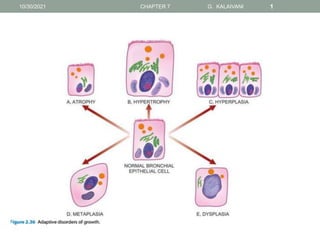
2. ATROPHY
Reduction of the number and size of parenchymal cells of an organ -
atrophy
CAUSES
physiologic or pathologic
Physiologic atrophy
lymphoid tissue with age
thymus in adult life
gonads after menopause
brain with ageing
10/30/2021 CHAPTER 7 G. KALAIVANI 2
3. ATROPHY
Pathologic atrophy
Starvation atrophy - Depletion of carbohydrate , fat stores ,protein catabolism.
emaciation (ABNORMALLY THIN)
anaemia cachexia(LOSS OF WEIGHT) seen in cancer
severely ill patients
Ischaemic atrophy - Gradual diminution (REDUCTION ) of blood supply due
to atherosclerosis
result in shrinkage of the affected organ
e.g.Small atrophic kidney - atherosclerosis of renal artery
Atrophy of the brain - cerebral atherosclerosis
Disuse atrophy - Prolonged diminished functional activity is associated with disuse
atrophy of the organ
e.g. Wasting of muscles of limb immobilised in cast
10/30/2021 CHAPTER 7 G. KALAIVANI 3
4. ATROPHY
• Neuropathic atrophy - Interruption in nerve supply leads to
wasting of muscles
• Eg. Poliomyelitis ,Motor neuron disease
• Pressure atrophy - Prolonged pressure from benign tumours
• may cause compression and atrophy of the tissues
e.g. Erosion of the spine by tumour in nerve
• Idiopathic atrophy – unknown
• e.g. Myopathies, Testicular atrophy.
10/30/2021 CHAPTER 7 G. KALAIVANI 4
5. ATROPHY
MORPHOLOGIC FEATURES
organ is small, often shrunken
cells become smaller in size
Shrinkage in cell size is due to reduction in cell
organelles, chiefly mitochondria, myofilaments and
endoplasmic reticulum.
10/30/2021 CHAPTER 7 G. KALAIVANI 5
6. HYPERTROPHY
An increase in the size of parenchymal cells resulting in
enlargement of the organ or tissue, without any change in
the number of cells
CAUSES
• physiologic or pathologic
• caused by increased functional demand or hormonal
stimulation
10/30/2021 CHAPTER 7 G. KALAIVANI 6
13. 2. Pathologic hypertrophy
Hypertrophy of cardiac muscle - cardiovascular diseases,
systemic hypertension
Aortic valve disease
Hypertrophy of smooth muscle - Cardiac achalasia (in oesophagus)
Pyloric stenosis (in stomach)
Hypertrophy of skeletal muscle - hypertrophied muscles in athletes
manual labourer
Compensatory hypertrophy - occur in an organ when the contralateral
removed
nephrectomy on one side in a young patient, there is compensatory
hypertrophy as well as hyperplasia of the nephrons of the other kidney
10/30/2021 CHAPTER 7 G. KALAIVANI 13
16. HYPERTROPHY
MORPHOLOGIC FEATURES
• affected organ is enlarged and heavy
• a hypertrophied heart of a patient with systemic hypertension
may weigh 700-800g
•
• average normal adult weight of 350 g
• enlargement of muscle fibres as well as of nuclei
• ultrastructural level, there is increased synthesis of DNA , RNA
and protein synthesis
• increased number of organelles mitochondria, endoplasmic
reticulum and myofibrils
10/30/2021 CHAPTER 7 G. KALAIVANI 16
17. HYPERPLASIA
An increase in the number of parenchymal cells resulting in
enlargement of the organ or tissue
All body cells do not possess hyperplastic growth potential
Labile cells (e.g. epithelial cells of the skin and mucous
membranes)
stable cells (e.g. parenchymal cells of the liver, pancreas,
kidney, adrenal, and thyroid)
Permanent cells (e.g. neurons, cardiac and skeletal muscle)
have little or no capacity for regenerative hyperplastic growth
10/30/2021 CHAPTER 7 G. KALAIVANI 17
18. HYPERPLASIA
• CAUSES
physiologic and pathologic
Physiologic hyperplasia
most common types - hormonal and compensatory
1.Hormonal hyperplasia - hyperplasia occurring under the
influence of hormonal stimulation
e.g.i) Hyperplasia of female breast at puberty - pregnancy
and lactation
ii) Hyperplasia - pregnant uterus.
10/30/2021 CHAPTER 7 G. KALAIVANI 18
26. HYPERPLASIA
iii) Proliferative activity of normal endometrium - normal menstrual cycle
iv) Prostatic hyperplasia - old age
2. Compensatory hyperplasia
hyperplasia occurring following removal of part of an organ or in the
contralateral organ in paired organ
e.g.
i) Regeneration of the liver - partial hepatectomy
ii) Regeneration of epidermis - after skin abrasion.
iii) Following nephrectomy on one side, there is hyperplasia of nephrons of
the other kidney.
10/30/2021 CHAPTER 7 G. KALAIVANI 26
27. HYPERPLASIA
• B. Pathologic hyperplasia - due to excessive stimulation of
hormones or growth factors
• e.g.
i) Endometrial hyperplasia - oestrogen excess
•
ii) wound healing - there is formation of granulation tissue due
to proliferation of fibroblasts and endothelial cells
•
iii) Pseudocarcinomatous hyperplasia of the skin - the margin
of a non-healing ulcer.
•
iv) Intraductal epithelial hyperplasia in fibrocystic - change in
the breast.
10/30/2021 CHAPTER 7 G. KALAIVANI 27
28. HYPERPLASIA
MORPHOLOGIC FEATURES
• enlargement of the affected organ or tissue
• increase in the number of cells
• due to increased rate of DNA synthesis and hence
increased mitoses of the cells.
10/30/2021 CHAPTER 7 G. KALAIVANI 28
29. METAPLASIA
• Reversible change of one type of epithelial or mesenchymal
adult cells to another type of adult epithelial or mesenchymal
cells
• usually in response to abnormal stimuli
• often reverts back to normal on removal Of stimulus
• stimulus persists for a long time, epithelial metaplasia may
progress to dysplasia
• further into cancer
Metaplasia is broadly divided into 2 types
• epithelial and mesenchymal
10/30/2021 CHAPTER 7 G. KALAIVANI 29
30. EPITHELIAL METAPLASIA
• change may be patchy or diffuse
• 2 types of epithelial metaplasia are
squamous and columnar
10/30/2021 CHAPTER 7 G. KALAIVANI 30
32. Squamous metaplasia
Squamous metaplasia
• Various types of specialised epithelium are capable of
undergoing
• squamous metaplastic change - due to chronic irritation
• may be mechanical, chemical or infective in origin
• Eg of squamous metaplasia are seen at following sites
i) In bronchus- chronic smokers
(normally lined by pseudostratified columnar ciliated
epithelium)
10/30/2021 CHAPTER 7 G. KALAIVANI 32
33. Squamous metaplasia
• i) uterine endocervix – prolapse(down) of the uterus
• old age
• (normally lined by simple columnar epithelium)
iii) gallbladder - in chronic cholecystitis(inflammation of the gall bladder
) & cholelithiasis(formation of gall stones)
• (normally lined by simple columnar epithelium)
iv) In prostate- chronic prostatitis & oestrogen therapy (ducts normally
lined by simple columnar epithelium)
v) In renal pelvis and urinary bladder- chronic infection and stones
(normally lined by transitional epithelium)
10/30/2021 CHAPTER 7 G. KALAIVANI 33
34. Columnar metaplasia
Columnar metaplasia
there is transformation to columnar epithelium
For eg
i) Columnar metaplasia in Barrett’s oesophagus, - change
of normal squamous epithelium to columnar epithelium
ii) chronic bronchitis and bronchiectasis - Conversion of
pseudostratified ciliated columnar epithelium to columnar
type
10/30/2021 CHAPTER 7 G. KALAIVANI 34
35. MESENCHYMAL METAPLASIA
transformation of one adult type of mesenchymal tissue to another
Eg
Osseous metaplasia - (formation of bone in fibrous tissue,
cartilage and myxoid tissue)
i) arterial wall - old age
ii) soft tissues - myositis ossificans(formation of bone tissue inside
muscle injury )
iii) cartilage of larynx and bronchi - elderly people
Cartilaginous metaplasia - In healing of fractures
occur where there is undue mobility.
10/30/2021 CHAPTER 7 G. KALAIVANI 35
37. DYSPLASIA
‘disordered cellular development’
• occurs most often in epithelial cells
• characterised by cellular proliferation and cytologic changes as
under
•
1. Increased number of layers of epithelial cells
•
2. Disorderly arrangement of cells from basal layer to the surface
layer
•
3. Loss of basal polarity i.e. nuclei lying away from basement
membrane
•
4. Cellular and nuclear pleomorphism
•
5. Increased nucleocytoplasmic ratio
•
6. Nuclear hyperchromatism
•
7. Increased mitotic activity
10/30/2021 CHAPTER 7 G. KALAIVANI 37
38. DYSPLASIA
• common examples of dysplastic changes are the uterine
cervix and respiratory tract
• often occur due to chronic irritation or prolonged
inflammation
• On removal of the inciting stimulus, the changes may
disappear
• In a proportion of cases, however, dysplasia may
progress into carcinoma in situ
(cancer confined to layers superficial to basement
membrane) or invasive cancer
10/30/2021 CHAPTER 7 G. KALAIVANI 38
40. NEOPLASIA(new growth or tumour )
• All new growth are not neoplasms
• Proliferation and maturation of cells in normal adults is
controlled as a result of which some cells proliferate
throughout life – labile cells
• Limited proliferation – stable cells
• Do not replicate – permanent cells
• Neoplastic cells lose control and regulation of replication
and form an abnormal mass of tissue
10/30/2021 CHAPTER 7 G. KALAIVANI 40
41. Some Common tumours are
• Melanoma – carcinoma of melanocytes
• Hepatoma – carcinoma of hepatocytes
• Lymphoma – malignant tumour of lymphoid tissue
• Seminoma – malignant tumour of the testis
• Leukemia – cancer of blood forming cells
10/30/2021 CHAPTER 7 G. KALAIVANI 41
42. Special categories of tumours
1.mixed tumours – adenosquamous carcinoma – mixture of
adenocarcinoma and Squamous cell carcinoma
2.teratomas – encapsulated tumour with tissue or organ eg.
Hair,teeth,bone
3.blastomas –group of malignant tumours which arise from
embryonal
such tumours occur more frequently in infants and children
under 5 years of age
.eg retinoblastoma
10/30/2021 CHAPTER 7 G. KALAIVANI 42
43. Special categories of tumours
4.Hamartoma – tumour like malformation made up of an
abnormal mixture of cells and tissues
• Considered as a developmental error
10/30/2021 CHAPTER 7 G. KALAIVANI 43
45. TUMOURSARE CLASSIFIEDAS BENIGNAND MALIGNANT,DEPENDING
ON THE BIOLOGICALBEHAVIOR OFATUMOUR
• 1.BENIGN TUMORS:
• remain localized without invasion or metastasis
• well –differentiated
• prognosis – very good
• can be cured by surgical removal in most of the patients
and the patient generally survives
10/30/2021 CHAPTER 7 G. KALAIVANI 45
46. TUMOURSARE CLASSIFIEDAS BENIGNAND MALIGNANT,DEPENDING
ON THE BIOLOGICALBEHAVIOR OFATUMOUR
• 2.MALIGNANT TUMOURS:
• cancer is the general term used for malignant tumour
• invasion – malignant tumors invade or infiltrate into the
adjacent tissues or structure
• metastasis- cancers spread to distant sites
• where the maligant cells reside,grow and again invade
• prognosis – most malignant tumours cause death
10/30/2021 CHAPTER 7 G. KALAIVANI 46
47. NOMENCLATURE OF NEOPLASMS
BENIGN TUMOUR –a tumour is said to be benign when it
gross and microscopic appearances are innocent
remain localizes
will not spread to other sites
can be surgically removed locally
the patient usually survives
generally named by attaching the suffix”oma” to the cell
origin
10/30/2021 CHAPTER 7 G. KALAIVANI 47
49. NOMENCLATURE OF NEOPLASMS
• 2.EPITHELIAL TUMOURS NOMENCLATURE IS NOT
UNIFORM BUT MORE COMPLEX
• CLASSIFIED IN DIFFERENT WAYS
A. cells of origin
B. microscopic pattern
C. macroscopic architecture
Adenoma – benign epithelial tumour arising from glandular
epithelium
May or may not form glandular structures
Eg. follicular adenoma of thyroid
10/30/2021 CHAPTER 7 G. KALAIVANI 49
50. NOMENCLATURE OF NEOPLASMS
PAPILLOMA- benign epithelial neoplasm that produces
microscopically or macroscopically visible finger like
eg. squamous papilloma
cystadenoma-tumour forming large cystic masses
eg.serous cystadenoma of ovary
10/30/2021 CHAPTER 7 G. KALAIVANI 50
52. CARCINOMA
• undifferentiated malignant tumour –
• malignant tumour composed of undifferentiated cells
• cells of origin cannot be made out on light microscopic
examination
• inappropriate terminology for malignant tumour – the term
suffix’oma’ is inappropriately used and sounds like benign
tumor
10/30/2021 CHAPTER 7 G. KALAIVANI 52
53. CARCINOMA
• malignant neoplasms arising from epithelial cell
• may be derived from any of the 3 germ layers
• nomenclature of carcinomas
10/30/2021 CHAPTER 7 G. KALAIVANI 53
GERM LAYER TISSUE/CELL MALIGNANT
TUMOUR
ECTODERM EPIDERMIS SQUAMOUS CELL
CARCINOMA
MESODERM RENAL TUBULES ADENOCARCINOMA
ENDODERM LINING OF THE GIT ADENOCARCINOMA
54. CARCINOMA
INAPPROPRIATE TERMINOLOGY
FOR MALIGNANT TUMOUR
SITE
HEPATOMA LIVER
MELANOMA SKIN
SEMINOMA/DYSGERMINOMA TESTIS/OVARY
LYMPHOMA LYMPH NODES AND EXTRANODAL
LYMPHOID TISSUE
10/30/2021 CHAPTER 7 G. KALAIVANI 54
55. SARCOMAS
• malignant tumour arising in mesenchymal tissue
• tumours have little connective tissue stroma and fleshy
• eg,fibrosarcoma, liposarcoma, osteosarcoma
• malignant tumours arising from blood forming cells are
called leukemias
10/30/2021 CHAPTER 7 G. KALAIVANI 55
56. GRADING AND STAGING OF CANCER
• ‘Grading’ and ‘staging’ are the two systems
• to predict tumour behaviour and guide therapy after a
malignant tumour is detected.
• Grading is defined as the gross appearance and
microscopic degree of differentiation of the tumour
• staging - extent of spread of the tumour within the
patient.
.
10/30/2021 CHAPTER 7 G. KALAIVANI 56
57. BRODERS GRADING ARE
THE DEGREE OF ANAPLASIA (cell with poor
differentiation)
THE RATE OF GROWTH
BASED ON THESE FEATURES,CANCERS ARE
CATEGORISED FROM
10/30/2021 CHAPTER 7 G. KALAIVANI 57
58. GRADING
• Grade I - well –differentiated (less than 25% anaplastic
cells)
• Grade II - moderately – differentiated(25-50% anaplastic
cells)
• Grade III - moderately – differentiated(50 -75% anaplastic
cells )
• Grade IV- poorly differentiated (more than 75% anaplastic
cells)
10/30/2021 CHAPTER 7 G. KALAIVANI 58
59. STAGING
• extent of spread of cancers can be assessed by 3 ways
• clinical examination
• investigations
• pathologic examination of the tissue removed
10/30/2021 CHAPTER 7 G. KALAIVANI 59
60. TNM STAGING – UNION INTERNATIONALE
CENTRE CAANCER,GENEVA
• T - PRIMARY TUMOUR
• N - REGIONAL NODAL INVOLVEMENT
• M – DISTANT METASTASES
• EACH OF 3 COMPONENTS ARE ADDED TO INDICATE
EXTENT OF INDIVIDUAL
• T0 to T 4- LARGEST AND MOST EXTENSIVE PRIMARY
TUMOUR
• N0 to N3 – NO NODAL INVOLVEMENT TO WIDESPREAD
LYMPHNODE INVOLVEMENT
• M0 to M2 – NO METASTASIS TO DISSEMINATED
HAEMATOGENOUS METASTASIS
10/30/2021 CHAPTER 7 G. KALAIVANI 60
61. AJC STAGING -AMERICAN JOINT COMMITTEE
STAGING
• DIVIDES ALL CANCERS INTO STAGE 0 to IV
• TAKES INTO ACCOUNT ALL THE 3 COMPONENTS OF
THE PRECEEDING SYSTEM
• (PRIMARY TUMOUR,NODULAR INVOLVEMENT AND
DISTANT METASTASES) IN EACH STAGE
10/30/2021 CHAPTER 7 G. KALAIVANI 61
62. • ROUTINE –RADIOGRAPHY (X-RAY,ULTRASOUND)
• -EXPLORATORY SURGERY
• MODERN TECHNIQUE - BASED ON TISSUE DENSITY
• - CT (COMPUTED TOMOGRAPHY)
• -MRI (MAGNETIC RESONANCE IMAGING
-PET(POSITRON EMISSION TOMOGRAPHY)-
DISTINCTION OF BENIGN AND MALIGNANT TUMOUR
ON THE BASIS OF BIOCHEMICAL AND MOLECULAR
PROCESSES IN TUOMOUR
RADIOACTIVE TRACER STUDIES –USE OF IODINE
ISOTOPE 125 BOUND TO SPECIFIC TUMOUR
ANTIBODIES
10/30/2021 CHAPTER 7 G. KALAIVANI 62
63. Local spread
• BENIGN TUMOURS – most benign tumours form
encapsulated or circumscribed that expand and push
aside the surrounding normal tissues without actually
invading,infiltrating or metastasis
• MALIGNANT TUMOURS- enlarge by expansion
• some well – differentiated tumours may be partially
encapsulated as well
• eg.follicular carcinoma thyroid
• invasion,infiltration and destruction of the surrounding
tissues
•
10/30/2021 CHAPTER 7 G. KALAIVANI 63
64. METASTASIS (DISTANT SPREAD)
metastasis and invasiveness are the 2 most important
features to distinguish malignant from benign tumours
ROUTE
1.Lymphatic spread
2.Haematogenous spread
3.Spread along body cavities
10/30/2021 CHAPTER 7 G. KALAIVANI 64
66. FIBROMA
• benign tumour arising in fibrous tissue is called fibroma
• true fibromas are uncommon in soft tissue
• combination of fibrous and other mesenchymal tissue is
more often seen
• these include neurofibroma,fibromyoma,dermatofibroma
and fibrolipoma
• oral cavity- fibroma more common in the oral mucosa
• reactive lesion rather than a neoplastic process
• called as irritation fibroma
10/30/2021 CHAPTER 7 G. KALAIVANI 66
67. FIBROMA
• Gross- occurs as a submucosal nodular mass primarily on
the buccal mucosa along the bite line or the gingiva
• Microcopy – shows fibrous connective tissue
stroma(consists of basement membrane, extracellular
matrix ,immune cells & vasculature)
10/30/2021 CHAPTER 7 G. KALAIVANI 67
68. FIBROSARCOMA
• slow – growing tumour
• affecting adults between 4 and 7 decades of life
• common locations are thigh,knee,trunk,head ,neck and
retroperitoneum (anatomical space in the abdominal
cavity behind the peritoneum)
• grossly – grey – white,firm,lobulated
• cut surface of the tumour is soft,fishflesh – like,with foci of
necrosis and haemorrhages
• histologically – tumour is composed of uniform ,spindle –
shaped fibroblasts
• well differentiated – herring – bone pattern
• poorly differentiated – highly pleomorphic
10/30/2021 CHAPTER 7 G. KALAIVANI 68
69. TERATOMAS
• tumours composed of different types of tissues derived
from the 3 germ cell layers
• ectoderm, mesoderm and endoderm in different
combinations
divided into 3 types
• mature (benign)
• immature (malignant)
• monodermal
10/30/2021 CHAPTER 7 G. KALAIVANI 69
70. TERATOMAS(germ cell tumour arises
from egg or sperm)
• mature (benign)- ovarian teratomas are benign and cystic
• predominat ectodermal elements – dermoid cyst
• mature teratoma may be solid and benign
• benign cystic – frequent in young women during their
active reproductive life
• tumour is bilateral in 10% of cases
10/30/2021 CHAPTER 7 G. KALAIVANI 70
71. TERATOMAS
• pathologic changes
• grossly – unilocular cyst
• 10 -15 cm in diameter, usually lined by skin
• on sectioning,the cyst is filled with paste –like sebaceous
secretions
• desquamated keratin admixed with masses of hair
• cyst wall is thin
• opaque grey –white
• generally, in one area of the cyst wall,a solid prominence
is seen (rokitansky’s protuberance)
• tissue elements such as tooth,bone,cartilage
10/30/2021 CHAPTER 7 G. KALAIVANI 71
72. TERATOMAS
• microscopically – lining of the cyst wall by stratified
squamous epithelium
• adnexal(acessory visual) structures such as sebaceous
glands,sweat glands and hair follicles
10/30/2021 CHAPTER 7 G. KALAIVANI 72
73. TERATOMA
• immature teratoma – rare
• 0.2% of all ovarian tumours
• predominatly solid tumours contain immature or
embryonal structures
• more common in prepubertal adolescents
• young women under 20 years of age
• pathological changes –
• grossly – malignant teratoma is a unilateral solid mass
• on cut section shows characterisitc
haemorrhages,necrosis
10/30/2021 CHAPTER 7 G. KALAIVANI 73
74. TERATOMAS
• microscopically – parts of the tumour may show mature
tissues
• while most of it is composed of immature tissues having
an embryonic appearance
• immature tissue elements may differentiate towards
cartilage,bone,glandular structures,neural tissues ,etc
• distributed in spindle – shaped myxoid or undifferentiated
sarcoma cells
10/30/2021 CHAPTER 7 G. KALAIVANI 74
75. TERATOMA
monodermal(specialised) teratoma- 2 important examples
struma ovarii and carcinoid tumour
struma ovarii – teratoma composed exclusively of thyroid
tissue
tumour has the appearance of a follicular adenoma of the
thyroid
rarely,struma ovarii may be hyperfunctioing and produce
hyperthyroidism
carcinoid tumour – ovarian teratoma arising from
argentaffin cells of intestinal epithelium in the teratoma
10/30/2021 CHAPTER 7 G. KALAIVANI 75
76. LIPOMA
• commonest benign tumour of fat
• most common soft tissue tumour of adulthood
• most often during 4 to 5 decades of life
• frequent in females
• lipoma is usually single,soft,mobile painless mass
• site – usually arises in the subcutaneous tissues of the
proximal extremities neck,back,shoulder and trunk
• lipoma rarely ever transforms into liposarcoma
10/30/2021 CHAPTER 7 G. KALAIVANI 76
77. LIPOMA
grossly – subcutaneous lipoma is usually small,round to
oval and encapsulated mass
• cut surface is soft,loblated,yellow – orange and greasy
histologically – tumour is composed of lobules of mature
adipose cells separated by delicate fibrous septa
a thin fibrous capsule surrounds the tumour
10/30/2021 CHAPTER 7 G. KALAIVANI 77
78. LIPOMA
• a variety of admixture of lipoma with other tissue
component may be seen
• include fibrolipoma – admixture with fibrolipoma
• angiolipoma – combination with proliferating blood
vessels
• myelolipoma – admisture with bone marrow elements as
seen in adrenals
10/30/2021 CHAPTER 7 G. KALAIVANI 78
79. LIPOSARCOMA
• one of the common soft tissue sarcomas
• lipoma which originates from mature adipose cells
• liposarcoma arises from primitive mesenchymal cells,the
lipoblasts
• peak incidence is in 5 to 6 decades of life
• lipomas are more frequently subcutaneous in locations
• liposarcomas often occur in the deep tissues
• most frequent site are intermuscular regions –
thigh,buttocks and retroperitoneum
10/30/2021 CHAPTER 7 G. KALAIVANI 79
80. LIPOSARCOMA
• grossly – appears as a nodular mass
• 5cm or more in diameter
• cut surface is grey white to yellow,myxoid and gelatious
• retroperitoneal masses are generally much larger
• histologically – hallmarks of diagnosis of liposarcoma is
the identification of variable number of lipoblasts
• may be multivacuolated or univacuolated
10/30/2021 CHAPTER 7 G. KALAIVANI 80
81. LIPOSARCOMA
• vacuoles represent fat in the cytoplasm
• 4 major histologic varieties of liposarcomas are
• 1.well – differentiated liposarcoma- resembles lipoma
• contains uni or multivacuolated lipoblasts
• 2.myxoid liposarcoma – composed of
monomorphic,fusiform or stellate cells representing
primitive mesenchymal cells
• lying dispersed in mucopolysaccharide – rich ground
substance
10/30/2021 CHAPTER 7 G. KALAIVANI 81
82. LIPOSARCOMA
• occasional tumour giant cells may be present
3.round cell liposarcoma – composed of uniform,round to oval
cells having fine multivacuolated cytoplasm with central
hyperchromatic nuclei
round cell liposarcoma may resemble a signet – ring
carcinoma
4.pleomorphic liposarcoma – highly undifferentiated
most anaplastic type
numerous large tumour giant cells
10/30/2021 CHAPTER 7 G. KALAIVANI 82
83. NEUROFIBROMA
• occurs as solitary,fusiform cutaneous tumour of a single
nerve
• adult
• hereditary disorder with autosomal dominant inheritance
• asymptomatic
• type 1 – mutation in chromosome 17
• type 2 – mutation in chromosome 22
10/30/2021 CHAPTER 7 G. KALAIVANI 83
84. NEUROFIBROMA
MORPHOLOGICAL FEATURES
• unencapsulated tumour producing fusiform enlargement
of the affected nerve
• involved in group of nerves or multiple
• oval and irregular swellings along the length of a nerve
MICROSCOPICALLY
composed of bundles
interlacing fascicles of delicate
elongated spindle shaped cells having wavy nuclei
cellular area is separated by loose collagen & mucoid
material
ihc – positive foe epithelial membrane antigen
10/30/2021 CHAPTER 7 G. KALAIVANI 84
85. MALIGNANT MELANOMA or
MELANOCARCINOMA
• Arising from melanocytes
• Most rapidly spreading malignant tumour of the skin that
can occur at all ages
• But rare before puberty
• Tumour spreads locally as well as to distant sites by
lymphatics and blood
• Etiology is unknown
• Role of excessive exposure of white skin to sunlight
• Eg high incidence in new zealand and australia where sun
exposure in high
10/30/2021 CHAPTER 7 G. KALAIVANI 85
86. MALIGNANT MELANOMA or
MELANOCARCINOMA
• common sites on the skin are the
trunk(men),legs(women),faces,palms and nail – beds
• depending upon the clinical course and
prognosis,cutaneous malignant melanomas are of the
following 4 types:
• 1.lentigo maligna melanoma
• often develops from a pre-existing lentigo
• essentially a malignant melanoma
• slow growing
• good prognosis
10/30/2021 CHAPTER 7 G. KALAIVANI 86
87. MALIGNANT MELANOMA or
MELANOCARCINOMA
• 2.superficial spreading melanoma- slightly elevated lesion
with variegated colour
• ulcerated surface
• often develops from a superifical spreading surface
• often develops from a superficial spreading melanoma
• prognosis is worse than for lentigo maligna melanoma
10/30/2021 CHAPTER 7 G. KALAIVANI 87
88. MALIGNANT MELANOMA or
MELANOCARCINOMA
• 3.acral lentigenous melanoma –
• occurs more commonly on the soles,palms and mucosal
surfaces
• tumour often undergoes ulceration
• early metastases
• prognosis is worse than that of superficial spreading
melanoma
10/30/2021 CHAPTER 7 G. KALAIVANI 88
89. MALIGNANT MELANOMA or
MELANOCARCINOMA
• 4.nodular melanoma
• often appears as an elevated and deeply pigmented
nodule that grows rapidly
• undergoes ulceration
• this variant carries the worst prognosis
10/30/2021 CHAPTER 7 G. KALAIVANI 89
90. MALIGNANT MELANOMA or
MELANOCARCINOMA
• HISTOLOGICALLY –
• 1.ORIGIN – MALIGNANT MELANOMA,WHETHER
ARISING FROM A PRE-EXISTING NAEVUS OR
STARING DE NOVO,HAS MARKED JUNCTIONAL
ACTIVITY AT THE EPIDERMO DERMAL JUNCTION
AND GROWS DOWNWARD INTO THE DERMIS
• 2.TUMOUR CELLS-MALIGNANT MELANOMA CELLS
ARE USUALLY LARGER THAN THE NAEVUS CELLS
• MAY BE EPITHELIOID OR SPINDLE – SHAPED
• THE FORMER BEING MORE COMMON
• TUMOUR CELLS HAVE AMPHOPHILIC CYTOPLASM
• LARGE,PLEOMORPHIC NUCLEI WITH
CONSIPICUOUS NUCLEOLI
10/30/2021 CHAPTER 7 G. KALAIVANI 90
91. MALIGNANT MELANOMA or
MELANOCARCINOMA
• 3.MELANIN
• MELANIN PIGMENT MAY BE PRESENT OR ABSENT
WITHOUT ANY PROGNOSTIC INFLUENCE
• THE PIGMENT,IF PRESENT,TENDS TO BE IN FORM
OF UNIFORM FINE GRANULES
• THERE MAY BE NO EVIDENCE OF MELANIN IN H & E
STAINED SECTIONS
• FONTANA – MASSON STAIN or DOPA REACTION
REVEALS MELANIN GRANULES IN THE CYTOPLASM
OF TUMOUR CELLS
10/30/2021 CHAPTER 7 G. KALAIVANI 91
92. MALIGNANT MELANOMA or
MELANOCARCINOMA
• 4.INFLAMMATORY INFILTRATE – SOME AMOUNT OF
INFLAMMATORY INFILTRATE IS PRESENT IN THE
INVASIVE MELANOMAS
• INFREQUENTLY,PARTIAL SPONTANEOUS
REGRESSION OF THE TUMOUR OCCURS DUE TO
DESTRUCTIVE EFFECT OF DENSE INFLAMMATORY
INFILTRATE
10/30/2021 CHAPTER 7 G. KALAIVANI 92
93. MALIGNANT MELANOMA or
MELANOCARCINOMA
• PROGNOSIS FOR PATIENTS WITH MALIGNANT
MELANOMA
• LEVEL I MALIGNANT MELANOMA CELLS CONFINED
TO THE EPIDERMIS AND ITS APPENDAGES
• LEVEL II EXTENSION INTO THE PAPILLARY DERMIS
• LEVEL III EXTENSION OF TUMOUR CELLS UPTO THE
INTERFACE BETWEEN PAPILLARY AND RETICULAR
DERMIS
• LEVEL IV INVASION OF RETICULAR DERMIS
• LEVEL V INVASION OF THE SUBCUTANEOUS FAT
10/30/2021 CHAPTER 7 G. KALAIVANI 93
94. MALIGNANT MELANOMA or
MELANOCARCINOMA
• METASTATIC SPREAD OF MALIGNANT MELANOMA IS
VERY COMMON
• TAKES PLACE LYMPH NODES
10/30/2021 CHAPTER 7 G. KALAIVANI 94
95. Carcinogenesis
• DEFINITION – A CARCINOGEN IS AN AGENT KNOWN
OR SUSPECTED TO CAUSE TUMOURS
• SUCH AGENTS ARE SAIS TO BE CARCINOGENIC
• CHEMICAL CARCINOGENIC AGENTS
• 1.CHEMICAL
• 2.MICROBIAL AGENTS
• 3.RADIATION
10/30/2021 CHAPTER 7 G. KALAIVANI 95
97. CLASSIFICATION OF CHEMICAL
Carcinogenesis
• A.DIRECT – ACTING AGENTS
• DO NOT REQUIRE MEABOLIC CONVERSION TO BECOME
CARCINOGENIC
• ALKYLATING AGENTS
• SOURCE – MANY CANCER CHEMOTHERAPEUTIC DRUGS
• Eg.cyclophosphamide, cisplatin,busulfan
• Mechanism of action – react with electron rich atoms in
DNA
• Drugs not only destroy cancer cells by damaging DNA,but
also injure normal cells
• Cancer produced – solid and hematological malignancie
10/30/2021 CHAPTER 7 G. KALAIVANI 97
98. CLASSIFICATION OF CHEMICAL
Carcinogenesis
• B.INDIRECT – ACTING AGENTS
• CHEMICALS REQUIRE METABOLC ACTIVATION FOR
CONVERSION TO AN ACTIVE ULTIMATE
CARCINOGEN
• Eg. benzol(a)Pyrene
• Source
• Originaly derived from coal tar and fossil fuels
• Cigarette smoke –RESPONSIBLE FOR LUNG CANCER
• Animal fats – PROCESS OF BROILING MEATS
• Smoked food- SMOKED MEATS AND FISH
10/30/2021 CHAPTER 7 G. KALAIVANI 98
99. CLASSIFICATION OF CHEMICAL
Carcinogenesis
• mechanism of action-metabolized by cytochrome p450 –
dependent mixed function oxidases to electophilic
epoxides
• epioxides react with proteins and nucleic acids(dna,rna)
• eg.polyvinyl chlorides(used in plastic industry) is
metabolized to an epoxide and causes hepatic
angiosarcomas
• cancer produced – skin,soft tissues,lung and breast
10/30/2021 CHAPTER 7 G. KALAIVANI 99
100. CLASSIFICATION OF CHEMICAL
Carcinogenesis
• 2.natural microbial product
• aflatoxin b1
• natural product of aspergillus flavus
• a mold which which grows on improperly stored grains
and peanuts
• mechanism of action – metabolized to an epioxide
• bind to dna
• also produces mutation of p53 gene
• cancer produced – hepatocellular carcinoma
10/30/2021 CHAPTER 7 G. KALAIVANI 100
101. CLASSIFICATION OF CHEMICAL
Carcinogenesis
OTHERS
• nitrosamines-potent carcinogenes
• source – before the advent of refrigerator,nitrites were
added as preservative for meals and other foods
• mechanism of action – nitrites react with amines and
amides in the diet
• metabolized by bacteria within the gut
• converted to carcinogenic nitrosamines
• cancer produced – gastrointestinal neoplasm
10/30/2021 CHAPTER 7 G. KALAIVANI 101
102. CLASSIFICATION OF CHEMICAL
Carcinogenesis
• metals – compunds like
arsenic,nickel,lead,cadmium,cobalt,chromium and
beryllium can produce cancer
• most metal induced cancers occur due to occupational
exposure
10/30/2021 CHAPTER 7 G. KALAIVANI 102
103. MECHANISM OF ACTION OF
CHEMICAL Carcinogenesis
• chemical carcinogens are mutagenic
• permanently alter the genetic constitution of a cell
• genes – proto- oncogenes (ras)
• tumour suppressor genes(p53)
10/30/2021 CHAPTER 7 G. KALAIVANI 103
104. MULTISTEP HYPOTHESIS
• 4 steps
• 1.initiation –first satge in carcinogenesis induced by
initiator chemical carcinogens
• change can be produced by a single dose of the initiating
agent for a short time
• large dose for longer duration is more effective
• change so induced is sudden,irreversible and permanent
• chemical carcinogens acting as initiators of carcinogens
10/30/2021 CHAPTER 7 G. KALAIVANI 104
105. INITIATION
• 1.direct – acting carcinogens
• few chemical substances(eg.alkylating agents,acylating
agents) which can induce cellular tranformation without
undergoing any priormetabolic activation
• 2.indirect – acting carcinogens or procarcinogens
• metabolic activation – chemical carcinogens are indirect
–acting or procarcinogens require metabolic activation
direct acting carcinogens donot require the metabolic
activation
10/30/2021 CHAPTER 7 G. KALAIVANI 105
106. INITIATION
• most carcinogens are activated chiefly by the mixed
oxidases of the cytochrome p-450 system located in the
microsomal component of the endoplasmic reticulum or
in the nucleus
10/30/2021 CHAPTER 7 G. KALAIVANI 106
107. REACTIVE ELECTOPHILES
• electron deficient which bind to electron rich portions of
others molecules of the cells such as dna,rna & other
protein
• target molecules – target of electrophiles in
dna,producing mutagenesis
• change in dna may lead to the initiated cells or some form
of cellular enzymes may be able to repair the damage in
dna
• initiated cells-unrepaired damage produced in the dna of
the cell becomes permanent only if the altered cell
undergoes atleast 1 cycle of proliferaton
10/30/2021 CHAPTER 7 G. KALAIVANI 107
108. INITIATED CELLS
• Results in transferring the change to the next progency of
the cell .so that dna damage becomes permanent &
irreversible
10/30/2021 CHAPTER 7 G. KALAIVANI 108
109. PROMOTION OF CARCINOGENESIS
• substances such as phorbol
esters,phenols,hormones,artifical sweeters & drugs like
phenobarbital
• donot produce sudden change
• they require application or administration as the case may
be,for sufficient time and in sufficient dose
• change induced may be reversible enhance the effect of
carcinogenesis
• activation of growth factor
10/30/2021 CHAPTER 7 G. KALAIVANI 109
111. VIRAL CARCINOGENESIS
• common viral infections can be transmitted by one of the 3
routes:
i) Horizontal transmission - by direct contact, by ingestion of
contaminated water or food, or by inhalation as occurs in most
contagious diseases
• infections begin on the epithelial surfaces, spread into deeper
tissues
• then through haematogenous or lymphatic or neural route
disseminate to other sites in the body.
ii) parenteral route - by inoculation as happens in
some viruses by inter-human spread and from animals and
insects to humans.
iii) Vertical transmission - infection is genetically
transmitted from infected parents to offsprings.
10/30/2021 CHAPTER 7 G. KALAIVANI 111
112. VIRAL CARCINOGENESIS
• Based on their nucleic acid content, oncogenic viruses fall
into 2 broad groups:
1.deoxyribonucleic acid are called DNA
oncogenic viruses.
2. ribonucleic acid are termed RNA
oncogenic viruses or retroviruses
10/30/2021 CHAPTER 7 G. KALAIVANI 112
113. VIRAL CARCINOGENESIS
• Both types of oncogenic viruses usually have 3 genes and are
abbreviated according to the coding pattern by each gene:
i) gag gene: codes for group antigen.
ii) pol gene: codes for polymerase enzyme.
iii) env gene: codes for envelope protein.
•
”Primary viral infections -
the infection lasts for a few days to a few weeks
generally cleared by body’s innate immunity and specific immune
responses
An immunocompetent host is generally immune to the disease
”
Persistence of viral infection or latent infection -
viruses may occur by acquiring mutations in viruses which
resist immune attack by the host, or virus
Induces immunosuppression in the host such as HIV
10/30/2021 CHAPTER 7 G. KALAIVANI 113
114. : • General mode of oncogenesis by each group of DNA and
RNA oncogenic viruses is briefly considered below:
10/30/2021 CHAPTER 7 G. KALAIVANI 114
118. PATHOLOGIC DIAGNOSIS OF CANCER / LAB DIAGNOSIS OF
CANCER
1.HISTOLOGIC METHODS
• Most valuable in arriving at the accurate diagnosis
• Based on microscopic examination of excised tumour mass, needle biopsy
• Tissue must be fixed in 10% formalin –light microscopy
• Glutaraldehyde – electron microscopy
• Quick –frozen section & hormonal analysis – fresh unfixed tissue
i)PARAFFIN –EMBEDDING TECHNIQUES
• 10% formalin fixed tissue
• tissue piece from larger tumour mass or biopsy is processed overnight
cycle
• tissue processing, rotary microtome
• stained with haematoxylin and eosin (H & E) and examined
microscopically.
10/30/2021 CHAPTER 7 G. KALAIVANI 118
119. PATHOLOGIC DIAGNOSIS OF
CANCER
ii) FROZEN SECTION
unfixed tissue is used
patient is undergoing surgery and is still under
anaesthesia
cryostat machine(-25°C )and fresh unfixed tissue
Rapid H & E or toluidine blue staining
10/30/2021 CHAPTER 7 G. KALAIVANI 119
120. 2. CYTOLOGICAL METHODS
i) Exfoliative cytology
Pap smear
carcinoma in situ and invasive carcinoma of the uterine cervix.
examination of sputum, bronchial washings,
pleural, peritoneal and pericardial effusions & CSF
ii) Fine needle aspiration cytology (FNAC)
Superficial masses are aspirated from the pelvic organ
investigated by ultrasound and computed tomography
Wet fixed smear – Pap staining
Air dried smear -May-Grünwald-Giemsa or Leishman stain.
10/30/2021 CHAPTER 7 G. KALAIVANI 120
124. 10/30/2021 CHAPTER 7 G. KALAIVANI 124
• ii) Prognostic markers in cancer
• The second important application of IHC
• predict the prognosis of tumours
• Examples, proto-oncogenes tumour suppressor genes or
antioncogenes - Rb gene, p53
iii) Prediction of respone to therapy
• to predict therapeutic response in two important tumours—
carcinoma of the breast and prostate.
• Both these tumours are under the growth regulation of
hormones—oestrogen and androgen
•
iv) Infections
• To confirm infectious agent in tissues by use of specific
antibodies against microbial DNA or RNA
• e.g. detection of viruses (HBV, CMV, HPV, herpesviruses),
bacteria (e.g. Helicobacter pylori) &
parasites (Pneumocystis carinii) e
125. 5. ELECTRON MICROSCOPY
General features of malignant tumour cells by examination can be
appreciated
i) Cell junctions, their presence and type
ii) Cell surface, e.g. presence of microvilli
iii) Cell shape and cytoplasmic extensions
iv) Shape of the nucleus and features of nuclear membrane.
v) Nucleoli, their size and density
vi) Cytoplasmic organelles—their number is generally
reduced
vii) Dense bodies in the cytoplasm.
10/30/2021 CHAPTER 7 G. KALAIVANI 125
126. • .
6. TUMOUR MARKERS (BIOCHEMICAL ASSAYS)
Tumour markers include: cell surface, cytoplasmic
proteins, enzymes, hormones and cancer antigens
• examples of oncofoetal antigens secreted
by foetal tissues as well as by tumours are
i) Alpha-foetoprotein (AFP).
ii) Carcino-embryonic antigen (CEA)
10/30/2021 CHAPTER 7 G. KALAIVANI 126
128. 7.Other modern aids in pathologic diagnosis of tumours
i) Flow cytometry
ii) In situ hybridisation
modern fluorescence in situ hybridisation (FISH)
iii) Cell proliferation analysis
a) Radioautography
b) Microspectrophotometric analysis.
c) IHC proliferation markers.
d) Nucleolar organiser region (NOR)
iv) Image analyzer and morphometry
a) Morphometric study.
b) Quantitative nuclear DNA ploidy measurement.
c) Quantitative valuation of immunohistochemical staining.
v) Molecular diagnostic techniques
a) Analysis of molecular cytogenetic abnormalities
b) Mutational analysis
c) Antigen receptor gene rearrangement
d) Study of oncogenic viruses at molecular level.
.
vi) DNA microarray analysis of tumours
10/30/2021 CHAPTER 7 G. KALAIVANI 128