Complication of ascitis
•Descargar como DOCX, PDF•
1 recomendación•379 vistas

Complication of ascitis Approach & Management of some of them

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Complication of ascitis
Similar a Complication of ascitis (20)
Último
Último (20)
Complication of ascitis
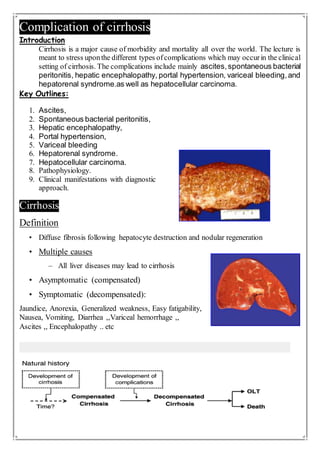
- 1. Complication of cirrhosis Introduction Cirrhosis is a major cause of morbidity and mortality all over the world. The lecture is meant to stress uponthe different types ofcomplications which may occurin the clinical setting of cirrhosis. The complications include mainly ascites,spontaneous bacterial peritonitis, hepatic encephalopathy, portal hypertension, variceal bleeding,and hepatorenal syndrome.as well as hepatocellular carcinoma. Key Outlines: 1. Ascites, 2. Spontaneous bacterial peritonitis, 3. Hepatic encephalopathy, 4. Portal hypertension, 5. Variceal bleeding 6. Hepatorenal syndrome. 7. Hepatocellular carcinoma. 8. Pathophysiology. 9. Clinical manifestations with diagnostic approach. Cirrhosis Definition • Diffuse fibrosis following hepatocyte destruction and nodular regeneration • Multiple causes – All liver diseases may lead to cirrhosis • Asymptomatic (compensated) • Symptomatic (decompensated): Jaundice, Anorexia, Generalized weakness, Easy fatigability, Nausea, Vomiting, Diarrhea ,,Variceal hemorrhage ,, Ascites ,, Encephalopathy .. etc
- 2. Examination Findings • Spider angiomatas • Palmar erythema • Gynecomastia • Testicular atrophy • Leuconychia • Parotid gland hypertrophy • Dupuytren’s contractures • Clubbing • Jaundice Portal Hypertension Increased intrahepatic vascular resistance Fixed component Sinusoidal fibrosis Compression by regenerative nodules Functional component Vasoconstriction Deficiency in intrahepatic NO Enhanced activity of vasoconstrictors Portal Venous Pressure (PVP) Normal = 5-10 mm Hg Hepatic Venous Pressure Gradient (HVPG) = portal venous pressure - hepatic venous pressure or RA pressure Normal = 1-5 mm Hg
- 3. Classification Pre hepatic: Portal or splenic vein thrombosis Intrahepatic • Presinusoidal Schistosomiasis • Sinusoidal Cirrhosis • Postsinusoidal Veno-occlusive disease Post hepatic Hepatic vein thrombosis Constrictive pericarditis Varices : Common lethal complication 50% of patients with cirrhosis More likely to bleed in more decompensated disease Varices: Portosystemic Collateral Formation • Esophageal varices • Caput medusa • Rectal varices Variceal Bleed: Risk Factors • High Gradient • Large esophageal varices • Endoscopic features – red wale markings – cherry red signs Treatment • Primary prophylaxis (never bled) – If no varices: no need for nonselective B blocker – If small varices: no long term evidence to use B blocker unless red signs present
- 4. – If large varices: • High risk patient (red wale, childs B/C): B blocker (nadolol/ propranolol) or prophylactic banding • Low risk patients: B blocker • Titrate B blocker to max tolerated dose • Blood transfusion: • Antibiotics: norfloxacin, IV cipro, ceftriaxone (probably best) • Vasopressin, telipressin, octreotide, vapreotide x 3-5 days – Splanchnic vasoconstriction, reduced portal flow • EGD within 12 hours – Banding(almost always) or sclerotherapy (rare) • Balloon Tamponade (Blakemore / Minnesota tube) temporizing measure for up to 24 hours • TIPS • Secondary prophylaxis – All patients who have has a variceal bleed – Combination of B Blocker and serial banding – Continue banding (usually outpt) until varices are eradicated Ascites Fluid within the peritoneal cavity Occurs in 50-60% of patients with cirrhosis over 10-15 years Pathophysiology Elevated Hydrostatic Pressure • Cirrhosis • Congestive heart failure • Constrictive pericarditis • Hepatic outflow block
- 5. Decreased Oncotic Pressure • Nephrotic syndrome • Protein-losing enteropathy • Malnutrition • Cirrhosis Peritoneal Fluid Production > Resorption • Infections (bacterial, tuberculosis, fungal) • Neoplasms CP • Abdominal distention • Bulging flanks • Shifting dullness • Fluid wave • Fluid detected on US or CT scan Serum-Ascites Albumin Gradient ≥1.1 caused by portal hypertension <1.1 others e.g. -Nephrotic syndrome, TB… etc. Treatment of Ascites • Usually responds to Na restriction and diuretics – When SAAG >1.1 • Dual diuretics: – Furosemide AND Spironolactone • Single daily dosing (40/ 100) • Na restriction <2000mg/day • Fluid restriction is usually NOT necessary
- 6. In refractory ascites… • AVOID – ACE inhibitors / angiotensin receptor blockers • Blood pressure / adverse renal effects – Propranolol • Blood pressure / circulatory dysfunction during LVP • Renal function – Consider risks benefits – NSAIDS Large / Tense ascites • Therapeutic paracentesis followed by diuretics / Na restriction • 6-8 g/of albumin per liter of ascites removed • Midodrine may be helpful – Shown to increase BP, survival benefit • Consideration of liver transplantation referral Spontaneous Bacterial Peritonitis (SBP) Infectious complications of cirrhosis 1. Spontaneous bacterial peritonitis (SBP) 2. Urinary tract infection 3. Pneumonia 4. Bacteremia SBP 7-25% of hospitalized cirrhotics – In-hospital mortality 20-50% Recurrence of SBP 30-70% Eschericia coli 43% Miscellaneous 20% Klebsiella pneumoniae 8%
- 7. Streptococcus pneumoniae 8% Group D stretocococcus 8% Alpha-hemolytic streptococcus 5% Miscellaneous Enterobacteriaceae 3% Tap all patients admitted to hospital or for any reason rub you the wrong way… • Diagnosis: – Culture NOT needed (but send it anyways) – PMN >250cells/mm3 • Treatment: – 3rd gen cephalosporin i.e. cefotaxime 2g q8 – Albumin 1.5g/kg day 1 and 1.0 g/kg day 3 • Cr >1, BUN >30, or bilirubin >4 SBP : prevention • GIT bleed and cirrhosis – Ceftriaxone or Norfolk x 7 days • If prior episode of SBP, long term prophylaxis – Daily Norfloxacin or Bactrim Hepatic Encephalopathy Reversible alteration in the neuropsychiatric function • Due to shunting of neurotoxic nitrogenous products • Lack of hepatic detoxification • 10-50% of cirrhotics • 40% survival 1 year after 1st episode • 15% survival 3 years after 1st episode • Disturbance in diurnal sleep pattern precedes neurologic signs • 15-30% have abnormal NCT or abnormal EEG without overt encephalopathy
- 8. Treatment • Lactulose – First line – 2-3 softBM/ day • Rifaximin – Reduced ammonia producing bacteria Long Term Management of HE • After initial HE event – Usually on therapy indefinitely or until liver transplant – Long term use of lactulose and or rifaximin • High protein diet is OK (and preferred in cirrhosis) • Patients with HE should NOT undergo TIPS if possible Hepatorenal Syndrome Pathophysiology • Occurs in setting of cirrhosis and ascites • Severe renal arterial vasoconstriction • Compromised glomerular filtration rate • Normal kidney structure • Advanced liver disease: cirrhosis, alcoholic hepatitits, fulminant hepatitis • Sometimes precipitated by overdiuresis, GI bleed, use of nephrotoxic agents
- 9. Clinical Features • Ascites • Oliguria • Hypotension •Jaundice Course • Typically death within weeks • HRS Type 1 • Rapidly progressive • Precipitating event frequent, esp SBP • Very short survival • HRS Type 2 • Slow onset of moderate renal insufficiency • Poor response to diuretics (refractory ascites) • Longer survival Diagnostic Criteria 1. Cirrhosis with ascites 2. Serum CR >1.5 mg/dL 3. No improvement in serum CR after at least 2 days of diuretic withdrawal & volume expansion with albumin (max 100g/day) 4. Absence of shock 5. No current or recent nephrotoxic drugs 6. Absence of parenchymal kidney disease Treatment Treatment principles Treat the underlying precipitant promptly More quickly addressed the more likely to have improvement in HRS Have a high suspicion for an occult precipitating event in any liver patient who has ARF
- 10. - Even with removal of the precipitant, HRS may be irreversible 1. Renal vasodilators 2. Systemic vasoconstrictors 3. TIPS 4. Dialysis 5. Transplantation Hepatocellular Carcinoma • Seen in cirrhosis – Exception: HBV (can be noncirrhotic) • Diagnosis by US, CT scan, MRI – Histology is not essential • Alpha-fetoprotein level may be elevated • Surveillance – Screen all patients with cirrhosis for HCC • Up to 8% risk of HCC/year – Also male HBV carriers >40 and female HBV >50 (even if they don’t have cirrhosis) Diagnosis • Usually with imaging, histology used less often • If lesion seen on u/s> 1cm then follow up with CT or MR • If hyper vascular lesion that washes out on portal venous phase then dx with HCC
- 11. Treatment of HCC 1. Resection Less commonly used Noncirrhotic or very well compensated Well preserved synthetic function (INR near normal) Normal bilirubin Low portal pressure Possibly for noncirrhotic HBV patient. 2. Liver transpantation 3. Systemic – Sorafenib Last resort 4.Local ablation – Alcohol injection • Only in smaller tumors • Not used very often – Radiofrequency ablation • Better for larger tumors – May use as a bridge to liver transplantation • Transarterial Chemoebolization (TACE) – Non curative – Nonsurgical patients – Large multifocal HCC – No vascular invasion – No extrahepatic spread
- 12. 5.Liver transplantation – Curative approach – Milan Criteria • 1 tumor <5cm • Up to 3 tumors <3cm • No vascular / extrahepatic spread Conclusions • The transition from compensated cirrhosis to decompensated cirrhosis carries a significant change in mortality • Clinical diagnosis is important • Simultaneous compications may (and usually arise) References: Kumar and Clark's Clinical Medicine. USMLE CK book Macleod's clinical examination. Davidson's principles of clinical practice. medicinenet.com webmd.com
- 13. Supervisedby : Tropical Medicine Department Prepared by: Eslam Emad Awesh