PLACENTA
•
488 recomendaciones•257,341 vistas

DEVELOPMENT OF PLACENTA,PLACENTA AT TERM , DECIDUA,PLACENTAL MEMBRANE , PLACENTAL CICULATION,PLACENTAL ENDOCRINE SYNTHESIS,ABNORMAL PLACENTA,FUNCTIONS.

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a PLACENTA
Similar a PLACENTA (20)
Más de KHUSHBU PATEL
Más de KHUSHBU PATEL (14)
Último
Último (20)
PLACENTA
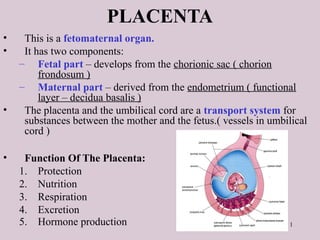
- 1. 1 PLACENTA • This is a fetomaternal organ. • It has two components: – Fetal part – develops from the chorionic sac ( chorion frondosum ) – Maternal part – derived from the endometrium ( functional layer – decidua basalis ) • The placenta and the umbilical cord are a transport system for substances between the mother and the fetus.( vessels in umbilical cord ) • Function Of The Placenta: 1. Protection 2. Nutrition 3. Respiration 4. Excretion 5. Hormone production
- 2. 2
- 3. Further Development of Chorionic Villi Early in the 3rd week, mesenchyme growth into the primary villi forming a core of mesenchymal tissue. Thus the Secondary Chorionic Villi are formed over the entire surface of the chorionic sac. Some mesenchymal cells in the secondary villi differentiate into capillaries and blood cells forming the Tertiary Chorionic Villi. The capillaries in the villi fuse to form arteriocapillary networks.
- 4. The previous formed arteriocapillary networks become connected with the embryonic heart through vessels which are formed in the mesenchyme of the chorion and connecting stalk. By the end of the 3rd week, embryonic blood begins to flow through the capillaries in the chorionic villi. Oxygen & nutrients in the maternal blood in the intervillous space diffuse through the walls of the villi and enter the embryo’s blood. Carbon dioxide & waste products diffuse from blood in the fetal capillaries through the wall of the chorionic villi into the
- 6. 6 DECIDUA • This is the endometrium of the gravid (pregnant) uterus. • It has four parts: – Decidua basalis: it forms the maternal part of the placenta – Decidua capsularis: it covers the conceptus – Decidua parietalis: the rest of the endometrium – Decidua reflexa: – Junction between capsularis & parietalis.
- 7. 7 DEVELOPMENT OF PLACENTA • Until the beginning of the 8th week, the entire chorionic sac is covered with villi. • After that, as the sac grows, only the part that is associated with Decidua basalis retain its villi. • Villi of Decidua capsularis compressed by the developing sac. • Thus, two types of chorion are formed: – Chorion frondosum (villous chorion) – Chorion laeve – bare (smooth) chorion – About 18 weeks old, it covers 15-30% of the decidua and weights about 1 6 of fetus
- 8. 8 DEVELOPMENT OF PLACENTA • The villous chorion ( increase in number, enlarge and branch ) will form the fetal part of the placenta. • The decidua basalis will form the maternal part of the placenta. • The placenta will grow rapidly. • By the end of the 4th month, the decidua basalis is almost entirely replaced by the fetal part of the placenta.
- 9. 9 FULL-TERM PLACENTA • Cotyledons –about 15 to 20 slightly bulging villous areas. Their surface is covered by shreds of decidua basalis from the uterine wall. • After birth, the placenta is always inspeced for missing cotyledons. Cotyledons remaining attached to the uterine wall after birth may cause severe bleeding. • Grooves – formerly occupied by placental septa • The fetal part of placenta; fetal membranes called developmental adnexa • Placenta;fetal membranes which are expelled are called afterbirth or secundina Maternal side
- 10. 10 FULL-TERM PLACENTA ( Discoid shape -500- 600 gm- Diameter 15-20 cm – Thickness of 2-3 cm) • Fetal surface: • This side is smooth and shiny. It is covered by amnion. • The umbilical cord is attached close to the center of the placenta. • The umbilical vessels radiate from the umbilical cord. • They branch on the fetal surface to form chorionic vessels. • They enter the chorionic villi to form arteriocapillary- venous system. Fetal side
- 11. 11 PLACENTAL CIRCULATION 80 to 100 each cotyledon - inflow
- 12. 12 STRUCTURE OF STEM CHORIONIC VILLUS
- 13. 13
- 14. 14 PLACENTAL MEMBRANE knot –syncytiotrophoblast –Toward end of pregnancy – phagocytic cells • This is a composite structure that consists of the extrafetal tissues separating the fetal blood from the maternal blood. • It has four layers: – Syncytiotrophoblast – Cytotrophoblast – Connective tissue of villus – Endothelium of fetal capillaries • After the 20th week, the cytotrophoblastic cells disappear and the placental membrane consists only of three layers.
- 15. 15 TRANSFER ACROSS THE PLACENTAL MEMBRANE Viruses: measles;poliomyelitis Microorganism: treponema pallidum of syphilis ; T.g which produce destructive change in the eye; brain . IgG( gamma globulin) , IgS;IgM ( immunoglobulin S;M )
- 16. Placental endocrine synthesis • The syncytiotrophoblast synthesizes protein &steroid hormones • The protein homones • 1- human chorionic gonadotropin • 2- h.c. somatomammotropin • 3-h.c. thyrotropin • 4-h.c. corticotropin • The steroid hormones • Progesterone & Estrogens
- 17. 17
- 18. 18
- 19. 19 Third trimester bleeding is the common sign of these anomalies
- 21. When villi persist on the entire surface of the chorionic sac ,a thin layer of placenta attaches to a large area of the uterus …… it is a membranous placenta.
- 22. 22
- 23. 23
- 24. 24
- 25. 25
- 26. 26
- 27. 27
- 29. 29
- 30. PLACENTAL FUNCTION • Transfer of nutrients and waste products bn the mother & fetus. RESPIRATORY EXCRETORY NUTRITIVE • Produces or metabolizes the hormones & enzymes necessary to maintain the pregnancy.
- 31. PLACENTAL FUNCTION • BARRIER FUNCTION • IMMUNOLOGICAL FUNCTION
- 32. Transfer function • Transport is facilitated by the close approximation of maternal and fetal vascular systems within the placenta. • It is important to recognize that there normally is no mixing of fetal and maternal blood within the placenta.
- 33. • Respiratory function—Intake of o2 & output of co2 takes place by simple diffusion.o2 supply to fetus rate of 5ml/kg/min & this achieved with cord flow of 165-330ml/min. • Excretory function—waste products urea, uric acid,creatinine are excreted to maternal blood by simple diffusion.
- 35. NUTRITIVE FUNCTION • Glucose is the major energy substrate provided to the placenta and fetus. It is transported across the placenta by facilitated diffusion via hexose transporters • Although the fetus receives large amounts of intact glucose, a large amount is oxidized within the placenta to lactate, which is used for fetal energy production.
- 36. • Amino acid concentrations in fetal blood are higher than in maternal blood. Amino acids are therefore transported to the fetus by active transport . • LIPIDS—TG`s & FA directly transported from mother to fetus in early pregnancy but synthesized in fetus later in pregnancy. Thus, fetal fat has got dual origin.
- 37. • Water & electrolytes—Na,K+,Cl- by simple diffusion.Ca,Ph,iron by active transport. • BARRIER FUNCTION:-Protective barrier to the fetus against noxious agents circulating in maternal blood. (High MW >500daltons.
- 38. IMMUNOLOGICAL FUNCTION • Fetus & placenta contain paternally determined antigens,foreign to the mother . Inspite of this ,no evidence of graft rejection. Probably: 1. Fibrinoid & sialomucin coating of trophoblast may suppress the troblastic antigen. 2. Placental hormones ,steroids, HCG have got weak immunosuppressive effect, may be responsible for producing sialomucin.
- 39. 3.Nitabuch`s layer which intervenes bn decidua basalis &cytotrophoblast probably inactivates the antigenic property of tissue. 4.There is little HLA & blood group antigens on trophoblast surface. so antigenic stimulus is poor. 5. Production of block antibodies by mother ,protects fetus from rejection.
- 40. • ENDOCRINE—hormones secreted internally. • HORMONE--Any organic chemical that is secreted by a gland into the circulatory system and is transported to some target organ. The target may be either peripheral tissue (such as muscle or other gland) or brain.
- 41. Fetal, placental & maternal compartments form an integrated hormonal unit The feto-placental-maternal (FPM) unit creates the Endocrine Environment that maintains and drives the processes of pregnancy and pre-natal development.
- 42. PLACENTAL HORMONES • Human Chorionic Gonadotropin (hCG • Human Chorionic Somammotropin (hCS) or Placental Lactogen(hPL) OTHER HORMONES • Chorionic Adrenocorticotropin • Chorionic thyrotropin • Relaxin • PTH-rP • hGH-V • Estrogen (E) • Progesterone (P) • HYPOTHALAMIC-LIKE RELEASING HORMONES • GnRH • CRH • cTRH • GH-RH • PLACENTAL PEPTIDE HORMONES • Neuropeptide-Y • Inhibin & Activin • ANP
- 43. To understand the FPM one should know: 1. The major hormones involved: hCGn Progesterone Estrogen Human Chorionic Somatomammotropin (hCS) (placental lactogen) 2. How the FPM compartments work together to produce the steroid hormones 3. The transfer of hormones between the FPM compartments.
- 45. Human Chorionic Gonadotropin (hCG) • PREGNANCY HORMONE--- glycoprotein • Half life –24hrsof hCG • Levels peak at 60-70 days then remain at a low plateau for the rest of pregnancy. • Placental GnRH have control of hCG. • FUNCTIONS: 1. RESCUE &MAINTENANCE of function of corpus luteum.
- 46. • Prevents degeneration of corpus luteum • Stimulates corpus luteum to secrete E + P which, in turn, stimulate continual growth of endometrium. 2.hCG stimulates leydig cells of male fetus to produce testosterone in conjunction with fetal pituitary gonadotrophins.Thus indirectly involed in development of external genitalia. 3. Suppresses maternal immune function & reduces possibility of fetus immunorejection
- 47. Human Chorionic Somammotropin (hCS) or Placental Lactogen • Structure similar to growth hormone • Produced by the placenta • Levels throughout pregnancy • Large amounts in maternal blood but DO NOT reach the fetus
- 48. Human Chorionic Somammotropin (hCS) or Placental Lactogen • Biological effects are reverse of those of insulin: utilization of lipids; • make glucose more readily available to fetus, and for milk production. • hCS levels proportionate to placental size • hCS levels placental insuffiency
- 49. Estrogen (E) • FORMS-estriol,estradiol &estrone . • Estriol most important . • Levels increase throughout pregnancy • 90% produced by placenta. (syncytiotrophoblast) • Placental production is transferred to both maternal and fetal compartments
- 51. • Two of the principle effects of placental estrogens are: • Stimulate growth of the myometrium and antagonize the myometrial-suppressing activity of progesterone. In many species, the high levels of estrogen in late gestation induces myometrial oxytocin receptors, thereby preparing the uterus for parturition. • Stimulate mammary gland development. Estrogens are one in a battery of hormones necessary for both ductal and alveolar growth in the mammary gland.
- 52. Progesterone (P) • Levels increase throughout pregnancy • 80-90% is produced by placenta and secreted to both fetus and mother
- 53. • Progestins, including progesterone, have two major roles during pregnancy: • Support of the endometrium to provide an environment conducive to fetal survival. If the endometrium is deprived of progestins, the pregnancy will inevitably be terminated. • Suppression of contractility in uterine smooth muscle, which, if unchecked, would clearly be a disaster. This is often called the "progesterone block" on the myometrium. Toward the end of gestation, this myometrial-quieting effect is antagonized by rising levels of estrogens, thereby facilitating parturition.
- 54. • Progesterone and other progestins also potently inhibit secretion of the pituitary gonadotropins luteinizing hormone and follicle stimulating hormone. This effect almost always prevents ovulation from occuring during pregnancy
- 57. Adrenal Gland Development • Adrenal Cortex – Vital to organism survival – Begins to develop at 4th week of embryonic life – Functional around 10th to 12th week of embryonic life – Enzymes necessary for biosynthesis of adrenocortical hormones do not develop simultaneously – hCG may have a role in stimulating Adrenocortical development • Adrenal Medulla – Originates from nervous system – Ganglia of Autonomic Nervous System
- 58. Fetal Adrenal Cortex Function – Adrenal Cortex • Zona Glomerulosa – Has enzymes to convert Pregnenalone to: » Progesterone » Deoxycorticosterone » Corticosterone » Aldosterone • Zona Fasciculata – Converts Pregnenalone and Progesterone to 17OH-Pre and 17OH-Pro – 17OH-Pro is converted to cortisol (major glucocorticoid) • Zona Reticularis – Converts 17OH-Pre into DHEA and Androstenedione (androgens)
- 59. THE END
Notas del editor
- FETAL ADRENAL GLAND