3. INTRODUCTION
ORAL MUCOSA CONSISTS OF
★ Masticatory mucosa
★Specialized mucosa
★Oral mucous membrane lining
the remained of the oral cavity
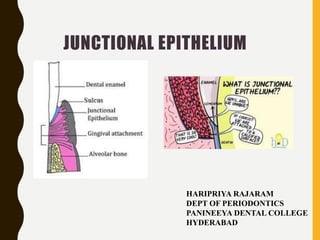
4. • The gingiva is composed of gingival epithelium and gingival
connective tissue.
• Furthermore, the gingival epithelium is in turn classified into
the
☛ oral epithelium: covers the crest
and outer surface of marginal gingiva and
attached gingiva
☛ sulcular epithelium : lines the gingival
Sulcus.
☛junctional epithelium: which provides the
contact between the gingiva and the tooth.
5. HISTORICAL ASPECT
• Gottlieb (1921) had reported that the "epithelial
attachment" is organically united to the tooth
surface.
6. • Waerhaug (1952) concluded that the "epithelial
attachment" belongs to the lining of the "physiological
pocket", that its cells adhere only weakly to the tooth
surface, and that the bottom of that pocket is to be found at
the cemento-enamel junction
7. WAERHAUG’S CONCEPT (1960)
• He presented the concept of epithelial cuff. This concept
was based on insertion of thin blades between the surface of
tooth and the gingiva.
• Blades could be easily passed apically to the connective
tissue attachment at CEJ without resistance.
• Itwas concluded that gingival tissue and tooth are
closely adapted but not organically united.
8. SCHROEDER AND LISTGARTEN CONCEPT
(1971)
• Primary epithelial attachment refers to the epithelial
attachment lamina released by the REE. Itlies in direct
contact with enamel and epithelial cells attached to it by
hemi-desmosomes.
• When REE cells transform into JE cells the primary
epithelial attachment becomes secondary epithelial
attachment. Itis made of epithelial attachment between
basal lamina and hemi-desmosomes
9. SCHROEDER AND LISTGARTEN (1977)
Clarified the anatomy and
histology of dentogingival
junction in their monograph Fine
structure of developing
epithelial attachment of human
teeth.
MAX LISTGARTEN
10. DEFINITION
Junctional epithelium isthe non keratinized stratified squamous
epithelium which attaches and form a collar around the
cervical portion of the tooth that follows CEJ.
-Carranza
A single or multiple layer of non keratinizing cells adhering
to the tooth surface at the base of the gingival crevice.
Formerly called epithelial attachment.
-Glossary of periodontal terms- AAP 4th
edition
12. • As the erupting tooth approaches the oral epithelium, the
cells of the outer layer of the reduced dental epithelium
(RE), as well as the cells of the basal layer of the oral
epithelium (OE), show increased mitotic activity and start
to migrate into the underlying connective tissue..
13. • When the tooth has penetrated into the oral cavity, the
REE cells transform into flat cells forming junctional
epithelium. The cervical region of the enamel, however, is
still covered by ameloblasts (AB) and outer cells of the
reduced dental epithelium.
14. • During the later phases of tooth eruption, all cells of the
reduced enamel epithelium are replaced by a junctional
epithelium (JE). This epithelium is continuous with the
oral epithelium and provides the attachment between the
tooth and the gingiva.
15. ANATOMICAL FEATURES
• Junctional epithelium consists of a collar like band of
stratified squamous non keratinizing epithelium.
• It is 3-4 layers thick in early life but, but the number
increases with age to 10 or even 20 layers.
• It tapers from coronal end to its apical end, which is
located at the CEJ in the healthy tissue.
• Periodontal ligament limits its apical extent, and
coronally it is continuous with sulcular epithelium
• The length of junctional epithelium ranges from 0.25 to
1.35 mm
16. DENTOGINGIVAL UNIT
• The attachment of the junctional epithelium to the tooth is
reinforced by the gingival fibers, which brace the marginal
gingiva against the tooth surface.
• For this reason, the junctional epithelium and the gingival
fibers are considered together as a functional unit referred
to as the dentogingival unit.
17. MICROSCOPIC FEATURES
Non-keratinizing stratified squamous epithelium is made up of two
strata: basal layer and the supra-basal layer
• Basal layer – consisting of cuboidal cells, are arranged along the
connective tissue interface
• Supra-basal layer – multiple layers of flattened cells lying parallel to
tooth surface
18. Junctional epithelium is attached to
1.gingival connective tissue - external basal lamina
2. tooth surface - internal basal lamina.
19. • External basal lamina contains the structures similar to that of
typical basement membrane, with the lamina densa supporting
the underlying connective tissue and lamina lucida lying in
between the lamina densa and the basal cells.
• Internal basal lamina lacks true basement membrane
components like: collagen IV and VII, laminin 1 while it
contains laminin 5 and type VIII collagen (usually absent in
typical basement membrane); hence it is considered as a
specialized extracellular matrix.
20. • The single layer of cell, lying in
contact with tooth surface, is referred
to as DAT (Directly attached to
tooth) cells
• Salonen JI in the year 1994 proved
the proliferative potential of these
cells in his study.
• The existence of a proliferating
population of epithelial cells (DAT
cells) in a supra-basal location,
several layers away from the
connective tissue, is a unique
feature of the junctional
epithelium.
22. FEATURES OF JUNCTIONAL EPITHELIAL
CELLS:
• These cells contain dense cytoplasm
• abundant amount of
1. rough endoplasmic reticulum,
2. Golgi complex (LARGE)
3. lysosomal bodies
4. polyribosomes .
• few tonofilaments
• Absence of
1. Keratinosomes (ODLAND BODIES)
2. Acid phosphatase
23. • Cytokeratins (CK) are the intermediate filament proteins
of cytoskeletal family and form the main structural
proteins of these Junctional epithelial cells . They express
CK5,CK10, CK13, CK 14, CK16 and CK19 .
• The expression of CK19 being high, found in almost all
the layers of junctional epithelium, have been regarded as
the characteristic histological marker for Junctional
epithelium .
24. • The cells exhibit relatively loose intercellular junctions
comprising of few desmosomes, adherens junctions and
occasional gap junctions . The fluid-filled inter-cellular spaces
are responsible for remarkable permeability .
• Intercellular spaces are occupied by mononuclear leukocytes
of varied nature. Different types of cells like the polymorpho
nuclear leukocytes, lymphocytes, macrophages, antigen-
presenting cells, Langerhans cells are seen to exist in and
around the junctional epithelium cells
• It is also being innervated by sensory nerve fibers.
25. Characteristics OuterOral
epithelium
Sulcularepithelium Junctional
epithelium
Origin Oral epithelium Oral epithelium Reduced enamel
epithelium
Keratinization Parakeratinized
Sometimes
orthokeratinized
Nonkeratinized Nonkeratinized
Stratification Well stratified Stratified but
granulosamand
corneum are
absent
Poorlystratified
Proliferation Lesserproliferation
among three
Higher than OEE
but lesser thanJE
Higherproliferation
Permeability Not permeableto
water soluble
substances
Moderately
permeable
Highlypermeable
IntercellularSpace
Desmosomes&
tonofilaments
Narrowest
More thanSE&JE
Narrower thanJE
More thanJE
Widestamong
three
Least among three
Retepegs Present Normallyabsent,
appears in
inflammation
Normallyabsent,
appears in
inflammation
DIFFERENCES BETWEEN THE EPITHELIUM
26. EPITHELIALATTACHMENT APPARATUS
• The gingiva (specifically junctional epithelium) is adherent
to tooth through a structural complex, referred to as
epithelial attachment apparatus
• This consists of
[1]hemidesmosomes
[2] a basal lamina, i.e. internal basal lamina, to which the
cells are attached through hemidesmosomes
27. HEMIDESMOSOMES
• Hemidesmosomes have a decisive role in the firm
attachment of the cells to the internal basal lamina on the
tooth surface
• The hemidesmosome comprises of an attachment plaque,
cytokeratin filaments and a sub-basal lamina dense plate
The interaction between IBL and cell
surface macro-molecule helps in cell
motility, adhesion, synthetic capacity,
tissue stability, regeneration and response
to external signal
28. MOLECULAR ASPECT OF JUNCTIONAL
EPITHELIUM
CELL ADHESION MOLECULES
MOLECULAR FACTOR FUNCTION
INTEGRINS
MEDIATE CELL MATRIX AND
CELL-CELL INTERACTION
EPITHELIAL CADHERIN intercellular adhesion
structural integrity
CEACAM1
(carcino embryonic Ag- related cell
adhesion molecule 1)
Adhesion between epithelial cells;
guidance of PMNs through the
junctional epithelium;
regulation of cell proliferation,
stimulation, and co-regulation of
activated T-cells;
cell receptor for certain bacteria
CAM-1 Mediates cell-cell interactions in
inflammatory reactions; guiding
PMNs toward the sulcus bottom
29. Interleukin-8 Chemotaxis; guiding PMNs toward
the sulcus bottom
Interleukin-1
Tumor necrosis factor
Pro-inflammatory cytokines that
contribute to the innate immune
defense
CYTOKINE
GROWTH FACTORS AND CORRESPONDING RECEPTORS
Epidermal growth factor
(EGF)
Mitogen that participates in epithelial growth,
differentiation, and wound healing
Epidermal growth factor
receptor (EGFR)
Signal transduction
30. PROTEASES
Tissue plasminogen activator (t-PA) Serine protease that converts
plasminogen into plasmin, which in
turn degrades extracellular matrix
proteins and activates matrix
metalloproteinases
MMP-7 OR MATRILYSIN Proteolytic degradation of the
extracellular matrix
NATURAL ANTIMICROBIAL PEPTIDES
AND PROTEINSα-defensins PMN-produced antimicrobial
substances that contribute to the
innate immune defense
Human -defensin Epithelially produced antimicrobial
substances that contribute to innate host
defense
31. FUNCTIONS
• Barrier: junctional epithelium forms a dynamic seal
around the tooth, protecting delicate periodontal tissues
from external environment, and acts as a physical barrier.
• Rapid turnover: junctional epithelium shows
exceptionally high turnover rate, which not only
maintains a structural integrity but also adapts itself as per
need.
• Anti-microbial function: junctional epithelium has no
keratinized layer at its free surface, some special structural
and functional characteristics compensate for absence of
this barrier, thereby help to maintain a potent anti-
microbial mechanism, which is a unique property of J.E
32. TURN OVER OF JUNCTIONAL EPITHELIAL CELLS
• The turnover rate of junctional epithelium is exceptionally rapid
• Previously it was thought that only epithelial cells facing the
external basal lamina were rapidly dividing. However, recent
evidence indicates that a significant number of the DAT cells
are, like the basal cells along the connective tissue, capable of
synthesizing DNA, which demonstrates their mitotic activity .
33. • At the coronal part of the junctional epithelium, the DAT cells
typically express a high density of transferrin receptors
which supports the idea of their active metabolism and high
turnover
• The existence of a dividing population of epithelial cells (DAT
cells) in a suprabasal location, several layers from the
connective tissue, is a unique feature of the junctional
epithelium. The distinct phenotype may result from specific
permissive or instructive signals provided by the internal
basal lamina matrix on the tooth surface.
34. POSSIBLE PATHWAYS
FOR TURN OVER OF DAT
CELLS
(1).The daughter cells produced by
dividing DAT cells replace degenerating
cells on the tooth surface
(2) the daughter cells enter the exfoliation
pathway and gradually migrate coronally
between the basal cells and the DAT cells
to eventually break off into the sulcus, or
(3) epithelial cells move/migrate in the
coronal direction along the tooth surface
and are replaced by basal cells migrating
round the apical termination of the
junctional epithelium.
35. JUNCTIONAL EPITHELIUM IN THE
ANTIMICROBIAL DEFENCE
1.In the coronal part, rapid cell exfoliation occurs due to
high turn over rate and funneling of cells towards the
sulcus prevents bacterial colonization .
2. Laterally, the (external) basal lamina forms an effective
barrier against invading microbes .
3. Active antimicrobial substances are produced in junctional
epithelial cells.
These include defensins and lysosomal enzymes
36. • Epithelial cells activated by microbial substances
secrete chemokines, e.g. interleukin- 8 and
cytokines, e.g. interleukins -1 and -6, and tumour
necrosis factor-∝ that attract and activate professional
defense cells, such as lymphocytes (LC) and
polymorpho- nuclear leukocytes (PMN).
37. • Recently, it has been found that the junctional epithelial
cells lateral to DAT cells produce matrilysin (matrix
metalloproteinase-7). It has the following effects.
1. this enzyme is able to activate the precursor peptide of ∝-
defensin, an important antimicrobial agent of mucosal
epithelium .
2. release of bioactive molecules from the cell surfaces
which play a role in the inflammatory reaction
38. (1)because of rapid cell division
(2)and funnelling of junctional
epithelial cells towards the
sulcus hinder bacterial
colonization.
(3)Laterally, the (external)
basement mem- brane forms
an effective barrier against
invading microbes
(4) Active antimicrobial
substances are produced in
junctional epithelial cells.
These include defensins and
lysosomal enzymes
39. (5)Epithelial cells activated by
microbial substances secrete
chemokines, e.g. interleukin- 8
and cytokines, that attract and
activate professional defense cells,
such as lymphocytes (LC) and
polymorpho- nuclear leukocytes
(PMN). Their secreted product, in
turn, cause further activation of
the junctional epithelial cells
.
40. • The GCF passing through the junctional
epithelium determines the
environmental conditions and provides
sufficient nutrients for the DAT cells to
grow.
• The main route for GCF diffusion is
through the (external) basement
membrane and then through the
relatively wide intercellular spaces of
the variable thickness junctional
epithelium into the sulcus.
ROLE OF GCF
41. • During inflammation the GCF flow increases and its
composition starts to resemble that of an inflammatory
exudate
• The increased GCF flow contributes to host defense by
flushing bacterial colonies and their metabolites away
from the sulcus, thus restricting their penetration into the
tissue
44. ESTABLISHED LESION:
1.Widened intercellular spaces that
are filled with granular , cellular
debris from disrupted neutrophils,
lymphocytes and monocytes.
2. Rete pegs protrude into the
connective tissue and basal lamina
is destroyed in some areas.
45. ROLE OF JUNCTIONAL EPITHELIUM IN INITIATION OF
POCKET FORMATION
• Conversion of junctional epithelium to pocket epithelium is
regarded as a hallmark in the development of
periodontitis
• the initiation of pocket formation may be
attributed to the detachment of the DAT
cells from the tooth surface or to the
development of an intra-epithelial split
46. • With increasing degrees of gingival inflammation, both the
emigration of PMNs and the rate of gingival crevicular
fluid passing through the intercellular spaces of the
junctional epithelium increases causing focal
disintegration.
• In contrast, the bacteria and their products also have the
opportunity to enter the junctional epithelium .
47. • Among the virulence factors produced by P. gingivalis,
gingipains specifically degrade components of the
epithelial cell-to-cell junctional complexes .
• The proteolytic disruption of the epithelial integrity may
not only be a significant factor in the initiation of pocket
formation, but may also pave the way for bacterial
invasion into the sub- epithelial connective tissue in
advanced stages of the lesion.
48. Apical shift of junctional epithelium: collagenase released
by various cells such as fibroblasts, PMNs and macrophages
degrade the collegen matrix.
Apical cells of JE proliferate along the root surface and
extend finger like projections that are 2-3 cell in thickness.
49. Coronal detatchment of junctional epithelium :
As a result of inflammation , the PMNs invade the coronal
end of junctional epithelium in increasing numbers. When
the relative volume of PMNs reach 60% or more of
junctional epithelium , the epithelium loses its cohesiveness
and detatches from the tooth surface.
apical shift of JE
50. CHANGES SEEN IN JUNCTIONAL EPITHELIUM IN
PERIODONTAL POCKET:
• JE at the pocket is much shorter than JE at base of normal
sulcus.
• Slight degenerating changes,
51. REGENERATION OF JUNCTIONAL
EPITHELIUM
Injury to junctional epithelium may occur due to:
Accidental trauma
• Toothbrushing
• Flossing
• Eating
Intentional
• Periodontal surgery
52. • Following probing, a new and complete attachment
indistinguishable from that in controls was established 5 days
after complete separation of the junctional epithelium from the
tooth surface (Taylor and Campbell, 1972)
• Waerhaug (1981) studied healing of the junctional epithelium
after the use of dental floss at premolars in 12-year-old
humans. Then new attachment of junctional epithelial cells
started 3 days after flossing ceased. Finally the cell populations
on the experimental and control surfaces were again
indistinguishable after two weeks
• In general, a new junctional epithelium after gingivectomy
forms within 20 days
53. LONG JUNCTIONAL EPITHELIUM
• If the epithelium proliferates along the root surface before
other tissues, it results in the formation of long junctional
epithelium.
• The long junctional epithelium consists of two or three
layers aligned parallel to the tooth surface.
• This epithelium attaches to the cementum surface by
hemidesmosomes and the basal lamina. The epithelium is
permeable due to its wide intercellular spaces.
54. • Fewer capillaries underneath the long junctional
epithelium are evident than in the normal junctional
epithelium
• Listgarten et al. suggested that the long junctional
epithelium is a transient feature of the healing process on
the road to connective tissue attachment, but it is not a
final healing stage
55. BIOLOGIC WIDTH
• BIOLOGIC WIDTH is defined as the dimension of the
soft tissue which is attached to the portion of the tooth
coronal to the crest of the alveolar bone.
• It is important from the restorative point of view because
its violation leads to complications like gingival
enlargement alveolar bone loss and improper fit of the
restoration.
56. • The average histological width of connective tissue
attachment was 1.07mm. The mean average length of
epithelial attachment was 0.97mm with the range of
0.71mm-1.35mm.
• The average combined histological width of connective
tissue attachment and junctional epithelium was
2.04mm, which is referred to as the BIOLOGIC
WIDTH
57. JUNCTIONAL EPITHELIUM AROUND IMPLANTS
• The junctional epithelium
around implants always
originates from epithelial
cells of the oral mucosa, as
opposed to the junctional
epithelium around teeth which
originates from the reduced
enamel epithelium .
58. • Structurally the peri implant epithelium closely resembles
the junctional epithelium around teeth
• Marker molecules involved in the defense mechanisms
against the bacterial challenge are also expressed in the
peri-implant epithelium .Eg: t- PA , ICAM-1, and a
cytokeratin profile .
60. ROLE OF JUNCTIONAL EPITHELIUM IN
PASSIVE ERUPTION
Passive eruption is the exposure of the teeth by apical
migration of the gingiva.
STAGE 1
• The teeth reach the line of occlusion.
• The junctional epithelium and
base of the gingival
sulcus are on the enamel.
61. STAGE 2
• The junctional epithelium proliferates so that part is
on the cementum and part is on the enamel.
• The base of the sulcus is still on the enamel.
62. STAGE 3
• The entire junctional epithelium is on the cementum,
and the base of the sulcus is at the cementoenamel
junction.
63. STAGE 4
• The junctional epithelium
has proliferated farther on
the cementum.
• The base of the sulcus is on
the cementum, a portion of
which is exposed.
• Proliferation of the
junctional epithelium onto
the root is accompanied by
degeneration of gingival and
periodontal ligament fibers
and their detachment from
the tooth.
64. CONCLUSION
• Junction epithelium is important because of its anatomic
location.
• It is a site of host bacterial interaction in the initiation of
periodontal disease.
• Conversion of junctional epithelium to pocket epithelium is
considered as a hallmark in the initiation of periodontitis.
• Hence , a thorough knowledge of junctional epithelium is
essential to prevent the initiation of periodontal disease.
65. REFERENCES
• Carranza’s Clinical periodontology-11th edition
• Carranza’s Clinical periodontology- 13th edition
• Clinical periodontology and Implant dentistry-Jan Lindhe,
6th edition
• Orbans Oral histology and embryology
• DD Bosshardt and NP Lang. The Junctional Epithelium:
from health to disease. J Dent Res 2005.
66. • Marja T Pollanen, Jukka I Salonen, Veli- Jukka Uitto. Structure and
function of the tooth–epithelial interface in health and disease .
Periodontology 2000. 2003 ; 31:12–31 .
• Masaki Shimono , Tatsuya Ishikawa , Yasunobu Enokiya , Takashi
Muramatsu et al. Biological characteristics of the junctional epithelium
. Journal of Electron Microscopy.2003; 52(6): 627–639.
• Hubert E. Schroeder and Max A. Listgarten. The Junctional Epithelium:
From Strength to Defense . J Dent Res .2003; 82(3):158- 161
• Anindya Priya Saha , Sananda Saha , Somadutta Mitra. Junctional
Epithelium: A dynamic seal around the tooth Journal of Applied
Dental and Medical Sciences . 2018 ; 4(3): 2454-2288