
Recomendados
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a TURP
Similar a TURP (20)
Más de DrVishal Kandhway
Último
Último (20)
TURP
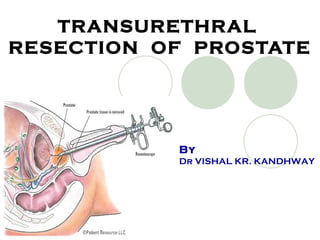
- 1. TRANSURETHRAL RESECTION OF PROSTATE By Dr VISHAL KR. KANDHWAY
- 2. INTRODUCTION Benign prostate hyperplasia is responsible for majority of urinary symptoms in men over 50 yrs of age TURP is a type of prostate surgery done to relieve moderate to severe urinary symptoms caused by an enlarged prostate(BPH( -TURP uses cystoscopy and a resectoscope to remove tissue protruding into the prostatic urethra. -So this procedure is most commonly performed on elderly patients- a population with high incidence of cardiac, respiratory and renal disease. -Safe anaesthesia depends on detection and optimisation of co-existing diseases, and weighing the relative risks and benefits of regional and general anaesthesia for each patient.
- 3. ANATOMY OF PROSTATE GLAND Pyramidal shaped organ Lies below urinary bladder & located infront of the rectum, posterior to the pubic symphysis & superior to the perineal membrane Normal weight- 20 g Encircles urethera as it emerges from base of bladder. It Is enclosed within a capsule composed of collagen, elasten & large no. of smooth muscles Microscopic anatomy -1.Transitional -2.Central -3.periphery zone
- 4. Transional zone: -This is the area surrounding the prostatic urethra. It is were the BPH occurs. Central zone: It is the area surrounding the ejaculatory duct Peripheral zone: This zone covers the posterior & lateral zone aspects of the prostate. It is the most common area affected by chronic prostatitis & adenocarcinoma.
- 5. The Prostate Gland is rich in blood supply, mainly from inferior vesical artery The prostatic venous plexus drains into internal iliac vein & communicates with the vertebral plexus, thereby allowing neoplastic spread to vertebrae The prostatic vessels & the autonomic innervations run between the layers of the lateral prostatic fascia & the prostate. -Arteries and veins penetrate the capsule and branch inside the gland. -The venous sinuses adjacent to the capsule are particularly large. Nerve Supply -Prostatic plexus-Sympathetic- T12-L2(contraction of smooth muscles of capsule & stroma( -Parasympathetic- S2-S4(prostatic secretion( -Pain fibres from Prostate, Prostatic Urethra and Bladder mucosa- S2-S4 -Bladder distension pain – T12-L2
- 6. SURGICAL PROCEDURE -TURP - performed by inserting a Resectoscope through urethra. -Prostatic tissue is resected into pieces with an electrically powered cutting- coagulating metal loop. -Pieces washed out by irrigating solution. -Prostatic capsule preserved- If violated, large amounts of irrigating fluid is absorbed into circulation, periprostatic and retroperitoneal spaces.
- 7. -Surgery normally takes 30-60 mins- depending on size of gland and experience of surgeon. -Position- Lithotomy position -At the end of surgery- a 3-lumen catheter placed to allow continuous irrigation using normal saline for upto 24 hours after surgery
- 8. IRRIGATION FLUIDS -Properties of ideal Irrigation Solution- 1.Transparent- allows visualization 2.Isotonic 3.Electrically non conductive- allows diathermy to work. 4.Non-hemolytic 5.Non metabolised 6.Non-toxic 7.Inexpensive 8.Easy to sterilize
- 10. Commonly used Irrigation Solutions are- SOLUTION OSMOLALITY (mOsm/Kg( Glycine, 1.2% 175 Glycine, 1.5% 220 Sorbitol, 3.5% 165 Mannitol, 5% 275 Cytal )Sorbitol 2.7% + Mannitol 0.54%( 178 Glucose, 2.5% 139 Urea, 1% 167
- 11. COMPLICATIONS OF IRRIGATION FLUIDS -Glycine- -Normal plasma glycine levels are 13 to 17 mg/L -Transient blindness is attributed to glycine toxicity. -Glycine is a major inhibitory-transmitter acting in the spinal cord and brain- stem. -Glycine also has been implicated in the myocardial depression and hemodynamic changes associated with TURP syndrome. -Ammonia Toxicity- -Absorption of glycine can result in CNS toxicity because of oxidative bio-transformation of glycine to ammonia.
- 12. -Mannitol- -Rapidly expands blood volume and causes pulmonary edema in cardiac patients. -Glucose- -Causes severe hyperglycemia in diabetic patients Distilled Water is electrically inert and inexpensive and has excellent optical properties. -Extremely Hypotonic. -When absorbed into the circulation in large amounts, plain water causes Hemolysis, Shock, and Renal failure. -Thus Isotonic fluids are preferred- ) these solutions are kept slightly hypotonic to preserve transparency(
- 13. ANAESTHETIC CONSIDERATIONS Preoperative Assessment Investigations Choice of Anaesthesia technique
- 14. PREOPERATIVE ASSESSMENT History and Examination: -Cardiovascular- Major risk factors for IHD )HTN, DM, Smoking,Hypercholesterolemia and family history( – can lead to silent perioperative MI. -Heart failure- fluid overload increases risk -Respiratory- Inability to lie flat due to dyspnoea will make awake spinal anaesthesia poorly tolerated. -CNS- Confused patients may not lie still during spinal anaesthesia. -Musculoskeletal- Degenerative changes in vertebral column makes SAB technically difficult. Arthritic joints may get damaged in lithotomy position. Endocrine- rule out h/o DM -Drug history- Beta blockers, ACE inhibitors, Alpha blockers, Warfarin
- 15. INVESTIGATIONS Routine tests required are- -Complete blood count -Creatinine and electrolytes )to detect renal impairment due to obstructive uropathy( -Urine analysis to screen UTI ) increased risk of postoperative septicaemia if left untreated( -ECG for symptomatic patients and routinely for above 60years. -Blood grouping
- 16. Special tests for particular circumstances- --Clotting studies )PT-INR if on Warfarin( --ABG and PFT )if severe respiratory disease suspected( --Chest radiogram )suspicion of metastasis(
- 17. CHOICE OF ANAESTHESIA TECHNIQUE ADVANTAGES DISADVANTAGES REGIONAL ANAESTHESIA 1.Useful in patients with significant respiratory disease 1.Does not prevent penile erection which can interfere with surgery 2.For good post-op analgesia 3.Allows to monitor level of consciousness and detect early signs of TURP syndrome 4.Earlier recognition of bladder perforation or capsular tear 5.Possible reduced blood loss GENERAL ANAESTHESIA 1.Useful in patients who are unable to lie supine for a long time. 1.Position reduces FRC 2.Penile erection can be prevented by deepening of anesthesia 2.Increased risk of aspiration 3.Allows better control of CO2- reduced bleeding 3.Post op analgesia needed
- 18. TECHNIQUE -SUB-ARACHANOID BLOCK -Check for any contraindications of SAB -A fluid preload of 500-1000 ml of warmed NS/RL. -Preloading assists -compensation of spinal induced vasodilatation and hypotension -provides a small sodium load to counter hyponatremia often occuring with TURP -A confirmed block till atleast T10, should be done. -Intraoperative sedation with IV Midazolam can be considered for anxious or confused patients )Early manifestations of TURP syndrome should be kept in mind( -Thermometer, Warming blankets and Fluid warmer should be kept available for detection and prevention of hypothermia due to cold irrigation solutions.
- 19. Subarachanoid anesthesia is generally preferred over continuous Epidural anesthesia for the following reasons: 1- It is technically easier to perform in the elderly 2- Duration of surgery is not generally very long. 3- Incomplete block of sacral nerve roots that occasionally occurs with the epidural technique is avoided with subarachnoid anesthesia.
- 20. GENERAL ANAESTHESIA --Either a spontaneously breathing technique with face mask or Laryngeal mask is used or relaxant technique is appropriate. --Elderly patients are susceptible to hypotensive effects of induction and maintainance agents. --These patients have a reduced requirement for Volatile anesthetic agents as well. --NDMR’s should be used with consideration of possible renal impairment.
- 21. INTRA-OPERATIVE COMPLICATIONS 1-Hypotension 2-TURP syndrome 3-Haemorrhage 4-Perforation of bladder/prostatic capsule 5-Hypothermia 6-Bacteremia and sepsis 7-Complications of positioning 8-Erection
- 22. 1-Hypotension -hypotension following sympathetic blockade of SAB. -uncommon with blocks extending to T10, but high blocks causes resistant hypotension and bradycardia. 2-Haemorrhage -Depends on resection time (2-5ml/min) and size of gland (20-50ml/g) -Bleeding requiring transfusion occurs in about 2.5% of procedures. -Serial hematocrit levels are the most sensitive indicators of the need for transfusion. -Severe blood loss are the result of clotting abnormalities caused by the release of Urokinase from the prostate -Anti-fibrinolytics such as IV Aminocaproic acid (4-5g in first hour, then 1g/hour) IV Tranexamic acid can be used to minimize active blood loss.
- 23. 3-Bladder Perforation -Complicates about 1% of cases. -Most perforations are Extra-peritoneal- result in supra-pubic, inguinal or peri-umbilical pain in the awake patient. The surgeon may notice reduced return of irrigation fluid from the bladder. -Intraperitoneal perforation- less common, but more serious. In these cases the abdominal pain is generalized, and the patient may complain of shoulder-tip pain. (referred from the diaphragm) -Pallor, sweating, nausea and vomiting, and associated hypotension depending on the size of the perforation. -Perforation may present as sudden, unexpected hypotension under general anesthesia. -Management consists of immediate laprotomy and correction of the defect.
- 24. 4-Hypothermia -Use of room-temperature IV fluids and large volumes of irrigation fluids leave elderly patients hypothermic. -All irrigation fluid should be warmed to body temperature prior to use. -Post-operative shivering can cause massively increased myocardial oxygen requirements. 5-Bacteraemia and sepsis Septic shock following TURP is rare. -Antimicrobial prophylaxis - single dose of Gentamicin 3 - 4mg/kg on induction.
- 25. 6-Complications due to Positioning -Lithotomy position- causes nerve compression (especially common peroneal nerve from pressure effects exerted by the stirrups) -Dislocation of hip prostheses. -Compartment syndrome in lower legs -Respiratory compromise in patients with pre-existing lung disease (reduction of functional residual capacity) 7-Erection -Occurs as a result of surgical stimulation due to light planes of anaesthesia -Makes cystoscopy technically difficult. -The erection usually subsides with deepening of anaesthesia.
- 26. TURP SYNDROME -TURP syndrome is a term applied to a constellation of symptoms and signs caused primarily by excessive absorption of irrigating fluid. -Occurs in up to 8% of cases in mild form, but is severe in 1-2% of cases. -Resection of prostatic tissue opens an extensive network of venous sinuses, which allows the irrigation fluid to be absorbed into the systemic circulation.
- 27. Simple principles govern the amount of absorption: 1-Duration of the procedure- 10 to 30 mL of fluid is absorbed per minute of resection time, with as much as 6 to 8 L absorbed in some procedures lasting up to 2 hours. 2-Height of the irrigation fluid bag above the patient (increased height implies increased hydrostatic pressure driving the fluid intravenously) 3-Vascularity of the diseased prostate 4-Capsular or bladder perforation allowing large volumes of irrigation fluid into peritoneal cavity from where it is absorbed
- 28. -Factors which increase the risk of TURP syndrome 1-Pre-existing hyponatraemia or pulmonary oedema 2-Prostate size larger than 60-100g 3-Reduced venous pressure 4-Procedures longer than 1 hour 5-Hydrostatic pressure > 60cm H2O (height of bag above patient( 6-Inexperienced or slow surgeon
- 29. Classical triad of features of TURP syndrome:- 1-Hypertension 2-Bradycardia 3-Altered mental status
- 30. -Investigations required for diagnosis- 1-Serum Sodium- levels below 120mEq/l - symptomatic. 2-ECG – QRS widening, ST segment elevation, T wave inversion ( below sodium levels of 115 mEq/l( 3-Hyperammonemia ( by-product of glycine metabolism(
- 31. Management of TURP syndrome 1-Initial management follows the airway, breathing and circulation (ABC( guidelines. Awake patients need to be sedated and ventilated. 2-Anesthetised patients with mask airways may need intubation and positive pressure ventilation. 3-Surgeon should be informed and surgery terminated
- 32. 4-Initial management of fluid overload and hyponatraemia involves stopping IV fluids. 5-Inj frusemide 40mg IV to promote diuresis. 6-Patients should be closely monitored on an intensive care unit. 7-Hypertonic saline solutions ( 3% or 5%( should be used to increase the serum sodium level by about 1 mmol/l/hour (not exceding an increase of 20mmol/l in the first 48 hours of therapy( 8-Sodium levels should be checked every few hours. Therapy with hypertonic saline should be stopped when symptoms cease or the sodium level reaches 124-132mmol/l. (Rapid correction has been implicated as a cause of central pontine myelinolysis, which causes irreversible brain damage(
- 33. 9-Convulsions should be acutely treated with a benzodiazepine (e.g. diazepam 5-10mg( or small doses of thiopentone (25 - 100mg(. In the presence of intractable seizures, the sodium level may be corrected more rapidly at a rate of up to 8-10mmol/l/hour for the first 4 hours of therapy
- 34. 1-Bladder spasm 2-Blood loss – Usually about 500 ml (2.4-4.6 ml/ min of resection( 3-Clot retention – resulting in bladder distension causing vagal stimulation and pain( 4-Deep vein thrombosis 5-MI 6-TURP syndrome POSTOPERATIVE COMPLICATIONS
- 35. SUMMARY -TURP is a procedure carried out on a predominantly elderly population with a higher incidence of coexisting disease. -A thorough pre-operative assessment is important in detecting at-risk patients, and helping to choose the anaesthetic technique. -SAB is widely considered the most suitable technique, although GA has a similar morbidity and mortality profile. -Subarachnoid block to T10 provides excellent anaesthesia without notable hypotension -TURP syndrome is a rare but potentially fatal complication . Early recognition and prompt treatment are essential. -Blood loss is difficult to quantify and may be significant. Close attention to the patient’s clinical state and communication with the surgeon are vital.