavity Formation of disc
- 29. 13th week : Condyle and articular disk have moved up into contact with temporal bone. • Remnant of meckels cartilage - sphenomandibular ligament • Full differentiation of all articular surfaces occurs by 4th fetal month.
- 31. MUSCLES Masseter Temporalis Medial pterygoid Lateral pterygoid
- 32. Elevation of Mandible Temporalis Masseter Medial Pterygoids Depression Of Mandible Lateral pterygoid Digastric Geniohyoid Protrusion of Mandible Lateral Pterygoids Medial Pterygoids Retraction of Mandible Posterior fibres of Temporalis
- 33. Actions of the muscle of mastication A.Elevation –M Masseter ;MPt,medial pterygoid ; T.Temporalis B.Depression –IH.Infra hyoid ;LPt,lateral petrygoid ;SH,suprahyoid C.Protrusion .M (Sup),masseter,superficial fibers . D.Retrusion .M(deep ) masseter ,deep fibers ; T(horizontal) Temporalis ,horizontal fibers . E.Right lateral excrusion of the mandible Lt.Mpt,left medial pterygoid ,Lt Pt,left lateral pterygoid ,Rt M ,right masseter ,Rt T ,Right Temporalis F.Left lateral excrusion of the mandible . Lt M ,LEFT masseter .Lt T ,Left temporalis ,Rt Lpt ,right lateral pterygoid ,Rt MPt ,right medial pterygoid .
- 34. MOVEMENTS OF TMJ Rotational movement occurs in first 20-25mm of mouth opening Translational movement after that when the mouth is excessively opened
- 35. CHANGING POSITION OF THE MANDIBLE
- 36. AGE CHANGES Condyle: Becomes more flattened Fibrous capsule becomes thicker. Osteoporosis of underlying bone. Thinning or absence of cartilaginous zone. Disk: Becomes thinner. Shows hyalinization and chondroid changes. Synovial fold: Become fibrotic with thick basement membrane. Blood vessels and nerves: Walls of blood vessels thickened. Nerves decrease in number
- 37. CHANGES COULD LEAD TO: Dysfunction in old age Impairment of motion due to decrease in the extensibility of the disk and the capsule. Decrease in the secretion of the synovial fluid. The term myofacial pain dysfucntion syndrome (MPDS) is used to indicate a dysfunction of TMJ Characterized by Masticatory muscle tenderness (mostly lateral pterygoid ,temporalis ,medial pterygoid and masseter .) Limited opening of the mandible <37 mm . Joint sounds . Dislocation of the TMJ may take place without impact of external force . It is usually bilateral and displacement is anterior . When mouth is opened wide during yawning ,head of the mandible slip forward into the infra temporal fossa causing articular dislocation of the joint .
- 38. Recent diagnostic techniques such as CT (COMPUTERIZED TOMOGRAPHY ) and MRI (MAGNETIC RESONANCE IMAGING) permit the visualization of the TMJ disk in patients The disk ,for reasons not yet determined ,becomes displaced anteromedially and creates one or more of the following signs and symptoms :pain ,clicking ,limitation of jaw movement ,deviation or opening or locking . If remains untreated it leads to osteoarthrosis .