Progresive systemic sclerosis
•Descargar como PPTX, PDF•
14 recomendaciones•7,575 vistas

Progressive systemic sclerosis is a disorder affecting connective tissue in the skin, internal organs, and blood vessels. It is characterized by thickening and tightening of the skin, especially in the fingers and face. It can be classified as limited or diffuse cutaneous disease depending on the extent of skin involvement. Internal organ systems commonly impacted include the lungs, heart, kidneys, and gastrointestinal tract. Management involves treatments for symptoms such as Raynaud's phenomenon, digital ischemia, reflux, and pulmonary hypertension. Prognosis depends on factors like the extent of skin and organ involvement.

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (20)
Similar a Progresive systemic sclerosis
Similar a Progresive systemic sclerosis (20)
Más de Chitralekha Khati
Más de Chitralekha Khati (18)
Último
Último (20)
Progresive systemic sclerosis
- 1. Progressive Systemic Sclerosis ACMS Dept of Medicine 2010 Batch VIII Term
- 2. PSS: Definition • Systemic sclerosis (previously called 'scleroderma') is a generalised disorder of connective tissue affecting- • The skin • Internal organs and • Vasculature.
- 3. PSS: Hallmark The clinical hallmark is the presence of • Sclerodactyly in combination with • Raynaud's phenomenon or • Digital ischaemia
- 4. PSS: Epidemiology • The peak age of onset is in 4th & 5th decades • Overall prevalence is 10-20 per 100 000 • 4:1 female: male ratio
- 5. PSS: Classification It is subdivided into • Diffuse cutaneous systemic sclerosis (DCSS) • Limited cutaneous systemic sclerosis (LCSS) • Many patients with LCSS have features which are phenotypically grouped into the 'CREST' syndrome (calcinosis, Raynaud's, oesophageal involvement, sclerodactyly, telangiectasia).
- 6. PSS: Classification It is subdivided into • Diffuse cutaneous systemic sclerosis (DCSS) • Limited cutaneous systemic sclerosis (LCSS) • Many patients with LCSS have features which are phenotypically grouped into the 'CREST' syndrome (calcinosis, Raynaud's, oesophageal involvement, sclerodactyly, telangiectasia).
- 10. PSS: Etiopathology • Unknown, • No consistent genetic, geographical or racial associations. • Environmental factors are important in isolated cases that result from exposure to –silica dust, –vinyl chloride, –hypoxy resins and –trichloroethylene.
- 11. PSS: Etiopathology Early in the disease there is • Skin infiltration by T lymphocytes • Abnormal fibroblast activation • That leads to increased production of extracellular matrix in the dermis, primarily type I collagen. • This results in symmetrical thickening, tightening and induration of the skin (sclerodactyly).
- 12. PSS: Etiopathology Early in the disease there is –Skin infiltration by T lymphocytes and –Abnormal fibroblast activation • In addition to skin changes there is arterial and arteriolar narrowing due to intimal proliferation and vessel wall inflammation. • Endothelial injury causes release of vasoconstrictors and platelet activation, resulting in further ischaemia.
- 13. PSS Clinical Features and Diagnoais • Systemic sclerosis is predominantly a clinical diagnosis based on the presence of sclerodactyly. • Most patients are ANA-positive, and • Approximately 30% of patients with diffuse disease and • 60% with limited disease have antibodies to topoisomerase 1 and centromere respectively.
- 14. • Cutaneous changes Raynaud's phenomenon is universal and may precede other clinical features.
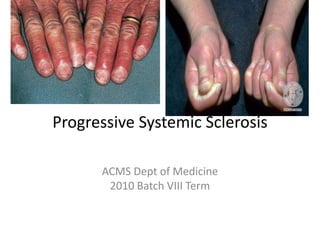
- 15. • Systemic sclerosis. Hands showing tight shiny skin, sclerodactyly, flexion contractures of the fingers and thickening of the left middle finger extensor tendon sheath
- 16. PSS: Skin Disease • The initial phase of skin disease is characterised by non-pitting oedema of the fingers and flexor tendon sheaths. • Subsequently, the skin becomes shiny and taut, and distal skin creases disappear. • There is usually erythema and tortuous dilatation of capillary loops in the nail-fold bed, readily visible with an ophthalmoscope. • The face and neck are usually involved next, with thinning of the lips and radial furrowing. In some patients skin thickening stops at this stage.
- 17. PSS: Skin Disease • Skin involvement restricted to sites distal to the elbow or knee (apart from the face) is classified as 'limited cutaneous disease' or CREST syndrome. • Involvement proximal to the knee and elbow and on the trunk is classified as 'diffuse cutaneous disease'.
- 18. PSS: Skin Disease In extremities- • Intimal fibrosis and vessel wall inflammation may combine to cause critical tissue ischaemia, skin ulceration on pressure points • Localised areas of infarction and • Pulp atrophy at the fingertips.
- 19. PSS: Musculoskeletal features • Arthralgia, morning stiffness and flexor tenosynovitis are common. • Restricted hand function is due to skin rather than joint disease and erosive arthropathy is uncommon. • Muscle weakness and wasting are usually due to myositis.
- 20. PSS: GI FEATURES • Gut involvement is common. • Smooth muscle atrophy and fibrosis in the lower two-thirds of the oesophagus lead to acid reflux with erosive oesophagitis. • Since this may progress to further fibrosis, adequate treatment of reflux (proton pump inhibitors) is important. • Dysphagia and odynophagia (painful dysphagia) may also occur.
- 21. PSS: GI FEATURES • Involvement of the stomach causes early satiety and occasionally outlet obstruction. • Recurrent occult upper GI bleeding may indicate a 'watermelon stomach' (antral vascular ectasia), which occurs in up to 20% of patients. • Small intestine involvement may lead to malabsorption, bacterial overgrowth and intermittent bloating, pain or constipation. • Dilatation of large or small bowel due to autonomic neuropathy may cause pseudo- obstruction.
- 23. PSS: Cardiorespiratory features • Pulmonary involvement is a major cause of morbidity and mortality. • Fibrosing alveolitis mainly affects pts with diffuse disease, esp those with antibodies to topoisomerase 1. • Pulmonary hypertension is a long-standing complication. It is 6X more prevalent in limited than diffuse disease. • The clinical features are rapidly progressive dyspnoea (more than ILD), RHF and angina with- • often rapidly progressing digital ischaemia.
- 24. PSS: Cardiorespiratory features Treatment strategies include • Vasodilators • Continuous infusions of epoprostenol • The oral endothelin 1 antagonist bosentan and • Heart-lung transplantation.
- 25. PSS: Renal features • Main cause of death is hypertensive renal crisis (rapidly developing malignant hypertension and renal failure). • Treatment is by ACE inhibition even in presence of renal impairment. • Hypertensive renal crisis is more likely in patients with diffuse rather than limited disease. • It is also more prevalent in patients with topoisomerase 1 antibodies. • Clinicians use prophylactic ACE Is for diffuse disease to prevent this manifestation.
- 26. PSS: Management and prognosis Five-year survival is approx70%. Risk factors for a poor prognosis include • Older age • Diffuse skin disease • Proteinuria • High ESR • A low gas transfer factor for carbon monoxide (TLCO) and • Pulmonary hypertension
- 27. PSS: Management and prognosis • Self-management to maintain core body temperature and avoid peripheral cold exposure is important. • Infection of ulcerated skin should be treated with prompt antibiotic therapy. • Antibiotics penetrate poorly into the skin lesions of systemic sclerosis and therefore need to be given at higher dose for longer periods (e.g. flucloxacillin 500 mg 6-hourly for 14 days).
- 28. PSS: Management and prognosis • Calcium antagonists (e.g. nifedipine, amlodipine) or angiotensin II receptor antagonists (e.g. valsartan) may be effective for Raynaud's symptoms. • For severe digital ischaemia, intermittent infusions of epoprostenol may be helpful.
- 29. PSS: Management and prognosis • Corticosteroids and cytotoxic drugs are indicated in patients with myositis or alveolitis. • No agent has been shown to arrest or improve skin changes.
Notas del editor
- P450, a mechanism that is less likely to produce toxic intermediates. Adva-27a is an excellent inhibitor of Topoisomerase II with an IC50 of ... Topoisomerases (type I: EC 5.99.1.2, type II: EC 5.99.1.3) are enzymes that regulate the overwinding or underwinding of DNA. The winding problem of DNA ...