
Recomendados
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Stanford UniversityDiabetes Health Literacy Project 030614
Similar a Stanford UniversityDiabetes Health Literacy Project 030614 (20)
Más de David Donohue
Más de David Donohue (17)
Stanford UniversityDiabetes Health Literacy Project 030614
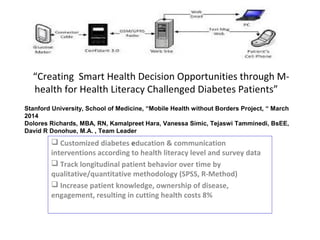
- 1. “Creating Smart Health Decision Opportunities through M- health for Health Literacy Challenged Diabetes Patients” Customized diabetes education & communication interventions according to health literacy level and survey data Track longitudinal patient behavior over time by qualitative/quantitative methodology (SPSS, R-Method) Increase patient knowledge, ownership of disease, engagement, resulting in cutting health costs 8% Stanford University, School of Medicine, “Mobile Health without Borders Project, “ March 2014 Dolores Richards, MBA, RN, Kamalpreet Hara, Vanessa Simic, Tejaswi Tamminedi, BsEE, David R Donohue, M.A. , Team Leader
- 2. Problems • Diabetes patients lack – Medical health literacy – Knowledge of their disease process – Ability to assist in their own disease management – Proactive ownership of their wellness – Dealing with fear, pain, health system confusion and lack of self management – Medication and treatment compliance
- 3. Benefits of Patient Self-Management • Increased knowledge of health condition leading to – Increase / Maintenance of Quality of Life – Savings in Cost of Health Care, Goal of 8% HC Savings – Patient Engagement, Disease Ownership • Increased MD and Clinician effectiveness – Time devoted to “health solutions” rather than emergencies
- 4. Interactive Media • Interactive tools/games (NVS Literacy and Q-Method Survey) • Data Warehouse • Data Mining • Data Analysis • Decision Support • Interactive Learning Environment • SMS, E-Mail, IVR, Web, Cell, Social Media • Tools that sell wellness to patients and care givers
- 5. Powerful Clustering Methods and Algorithms • Create interactive attitudinal profiles of patients for – Assessing patient medical literacy – Tracking patient health status over time – Monitoring patients for health status change “triggers” – Creating/choosing health interventions – Identifying user learning types – Creating custom incentive packages for patient attitudinal type, follow behavior patterns over time.
- 6. Our MHealth system isn't just another app. Rather, it engages patients via their own phones with their primary- care providers on a daily basis, sending reminders and reinforcing self-care behaviors that match a diabetic patients specific literacy level and factor group traits. Such approaches work best in systems where financial incentives are aligned and where the technology can synch with electronic health records (EHRs), neither of which is the norm as yet. Measure patient Health Literacy Level using Newest Vital Sign instrument Measure patient knowledge of their HbA1c, BP and Cholesterol condition and medical care experiences by qualitative/quantitative methologies Identify and understand patient factor-group traits (opinions feelings and attitudes) influencing health education and disease management experiences by subjective survey methods Create new M health educational interventions based on literacy level and factor group traits using SMS, E- mail, IVR, Laptop, Kiosk as communication channels Monitor HbA1c, BP and Cholesterol levels and patient self management variables by SPSS,R-Method analysis implement HIPAA data security and patient privacy protocols, encrypted technology. Database security on all provider/patient information and data PROJECT TECHNICAL APPROACH
- 7. Partners • Patient Primary and Physician Groups • Health Care Delivery Systems • Managed Care Companies (ACO’s) • Insurance, Other Health Payors • Phone/Internet/Digital Service Providers • “Premium” Partners: Federal/State govt. • Technology Companies, AT&T, Google
- 8. A Pilot SMS M-Health Research Model: Financial Costs March 2014 Even with the best health care available, patients with chronic illnesses (diabetes) typically spend no more than a few hours a year in a health care setting, while their outcomes are largely determined by their activities during the remaining 5,000 waking hours of the year. As a widely available, low-cost technology, mobile phones are a promising tool to use in engaging patients in behavior change and facilitating self-care between visits. Cost Model Estimate per 6-month Daily Cell Phone SMS diabetes Education Program Base cost per diabetic patient $575 p/p Breakout is $150.00 for technology; $225.00 for staff; $200 facility/resources COSTS OF TRADITIONAL DSME EDUCATION: Individual Diabetes Self Management Education (DSME) Initial Visit, $158.00 Per One-Hr Visit:* Individual DSME, Follow Up, $79.00 Per 30 Minutes:* Group Diabetes Management – Four Two-Hour Class Sessions,$120.00 per Two-Hr.;* Continuous Glucose Monitoring,$380.00; General Nutrition Therapy – One-on-One, Initial Visit, $117.00 Per One-Hr Visit; Nutrition Therapy – One-on-One, Follow Up, $69.00 Per 30-Minutes; Medical Nutrition Therapy, Initial, visit $132.00,Per 60 Minutes; Medical Nutrition Therapy, Follow Up, $80.00 Per 30 Minutes; Pre-Diabetes – Four One-Hour Class Sessions,$26/ Each One-Hour; Medical Nutrition Therapy Group, $30 Per 30 Minutes session; Medical Nutrition Therapy Reassess , $30 Per 15-Minutes: (source ICD codes) *First Ten Hours of Diabetes Education Per Year/PP APPROXIMATE COST $1,247.00. NOTE: 37% of U.S. Type-2 diabetes patients need to repeat the initial diabetes educational instruction series of classes.
- 9. Face to Face Interviews M.D. Gastroenterology, Clement J Zablocki VA Medical Center, Milwaukee, WI, March 2014 We would consider testing as a pilot Research Project Literacy and provider/patient communications are critical to all HC encounters and outcomes, benefiting all stakeholders Project need refinement and focus as to actual outcomes Overall a good beginning in developing solutions to a complex ongoing challenge What People are saying about “Creating Smart Health Decision Opportunities through M-health for Health Literacy Challenged Diabetes Patients.” March, 2014
- 10. Face to Face Interviews What People are saying about “Creating Smart Health Decision Opportunities through M-health for Health Literacy Challenged Diabetes Patients.” Interview conducted, Monday, March 3rd , 2014 Marketing Communications VP, March 2014 The project needs metrics (ROI) before we consider Overall has a good premise, lacking details Needs links to strong partnerships Continue developing the data and information security element; that’s the #1 priority
- 11. Face to Face Interviews What People are saying about “Creating Smart Health Decision Opportunities through M-health for Health Literacy Challenged Diabetes Patients.” Interview conducted, Froedtert Hospital, Wauwatosa WI cafeteria Sunday, March 2nd , 2014 Diabetes Clinician/RN Summary • Patients hide their literacy level • They need simple wording/layman terms •They have poor understanding of meds and treatment routines •HIPAA data and security are key to success Diabetes Patients Summary • Want simple explanations/instructions • Want information in layman terms • Want friends/relatives as support • Want additional information available • Communication is a two way street •Privacy and Information security very important
- 12. Interviews conducted New York City, NY- March 2014 Face to Face Interviews: Asked to 10 Medicare Advantage Members telephonically Questions: telephonically for face to face 10 Medicare Advantage Members: 1. Do you have a cell phone? 2. Do you use it for telephone calls only? 3. Do you text? 4. Would you like to get a daily text reminder to do your finger sticks/weigh yourself? 5. Do you get on the internet to look up information about your diabetes/heart condition/hypertension? Responses: 1. Do you have a cell phone? 10/10 said yes they have a cell phone. 2. Do you use it for telephone calls only?7/10 7 stated clearly that they only use cell to make calls. 3. Do you text? 0 none of the 10 use text. 4. Would you like to get a daily text reminder to do your finger sticks/weigh yourself?0 All 10 said they would not like text reminders. 5. Do you get on the internet to look up information about your 5/10 diabetes/heart condition/hypertension? 5/10 50% Medicare Advantage Members do use the internet to look up information pertaining to their diseases diabetes/heart condition and or hypertension. What People are saying about “Creating Smart Health Decision Opportunities through M-health for Health Literacy Challenged Diabetes Patients.”
- 13. What People are saying about “Creating Smart Health Decision Opportunities through M-health for Health Literacy Challenged Diabetes Patients.” INTERVIEW: March 2014 Retired-2013, United Healthcare Insurance Executive , Chief Medical Office, M.D. David-Here are my thoughts. Very nice 4-blocker (quad chart). Concise, easy to read. Good concept. Here are some thoughts--to take or leave: --I really like the tie in/sync with the Primary Care Provider and EHRs. So many projects leave this essential team member out. --You set a goal of 8% cost reduction. There are so many variables that can contribute to that and sometimes it takes a long period of time to demonstrate cost savings. Sometimes initial costs go up when people realize they need additional services--e.g. a comprehensive eye exam. Wonder if some shorter term measurable goals might be better--e.g. 10% drop in HgA1c within six months, 10% drop in LDL, increased activity measured through a smart phone pedometer. -- Is there a way to demonstrate interactivity and participant engagement? E.g something participants must do. Social psych studies show stronger adoption and commitment when a participant performs some action however small. Good luck with this -- sounds like an excellent opportunity!
- 14. Health Literacy: The Life Blood of Provider/Patient Communication & Understanding
- 15. Advancing Clear Health Communication to Positively Impact Health Outcomes
- 16. How Big Is the Problem? More Than 90 Million People in the US Have Difficulty Reading and Writing Approximately 40 to 48 Million Adults in the US Are Functionally Illiterate Approximately 54 Million Are Marginally Illiterate Average Reading Skills of Adults in the US Are Between the 8th and 9th Grade Levels Cannot Perform Basic Reading Tasks Required to Function in Society Have Trouble Reading Maps and Completing Standard Forms
- 17. Low Health Literacy Impacts a Patient’s Ability to Fully Engage in the Healthcare System The Largest U.S. Study Conducted to Date on Health Literacy Found That… 33% Were unable to read basic health care materials 42% Could not comprehend directions for taking medication on an empty stomach 26% Were unable to understand information on an appointment slip 43% Did not understand the rights and responsibilities section of a Medicare/Medicaid application 60% Did not understand a standard informed consent
- 18. Who Is at Health Risk for Low Health Literacy? Anyone in the US – regardless of age, race, education, income or social class – can be at risk for low health literacy – Ethnic minority groups are disproportionately affected by low health literacy – The majority of people with low literacy skills in the US are white, native-born Americans, with H.S. diploma – Older patients, recent immigrants, people with chronic diseases and those with low socioeconomic status are especially vulnerable to low health literacy – 2014, new research has pointed to 15-35 year olds as literacy challenged. PISA research study, 18% of 15 year olds are only reading at a class 2 level (solving basic reading tasks)
- 20. Solutions: Focus on Care Providers/Patient’s Educational and Communication Materials and Harness ALL Channels in One Voice Healthcare Thought Leaders: Agree that focusing on the patient-provider relationship would provide the most immediate and impactful solution to the issue of low HL 2/3 feel that low HL is driven by poor patient/doctor communication and comprehension levels Believe that providing easy-to-understand health information is key, and understanding the needs of each patient, as an individual from their viewpoint
- 21. A Picture of One American City’s Reading Culture in 2014 “The New American Global Standard?” America’s least literate city 1. Bakersfield, CA > Weekday newspaper circulation per 100: 10.1 (14th lowest) > Pct. adults with college degree: 20.5% (9th lowest) > Retail bookstores per 10,000: 0.84 (6th least) > Median income: $53,693 (12th highest) Bakersfield ,CA was in 2014 the worst city in the U.S. for its overall reading culture. The city was among the worst in the nation for access to bookstores, as well as subscriptions to magazines and scholarly journals. There were just two magazines with at least 2,500 subscriptions in the city in 2013 and no journal publications at all. There was just one independent bookstore in the city last year and just 30 retail book outlets for the city’s more than 350,000 residents. The city’s library system was also poor rated, with low circulation rates and understaffing. Low demand for reading materials could reflect low educational attainment rates — just 77% of adults had a high school diploma in 2012, among the worst nationally. The trend is a continual downward spiral.
- 22. “Creating Smart Health Decision Opportunities through M-health for Health Literacy Challenged Diabetes Patients” Creating Health Literacy in Primary Care Team, Stanford University, March 2014 Kamalprett Hara, Dolores Richards, MBA, RN, Vanessa Simic, Tejaswi Tamminedi, BsEE, David Donohue, M.A, Team Leader SYSTEM ARCHITECTURE TECHNICAL APPROACH Technology involved, cell phones, SMS, IVR, E-mail , Video, digital communications. 1. Determine patient parameters 2. Determine digital instrument protocols 3. Identify patient levels of literacy and comprehension and design customized health education messages 4. Breakdown patient population into medical literacy groups 5. Analyze patient outcome data using SPSS, R-Method for monitoring A1C, BP, and cholesterol levels, adjust communication as needed 6. Integrate results into treatment planning, address changes in patient needs over time. 7. Adaptation to wireless technology (cell, PC, smart phone etc.) 8. Set a goal of reducing patient health care costs by 8% PROJECTI OBJECTIVES AND DELIIVERABLES The goal of this project is to develop an innovative diabetes digital communication device and communicate customized educational messages using cell phones based on the patient literacy level (1) Literate (2) Literate Likely (3) Literate Unlikely. This is done by using NVS Newest Vital Sign health literacy instrument. In addition, each diabetics patient ‘s opinions, feelings and attitudes will be measured by a qualitative/quantitative instrument, (Q-Method) resulting in disease literate factor groups with similar traits. Establish new levels of understanding and communications between patient and provider Increase patient’s knowledge and ownership of the disease and treatment Increase patient safety and quality of life Every diabetes patients now classified into a factor group with individuals of similar traits (feeling, attitudes and opinions) SURVEY OBJECTIVES AND DELIVERABLES Survey methodology is an objective way of analyzing subjective patient data which allows assessment of reliability and validity Uses qualitative /quantitative methods to allow respondents to say something about their own subjective attitudes that can be tested, measured and compared Uses quantitative factor analysis (SPSS ,R-Method), data reduction and induction to generate testable hypotheses Generating customized communication interventions based on data and tested information Determine each factor groups specific medical education interventions Longitudinal , historic record of chronic disease patients progress and status trends over time. Meet HIPAA data and patient security and privacy requirements