
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Pityriasis versicolor
Similar a Pityriasis versicolor (20)
Último
Último (20)
Pityriasis versicolor
- 1. PITYRIASIS VERSICOLOR Dr. KIRAN SHRESTHA (INTERN) NMCTH,BIRGUNJ
- 2. INTRODUCTION Pityriasis versicolor is a mild chronic superficial fungal infection of stratum corneum caused mainly by Malassezia species. Infection usually results from change from its lipophilic yeast form to mycelial form of Malassezia. Also called as ‘Tinea versicolor’ the term best discarded as not caused by Dermatophytes. Malassezia species are normal flora of the skin and can be cultured from both normal and affected skin. Also thought to be responsible for other dermatological condition like Seborrheic dermatitis and is not contagious.
- 3. ETIOLOGY Pityriasis versicolor is caused by dimorphic lipophilic organisms in the genus Malassezia formerly known as pityrosporum. Fourteen species are recognized in this classification of Yeast of which Malassezia globosa , Malassezia sympodalis and Malassezia furfur are predominant species isolated in P. versicolor. Malassezia is naturally found on skin surfaces of many animals including humans. It can be isolated in 18% of infants and 90-100% of adults.
- 4. PATHOGENESIS Malassezia spp. are commonly found in the stratum corneum of normal skin mostly around lipophilic zones like upper trunk neck and upper arms in its yeast form Under appropriate conditions Warm, Humid environment Hyperhidrosis(Sweating) Oral Contraceptives, Steroids Cushings Disease Immunocompromised, Malnourished state Saprophytic Yeast cell of Malassezia converted into parasitic mycelial form which causes clinical disease
- 5. Malassezia metabolizes various fatty acids likearachidonic acids or vaccenic acid via lipase and releases Azelic acids which through inhibition of Tyrosinase in Melanin production resulting in persistent hypopigmentation of affected skin for months or sometimes years. Specific compound synthesized by Malassezia called pityriacitrin that absorbs UV light and causes hyperpigmentation. Other metabolites: Malassezin : Induces apoptosis of melanocytes. Pityrialactone : an indole alkaloids that fluroscences under 300nm uv light Pityriarubin : inhibits 5-lipoxygenase enzymes
- 6. CLINICAL PRESENTATION FORM 1: Most Common Form Patient with pityriasis versicolor present with a rash consisting of well demarcated, finely scaling hypopigmented (less commonly hyperpigmented or erythematous) macules mainly starts around perifollicular region. Scale is fine , powdery and branny. M/C site of lesions are on oily regions which are also very sweaty like upper trunk often spreading to the neck and upper arms.
- 7. Lesion appears to be sitting on the skin. Lesion frequently coalesces to form patches but the distinct perifollicular character of the lesions invariably retained at periphery. Scratch sign: Lesion surmounted by branny scales which can be accenuated by scratching lesion gently with the help of glass slides also known as ‘coup d’ongle sign’ or ‘Besnier’s sign’ or ‘Stroke of the nail sign’ Itching is minimal but mild pruritus may be present.
- 8. Fig Perifollicular hypopigmented macules of P. versicolor
- 9. Fig. Lesion of Pityriasis versicolor
- 11. OTHER FORMS FORM 2 : Inverse Form Distributed typically in flexular region More commonly seen in immunocompromised FORM 3 : Folliculitis form Perifollicular erythematous papule or pustule FORM 4 : Multiple , Firm , Red-Brown inflammatory papules May or may not demonstrate scales Usually found on torso and usually asymptomatic.
- 12. DIFFERENTIAL DIAGNOSIS Hypopigmented Lesions Vitiligo Pityriasis alba Leprosy Hyperpigmnted Lesions Tinea Corporis Pityriasis rosea Guttate psoriasis Nummular Eczema Confluent and Reticulate papillomatosis Post inflammatory hyperpigmentation
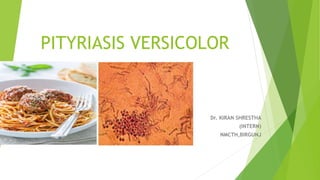
- 13. INVESTIGATIONS The Diagnosis of P. Versicolor is usually made clinically on the basis of typical lesion surmounted with scales. Culture of organism is of little value . 1. However the KOH wet mount test can be done Shows “Spaghetti and Meat ball” appearance • Spaghetti represents the fungal hyphae of Malassezia • Meat ball represents spore form
- 14. Fig. KOH wet mount preparation of P. Versicolor
- 15. 2. WOOD LAMP EXAMINATION On wood lamp examination of the lesion pityriasis versicolor gives the yellow fluroscence.
- 16. Fig Wood Lamp Examination of lesion of Pityrasis versicolor
- 17. 3. Histology Not done usually but on histopathological examination shows the superficial budding yeast (Blastoconidia) and short septate hyphae (Pseudomycelium) in stratum corneum layer of skin.
- 18. TREATMENT TOPICAL PREPARATION Selenium sulphide Zinc pyrithione Sodium sulfacetamide Azoles like Ketoconazole(2%), Allylamines like Terbinafine (1%) SYSTEMIC THERAPY Ketoconazole (200mg OD for 7-10 days or SOD of 400 mg) Fluconazole (Single oral dose of 400 mg) Itraconazole (200-400 mg OD for 3-7 days)
- 19. PREVENTION TOPICAL OR ORAL TREATMENTS ARE USED FOR PROPHYLAXIS IN CASE OF EXTENSIVE DISEASE. Topical Ketoconazole, Zinc pyrithione or Selenium sulphide shampoo applied 5-10 minutes , 1-4 times monthly Oral itraconazole 200 mg BD per month or Fluconazole or Ketoconazole
- 20. PITYRIASIS ROSEA
- 21. INTRODUCTION Pityriasis Rosea is a papulosquamous rash usually affects teen and young adults which is usually self limiting type of disease. Exact aetiology of this disorder remains to be unknown however a virus HHV-7 more frequently and HHV-6 less frequently been implicated in the pathogenesis of this disease though the disease is non contagious. Probably related to respiratory infections and slightly more common in females. Like other viral rashes most person will have this condition only once.
- 22. CLINICAL FEATURE Disease is characterized by initial appearance of Herald’s patch followed by secondary lesions. HERALD’S PATCH First lesion of Pityriasis Rosea and is seen in 80% of patients. Annular lesion with wrinkled salmon pink centre and collarette of scales at the periphery. Scales are just attached within leading edgeand free towards the centre. Primarily on trunks and upper arms.
- 24. SECONDARY ERUPTIONS Begins as a scaly papules which enlarges to form oval , annular plaques similar to Herald patch. These are smaller , less scaly and less erythematous than Herald patch. Are arranged characteristically with the long axis of patches runs downward and outward from spine along the line of Ribs with Fir tree or Christmas tree appearances.
- 25. FIG. FIR TREE DISTRIBUTION OF PITYRIASIS ROSEA
- 26. HERALD’s PATCH Phase of evolution(1-2wks) SIMILAR LESIONS, WHICH ENLARGES SLOWLY Phase of resolution (2-10 wks) MILD PIGMENTARY CHANGES FADES SLOWLY Fig. Pityriasis Rosea, Course A Self limiting Disease
- 27. HANGING CURTAIN SIGN When invidual lesions are scratched along long axis the scales tends to fold across the line of stretch.
- 28. Atypical Variants Inverse Form : Secondary eruptions are usually seen in Predominantly over axilla, groins and neck. Papular Form : When secondary eruptions is predominantly popular. Bullous Form : When secondary eruptions is predominantly vesicular.
- 29. Differential diagnosis 1. Tinea Corporis 2. Secondary Syphilis 3. Guttate Psoriasis 4. Pityriasis Licheoides Chronica(PLC) 5. Drug Eruptions Like Gold, Captopril, Barbiturates, and Penicillamines
- 30. INVESTIGATIONS Usually no investigation is required, Pityriasis Rosea is clinical diagnosis. Serology to rule out Syphilis as it can closely mimic secondary syphilis. KOH wet mount to differentiate from fungal infections.
- 31. TREATMENT Counsel patient regarding self limiting course of Disease. Symptomatic Treatment : Pruritus :Topical Calamine lotion and Antihistaminics Very Scaly/Erythematous Lesions: Coal Tar in Petroleum and Low- Medium Potency Steroids Recalcitrant Lesions : Sunlight, PUVA/PUVA SOL
- 32. PITYRIASIS ALBA
- 33. INTRODUCTION Often occurs on face, with chest being particularly common site. Etiology unknown maybe secondary to atopy and postinflammatory changes.
- 34. EPIDEMIOLOGY Exact incidence not known upto 5% of children may have Pityriasis alba. Prevalence : 5.2% in Nepal. Both gender equally affective. Age : 3-16 years of age.
- 35. CLINICAL FEATURES Rounded , Oval or Irregular plaques Red, Pink or Skin coloured Presence of Fine lamellar or Branny scaling Indistinct margins Usually 1-4 cm in diameter Generally asymptomatic but maybe mildly pruritic Site : often occurs on face , with cheek being particularly common site. Most common age group 3-16 years of age
- 36. FIG. LESION OF PITYRIASIS ALBA
- 37. FIG. LESION OF PITYRIASIS ALBA
- 38. Recurrent crops of new lesions may develop at intervals with the duration of Pityriasis alba varying from 1 month to 10 years . Most cases however resolve over a period of several months to years.
- 39. UNCOMMON VARIANT PIGMENTING VARIETY EXTENSIVE VARIETY
- 40. Differential Diagnosis Vitiligo Leprosy Psoriasis Progressive and Extensive Hypomelanosis Nevus depigmentosus Hypopigmented Mycosis Fungoides Ash leaf Macules of Tuberous Sclerosis Atopic Dermatitis Tinea versicolor Medications such as Retinoic acids, Benzyl peroxide
- 41. INVESTIGATION Investigation to rule out other causes KOH wet mounts Wood’s Lamp : Vitiligo rash will glow more brightly and have edges with sharper demarcation. SKIN BIOPSY Hyperkeratosis Parakeratosis Acanthosis Spongiosis Perivascular infiltrates
- 42. TREATMENT Reassurance Sun Protection Topical Steroids : For erythema and Pruritus. Bland Emolient creams to reduce scaling of the lesions. PUVA in extensive cases.
- 43. References DERMATOLOGY AND SEXUALLY TRANSMITTED DISEASE – DR. NEENA KHANNA DERMATOLOGY IN GENERAL MEDICINE – FITZPATRICK’s MEDSCAPE