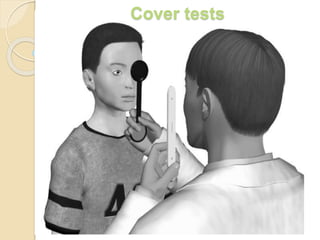
Cover tests
•Descargar como PPTX, PDF•
35 recomendaciones•27,486 vistas

Cover tests : Ophthalmology

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Cover tests
Similar a Cover tests (20)
Más de Dr Samarth Mishra
Más de Dr Samarth Mishra (20)
Último
Último (20)
Cover tests
- 1. Cover tests
- 2. Tests for ocular alignment • Cover tests • Corneal light reflex tests ( e.g: Hirschberg test ) • Dissimilar image tests • Dissimilar target tests
- 3. Foveal fixation in each eye, attention, cooperation, and the ability to make eye movements are all necessary for cover testing. They allow the examiner to: 1) differentiate between tropia and phoria, 2) Asses the degree of control of deviation 3) Note fixation preference and strength of fixation of both eyes. If a patient is unable to maintain constant fixation on an accommodative target, cover tests should not be used. 3 types of cover tests: 1) cover-uncover test. 2) alternate cover test. 3) simultaneous prism and cover test.
- 4. It is typically performed by the ophthalmologist, orthoptist, or ophthalmic technician. The comprehensive cover test assessment is multifaceted. Cover testing can be done to measure a deviation at near, which requires an accommodative target held at a distance of 33cm for fixation. It can also be done to measure a deviation with distance fixation.
- 5. Detection of squint: -a cover- uncover test is required to confirm a squint. It has two components: 1) Observations to be made during covering. ( cover test ) 2) Observations to be made during uncovering. ( cover-uncover test )
- 7. Cover testing is the gold standard objective method for determining the presence, type, and amount of ocular misalignment (strabismus) It is a monocular test. It is simple to undertake, does not require great amounts of skill by the examiner and is objective in nature cover-uncover test is an objective determination of the presence and amount of ocular deviation Most important test for detecting manifest strabismus.
- 8. Also for differentiating a heterophoria from heterotropia. Should be done for both distance and near. The single cover test is generally performed first. This is done by using an opaque or translucent (fogged) occluder to occlude one eye.
- 9. In case of children it is the hand or a thumb which can be used to avoid scaring them. It is important to have a proper fixation target. It should be a figure or letter of size 6/9 of snellen’s chart. This is to control accommodation.
- 10. A fixation achieved by torch is not desirable. The fixation distance should be 33cm for near and 6 meters for distance. As each eye is covered, the examiner watches for any movement in the opposite, non-covered eye; such a movt indicates a heterotropia. (cover test) If there is no movt of the uncovered eye, movt of the covered eye as the cover is applied and movt in opposite direction as the cover is removed indicates a heterophoria. (Uncover test)
- 11. The uncover test is helpful in unmasking the latent squint (heterophoria) which presents with both eyes appearing to fixate the target. One of the eyes is covered, which breaks the fusion, and if there is any heterophoria the eye behind cover deviates. (up/down/in/out) The examiner then observes the behaviour of this eye as he removes the cover. If it remains deviated it confirms a latent squint with poor fusion (poor recovery)
- 12. If it recovers the examiner observes for speed of recovery. The speed of recovery indicates the strength of fusion and is an important prognostic sign. If the pt has a heterophoria, the eyes will be straight before and after the cover-uncover test. The deviation appears during the test.
- 13. This is because of interruption of binocular vision. A pt with a heterotropia, however, starts with a deviated eye and after testing end with the same eye or in case of alternate heterotropia ,the opposite eye deviated. In some pts with heterophoria, the eyes are straight before testing, but they dissociate into a manifest deviation (heterotropia) after the occlusion interrupts the binocular vision.
- 14. Prerequisites for cover-uncover tests: Ability of both eyes to fixate the target. Ability of both eyes to have central fixation. Ability of both eyes to have no gross / severe motility defect. In presence of one eye being : blind/ markedley subnormal vision / severe restriction/ limitation movement / an eccentric fixation, which will not permit the eyes to refixate , the cover-uncover test may be fallacious.
- 15. For infants, who would not allow an occluder or a hand close to their face , the examiner can use indirect occlusion test or distant cover test. For children, very small pictures like those seen on a Lang stick can be used. Whereas for adults a small Snellen chart letter or number can be used Here the fixation target or light is obstructed for one eye by an occluder at some distance away from the
- 16. Information from cover-uncover test: Confirms a true manifest or latent squint and also its type: exo/ eso/ vertical deviation. It also indicates the visual dominance or the presence of amblyopia. The examiner can detect even small angle squints leaving only microtropia of < 5 prism dioptre deviation. A cover- uncover test needs to be done in all nine cardinal positions of gaze, as also for near and distance fixation
- 17. In a Manifest Strabismus it can tell us the following: - The type of deviation: whether it be eso, exo, hyper, hypo or cyclo tropia. - The size of the deviation: slight, small, moderate or large -Speed to take up fixation: if the eye takes up fixation fast it means there is good vision in that eye -Accommodation on the deviation - Nystagmus -Dissociated vertical deviation (DVD) - Incomitance – deviation angle varies in each position of gaze.
- 18. In a Latent Deviation it can tell us the following: esophoria, exophoria, -Type of deviation: hyperphoria, hypophoria, cyclophoria - Size of deviation - Rate of recovery that enables the person to achieve binocular single vision. - It also says about the strength of control over the deviation.
- 21. Uncover test
- 23. The alternate cover test is performed after the single cover test. The alternate cover test is the most dissociative cover test and measures a total deviation, including the tropic plus the phoric/latent component. This test is done to dissociate binocular fusion. Alternately each eye is occluded and refixation movt of uncovered eye to midline is observed. No shift in alternate cover test indicates orthophoria. A refixation shift to cover/alternate cover test indicates presence of strabismus, either a tropia, phoria or a tropia with phoria. Presence of a phoria is an indication of binocular fusion. If no movement was seen on the unilateral cover test, but movement is noted on the alternating test, the patient has a phoria
- 26. Alternate prism cover test
- 27. The alternate prism cover test is similar to the alternate cover test, with the addition of a prism held over one eye to quantify the misalignment Determines the amount of prism necessary to neutralize the full deviation including any latent phoria, by quantitating the shift associated with alternate cover testing. A prism is placed in front of deviating eye with apex towards the deviation. Alternate cover testing is then done with prism in place. The prism is changed ( either increased or decreased ) depending on the refixation shift.
- 28. Detects both latent and manifest deviations. Testing should be performed at both distance and near fixation. Used to dissociate binocular fusion. Deviation is quantified using prisms to eliminate the eye movt as the occluder is switched from eye to eye.(prism alternate cover test)
- 29. The misalignment is quantified with the size of the prism (measured in Prism Diopters) which is required to neutralize the deviation. It may be necessary to use both horizontally and vertically placed prisms. This measures total deviation. Does not distinguish between latent (heterophoria) and manifest (hereotropia) components of deviation.
- 30. 2 horizontal or 2 vertical prisms should not be stacked because doing so can induce significant measurment errors. A more accurate method for measuring deviations larger than those a single prism can correct is to place prisms in front of each eye, although this is not perfectly additive either. However, it is acceptable to stack a horizontal and vertical prism over the same eye, if necessary. If the pt head is tilted, the prisms must be tilted accordingly.
- 31. Simultaneous prism and cover test
- 32. It is used to measure the tropia component of the monofixation syndrome without dissociating the phoria. Used in patients with small angle strabismus. Performed by placing a prism in front of the deviating eye and covering the fixating eye at the same time. The test is repeated using increasing prism powers untill the deviating eye no longer shifts. The simultaneous prism and cover test provides the best indication of the size of the deviation under real life conditions.
- 33. Common causes of variable measurements: Poor control of accommodation. Variable working distance Tonic fusion not suspended. Physiologic redress fixation movt. Incomitant deviation.
- 34. Measurements should ideally be done in all 9 cardinal position of gaze, especially for identifying and quantifying incomitance. Measuring the deviation in primary position, upgaze, downgaze, right and left gaze, and with head tilt are sufficient. Measurement of deviation in primary position should be done at near (1/3 meter). Plastic prisms are placed in the frontal position i.e, parallel to infraorbital margin. Glass prisms are placed in prentice position, i.e the posterior surface of prism is perpendicular to the line of sight.
- 37. Cautions to be noted in avoidance of misdiagnoses /contamination of results It is important to avoid prolonged periods of dissociation of the eyes until a diagnosis can be made regarding the strabismus. Hence, the importance to note that although the eyes require dissociation for a minimum of three seconds, that dissociation is kept minimal whilst fixation is maintained. In the case of intermittent or latent deviations, for dissociative complications leading to misdiagnosis, it is also advised that binocular vision is tested prior, along with stereo testing. Frequently, during testing, the cover can be removed prematurely, therefore as mentioned earlier; dissociation of at least three seconds is needed for the patient to take up fixation during cover testing. This time allows for patients to recover from dissociation post cover removal.
- 38. The use of a penlight should be utilized to observe the steadiness and positioning of the deviated eye. Ensure to assist the patient in maintaining fixation on accommodative or distance targets at all times- if testing on children or adults, request specific details pertaining to the accommodative target (to assure accommodation is utilized) for near testing. Use of a detailed target for near fixation in both adults and children will identify the effects of accommodation on the deviation. Observing pupillary constriction should also be indicative of accommodation.
- 39. Cover-Uncover testing and alternate cover testing should be performed on the deviating eye even when a constant heterotropia is observed. This practice ensures the detection of a consistent increase in deviation and DVD isn’t neglected. The presence of orthophoria in uncommon when assessing both near and far fixation. VA must be considered when there is no deviation seen upon cover testing given amblyopic eyes may not take up fixation (VA too poor to see target or eccentric fixation). Microtropia may be present when a small unequal VA is recorded.
- 40. Cover test
- 43. THANK YOU..