This student "cheat sheet" is designed to provide medical students with basic information regarding the diagnosis and treatment of Hypertension. It includes Questions to Ask, what to look for on a Physical Exam, Labs to Order, and basic Treatment Plans.
These guides are particularly designed for first and second-year medical students as an introduction to primary care and ambulatory care medicine and attempts to tie in the basic pathophysiology that is high-yield for USMLE Step 1.
Any and all feedback is very welcomed.
Kodo Millet PPT made by Ghanshyam bairwa college of Agriculture kumher bhara...
Hypertension Cheat Sheet
1. Revised 8/17/14. Email justin.berk@ttuhsc.edu with any feedback.
HYPERTENSION CHEAT SHEET
A chronic disease of elevated arterial pressure- a measurement of how hard the heart has to work.
“Primary” hypertension accounts for 95% of hypertension –mechanism is not understood.
Systolic – arterial pressure when heart contracts | Diastolic – arterial pressure when heart relaxes
How to take an ideal blood pressure
- No nicotine/caffeine for 30 minutes
- Patient should be sitting for 5 minutes
- Free of restrictive clothing
- Appropriate cuff size
Other factors that BP: full bladder, unsupported back/feet, crossed legs, cuff over clothing, unsupported arm, conversation.
Risk factors for hypertension
- Ethnicity (Black)
- Family history
- Excess sodium intake
- Sedentary lifestyle
- Obesity
- High cholesterol
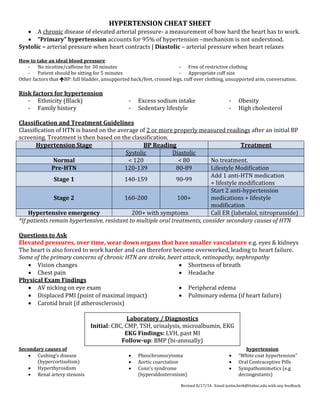
Classification and Treatment Guidelines
Classification of HTN is based on the average of 2 or more properly measured readings after an initial BP
screening. Treatment is then based on the classification.
Hypertension Stage BP Reading Treatment
Systolic Diastolic
Normal < 120 < 80 No treatment.
Pre-HTN 120-139 80-89 Lifestyle Modification
Stage 1 140-159 90-99
Add 1 anti-HTN medication
+ lifestyle modifications
Stage 2 160-200 100+
Start 2 anti-hypertension
medications + lifestyle
modification
Hypertensive emergency 200+ with symptoms Call ER (labetalol, nitroprusside)
*If patients remain hypertensive, resistant to multiple oral treatments, consider secondary causes of HTN
Questions to Ask
Elevated pressures, over time, wear down organs that have smaller vasculature e.g. eyes & kidneys
The heart is also forced to work harder and can therefore become overworked, leading to heart failure.
Some of the primary concerns of chronic HTN are stroke, heart attack, retinopathy, nephropathy
Vision changes
Chest pain
Shortness of breath
Headache
Physical Exam Findings
AV nicking on eye exam
Displaced PMI (point of maximal impact)
Carotid bruit (if atherosclerosis)
Peripheral edema
Pulmonary edema (if heart failure)
Secondary causes of hypertension
Cushing’s disease
(hypercortisolism)
Hyperthyroidism
Renal artery stenosis
Pheochromocytoma
Aortic coarctation
Conn’s syndrome
(hyperaldosteronism)
“White coat hypertension”
Oral Contraceptive Pills
Sympathomimetics (e.g
decongestants)
Laboratory / Diagnostics
Initial: CBC, CMP, TSH, urinalysis, microalbumin, EKG
EKG Findings: LVH, past MI
Follow-up: BMP (bi-annually)
2. Revised 8/17/14. Email justin.berk@ttuhsc.edu with any feedback.
TREATMENT
PHARMACOTHERAPY - FIRST LINE MEDS: diuretics, ACEI/ARBs, CCBs
Class Example Mechanism Notes
ACE-Inhibitor Lisinopril
Block Angiotensin
converting enzyme
Dry cough, angioedema
(2/2 inhibition of
bradykinin). Cr , K+
Angiotensin 2 receptor
blockers (ARBs)
Losartan Blocks AT2 receptors K+
Renin is secreted
by kidneys when
they perceive
hypoperfusion.
Renin stimulates
AT1 which is
converted to AT2
by ACE in the lung.
AT2 is a
vasoconstrictor
and stimulates
formation of
aldosterone
(which increases
BP through sodium
retention).
Calcium Channel
Blocker (CCB)*
Nifedipine
Blocks smooth muscle
vasoconstriction
Edema
Thiazide Diuretic
Hydrochlorothiazide
(HCTZ)
Increases natriuresis
Good in AA population –
salt sensitive. Lose K.
Beta Blockers** Atenolol, Metoprolol
MAP = CO x TPR
Decrease CO via HR
and inotropy
Can mask hypoglycemia
Alpha antagonists Doxasozin
Block a1 receptors
which vasoconstrict
Used for co-morbid BPH
Others: hydralazine, nitroprusside, methyldopa, clonidine
*Heart selective vs. vessel selective: Dihydropyridines (Amlodipine, Nifedipine) work preferentially on the vessels. (Thus, they can cause
rebound tachycardia.) Non-dihydropyridines (Verapamil, Diltiazem) work preferentially on the myocardium of the heart
**Selective vs. non-selective: e.g carvedilol (non-selective alpha and beta blockade)
LIFESTYLE MODIFICATION:
DASH Diet: Rich in fruits, vegetables, low-fat. Limit carbs. Eat whole grains.
Exercise: 40 minutes a day. Can include 3 bouts of 10 minutes walking
Smoking cessation: Reduces CVD risk associated with HTN. Consider pharmacotherapy.
Reduce salt intake: Choose “no salt added” foods, do not add salt.
Increase potassium intake: through fruits and nuts (only if renal function is normal)
Limit alcohol to 1 drink (women) or 2 drinks (men) per day
Maintain normal weight: Every 1% weight loss can decrease BP by 1mmHg.
Stress reduction / Good sleep: Consider yoga, meditation, prayer. Encourage good sleep habits.