Russian Call Girls in Noida Pallavi 9711199171 High Class Call Girl Near Me
URINARY SYSTEM DRUGS.docx
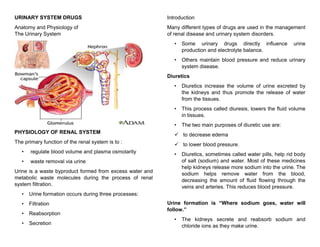
1. URINARY SYSTEM DRUGS
Anatomy and Physiology of
The Urinary System
PHYSIOLOGY OF RENAL SYSTEM
The primary function of the renal system is to :
• regulate blood volume and plasma osmolarity
• waste removal via urine
Urine is a waste byproduct formed from excess water and
metabolic waste molecules during the process of renal
system filtration.
• Urine formation occurs during three processes:
• Filtration
• Reabsorption
• Secretion
Introduction
Many different types of drugs are used in the management
of renal disease and urinary system disorders.
• Some urinary drugs directly influence urine
production and electrolyte balance.
• Others maintain blood pressure and reduce urinary
system disease.
Diuretics
• Diuretics increase the volume of urine excreted by
the kidneys and thus promote the release of water
from the tissues.
• This process called diuresis, lowers the fluid volume
in tissues.
• The two main purposes of diuretic use are:
to decrease edema
to lower blood pressure.
• Diuretics, sometimes called water pills, help rid body
of salt (sodium) and water. Most of these medicines
help kidneys release more sodium into the urine. The
sodium helps remove water from the blood,
decreasing the amount of fluid flowing through the
veins and arteries. This reduces blood pressure.
Urine formation is “Where sodium goes, water will
follow.”
• The kidneys secrete and reabsorb sodium and
chloride ions as they make urine.
2. • Diuretics block the reabsorption of these ions, so the
sodium has nowhere to go but out of the kidneys and
into the urinary bladder.
• Water then follows the sodium out of the kidneys and
into the urinary bladder, and diuresis occurs.
The Classes of Diuretics
• Thiazides
• Loop agent
• Potassium-sparing diuretics,
• Carbonic anhydrase inhibitors
• Osmotics agent
• Aldosterone antagonist
• ADH antagonist
Thiazides
• Thiazides are diuretics that act directly on the distal
convoluted tubules to block sodium reabsorption and
promote chloride ion excretion.
• Thiazides most often manage edema associated
with congestive heart failure.
• Oral administration of thiazides produces diuresis in
all patients , with few documented side effects.
This effect remains even with prolonged use, but long-term
thiazide use does cause:
• excessive potassium secretion
• leading to hypokalemia (potassium deficiency)
• cardiac dysfunction.
To prevent hypokalemia suggest that potassium-rich diets
or
• potassium supplements accompany thiazide
diuretics.
3. Loop diuretics
• The loop of Henle, a U-shaped renal tubule, is the
sodium-reabsorbing site that lends its name to this
type of diuretic.
• Loop diuretics influence the reabsorption action at
the loop of Henle.
Furosemide (Lasix, Disal, Diuride) and ethacrynic acid
(Edecrin), two loop diuretics, are potent and effective drugs
that block absorption of the following ions:
• chloride, potassium, calcium, hydrogen, magnesium,
and bicarbonate.
The result of blocking reabsorption of all of these
electrolytes is tremendous diuresis.
The main side effects
• Electrolyte imbalances, especially hypokalemia,
which can lead to cardiac arrhythmias.
• Parenteral administration produces diuresis
immediately on a fully functional kidney.
Potassium-Sparing Diuretics
Drugs in this group are used as mild diuretics or in
combination with other drugs.
• Potassium-sparing diuretics are weaker diuretics
than thiazides or loop
• diuretics.
• Potassium-sparing diuretics act on the distal
convoluted tubules to promote sodium and water
excretion and potassium retention.
Mechanism of action :
• Interfering the sodium-potassium pump that is
controlled by aldosterone (a mineralocorticoid
produced by the adrenal cortex that affects sodium
and potassium levels).
• Potassium is reabsorbed, and sodium is excreted.
DRUGS
In this category include spironolactone (Aldactone),
• triamterene (Dyazide), and amiloride (Midamor).
The main side effect of these drugs is hyperkalemia.
Carbonic Anhydrase Inhibitors
• Carbonic anhydrase inhibitors, such as
acetazolamide (Diamox) and dichlorphenamide
(Daranide),
Mechanism of action : block the action of the enzyme
“carbonic anhydrase.”
This enzyme is used by the body to maintain acid-
base balance (mainly between hydrogen and
bicarbonate ions).
Inhibition of this enzyme causes increased sodium,
potassium, and bicarbonate excretion.
The main side effect
With prolonged use of carbonic anhydrase inhibitors can
develop metabolic acidosis.
Indication : mainly used to decrease intraocular pressure
with open-angle glaucoma
4. Osmotic Diuretics
• Mechanism of action : Osmotic diuretics increase the
osmolality (concentration) of the filtrate in the renal
tubules.
This results in excretion of sodium, chloride, potassium,
and water.
Indication : use to prevent kidney failure, to decrease
intracranial pressure, and to decrease intraocular
pressure (i.e., glaucoma). Mannitol (Osmitrol and
generic) and glycerin (Osmoglyn) are examples of
osmotic diuretics.
• Side effects are uncommon with osmotic diuretics,
but can include fluid and electrolyte imbalance and
vomiting.
Nursing responsibilities
• Administer drug with food or milk if GI upset is a
problem to buffer drug effect on the stomach lining.
• Administer intravenous diuretics slowly to prevent
severe changes in fluid and electrolytes.
• Administer oral form early in the day to prevent
increased urination during sleep hours.
• Monitor patient response to drugs through vital signs,
weight, serum electrolytes and hydration to evaluate
effectiveness of drug therapy.
• Assess skin condition to determine presence of fluid
volume deficit or retention.
• Provide comfort measures (e.g. skin care, nutrition
referral, etc.) to help patient tolerate drug effects.
• Provide safety measures (e.g. adequate lighting,
raised side rails, etc.) to prevent injuries.
• Educate client on drug therapy to promote
compliance.
BLOOD PRESSURE LOWERING
Drugs used to decrease hypertension, called
antihypertensives
The primary factor in hypertension is increased
resistance to blood flow, resulting from the narrowing
of peripheral blood vessels.
If left untreated, elevated blood pressure are at risk
for developing cardiac and renal dysfunction.
Some drugs that affect blood pressure
include the following :
• Diuretics
• Angiotensin-Converting Enzyme Inhibitors (ACE
Inhibitors)
• Calcium Channel Blockers
• Direct-Acting Arteriole Vasodilators
• Beta-Adrenergic Antagonists
• Alpha-Adrenergic Antagonists
5. Diuretics
• Diuretics have an antihypertensive effect by
promoting sodium and water loss, which causes a
decrease in fluid volume and blood pressure.
Angiotensin-Converting Enzyme Inhibitors
(ACE Inhibitors)
The kidneys regulate blood pressure via the renin-
angiotensin system.
Renin, an enzyme released by the kidneys,
stimulates the conversion of angiotensin I to
angiotensin II (a potent vasoconstrictor).
Angiotensin II causes the release of aldosterone (a
mineralocorticoid from the adrenal cortex that
promotes retention of sodium and water).
Retention of sodium and water increases fluid
volume, which elevates blood pressure.
Mechanism of Action
• ACE inhibitors block the conversion of angiotensin I
to angiotensin II, which decreases aldosterone.
Clinically, ACE inhibitors are used to treat
hypertension.
DRUGS : enalapril (Enacard, Vasitec), captopril (Capoten),
lisinopril (Zestril), and benazepril (Lotensin)
Calcium Channel Blockers
Mechanism of Action : Calcium channel blockers block the
influx of calcium ions into the myocardial cells
Resulting in an inhibition of cardiac and vascular
smooth muscle contractility.
This decreased resistance to blood flow reduces
blood pressure, thus affecting glomerular filtration.
Side effects include hypotension and edema.
Examples include diltiazem (Cardizem), verapamil
(Isoptin), and nifedipine Procardia)
Direct-Acting Arteriole Vasodilators
Mechanism of Action : Direct-acting arteriole
vasodilators relax smooth muscles of the blood
vessels, mainly arteries, causing vasodilation.
6. The main side effect of this drug group is edema due
to sodium and water retention.
Examples include hydralazine (Apresoline) and
minoxidil (Loniten).
Beta-Adrenergic Antagonists
Beta-adrenergic antagonists, also known as beta
blockers, can affect the heart and bronchi.
Beta-1 blockers work on the heart
Beta-2 blockers work on the bronchial receptors.
Mechanism of Action : Nonselective beta blockers
will inhibit the activity of beta-1 and beta-2 receptors,
resulting in bradycardia and bronchoconstriction.
Side effects include decreased blood pressure,
decreased cardiac output, and bronchospasm.
An example of a nonselective beta blocker is
propranolol (Inderal®).
Nursing responsibilities
• Educate patient on importance of healthy lifestyle
choices which include regular exercise, weight loss,
smoking cessation, and low-sodium diet to maximize
the effect of antihypertensive therapy.
• Monitor blood pressure and heart rate and rhythm
closely to evaluate for effectiveness and ensure
quick response if blood pressure falls rapidly or too
much.
• Provide comfort measures for the patient to tolerate
side effects (e.g. small frequent meals for nausea,
limiting noise and controlling room light and
temperature to prevent aggravation of stress which
can increase demand to the heart, etc.)
• Monitor patient for any manifestations that could
decrease fluid volume inside the body (e.g. vomiting,
diarrhea, excessive sweating, etc.) to detect and
treat excessive hypotension.
• Educate patient and family members about drug’s
effect to the body and manifestations that would
need reporting to enhance patient knowledge on
drug therapy and promote adherence.
• Emphasize to the client the importance of strict
adherence to drug therapy to ensure maximum
therapeutic effects.
Urolithiasis
• Urolithiasis—the formation of stones (calculi) in the
kidney, bladder, and/or urethra—is increasingly
common, with a rate of approximately 12%
worldwide, and it is associated with an enhanced risk
of end-stage renal disease. The most common form
of kidney stone is calcium oxalate (CaOx) on the
renal papillary surface.
UROLITH TREATMENT
Uroliths (also known as urinary calculi) are abnormal
mineral masses in the urinary system.
Uroliths are composed of a large amount of
crystalline material (organic and inorganic
crystalloids) and a small amount of organic matrix
(typically mucoid material).
7. Overview
The development of urolith formation is not fully
understood, but dietary factors are known to be
important in some cases.
Uroliths in the urinary bladder cause hematuria
(blood in the urine) and dysuria.
Uroliths that lodge in the urethra may cause
obstruction, which is a major concern because of the
narrow diameter of the urethra.
Treatment
Antibiotic therapy (if warranted)
Medical dissolution of the uroliths
Surgical removal of the uroliths.
Medical dissolution of uroliths
• Dissolution therapy aims to dissolve stones through
administration of oral agents to by direct chemolysis
through renal irrigation.
Uroliths that form in alkaline (basic) urine (struvite
uroliths)
Place in urine-acidifying diet that dissolves uroliths
Prescribed urinary acidifiers such as methionine
(Methio-tabs, Methigel) and ammonium chloride
(Uroeze).
Once the uroliths are dissolved or removed, s are
then maintained on diets that produce acid urine.
Uroliths that form in acid urine (calcium oxalate,
cystine, and ammonium urate uroliths)
Place in urine-alkalinizing diets
Urinary alkalinizers such as potassium citrate
(Urocit-K) and sodium bicarbonate (generic).
Patient with renal disease should not be given
acidifying diets or prescribed urinary-acidifying
drugs.
Some uroliths, such as ammonium urate uroliths,
also indicate the need for a low-protein, low-purine,
low oxalate diet to prevent recurrence.
Patient with ammonium urate uroliths are also often
prescribed xanthine oxidase inhibitors.
• This group of drugs decreases the production of uric
acid.
8. • Decreasing uric acid production helps prevent the
formation of ammonium urate uroliths.
• Allopurinol (Zyloprim, Lopurin) is an example of a
xanthine oxidase inhibitor.
Side effects of allopurinol use are rare.
URINARY INCONTINENCE
Urinary incontinence is the loss of voluntary control
of micturition (a two stage process involving the
passive storage of urine and the active voiding of
urine).
Urinary incontinence can be divided into two main
categories:
1. Disorders due to neurologic disorders
2. Nonneurologic disorders.
Neurologically Caused Incontinence
Cholinergic agonists (parasympathomimetic agents)
are used to treat patients with ―spinal cord
bladders‖—that is, damage to the nerves that control
relaxation of the urinary bladder outflow sphincters.
This nerve damage results in the retention of urine.
Mechanism of Action : The cholinergic agonist binds
to the receptors on smooth muscles, allowing sodium
and calcium to enter the cells.
Pharmacokenitics
• Cholinergic agonists promote voiding of urine from
the urinary bladder.
• These drugs simulate the action of acetylcholine by
direct stimulation of cholinergic receptors.
• This influx of sodium and calcium in turn allows
muscle contraction.
• Tone of the detrusor muscle of the urinary bladder is
increased, which may increase detrusor muscle
contractions.
Drugs
An example of a cholinergic agonist is bethanechol
(Urecholine, Duvoid, Urabeth).
Side effects include: GI signs such as vomiting and
diarrhea.
Neurologically Caused Incontinence
Anticholinergics (parasympatholytic drugs) are used
to treat urinary incontinence by promoting urine
retention in the urinary bladder.
Mechanism of Action : blocking the binding of
acetylcholine to its receptor sites and thereby
causing muscle relaxation.
Anticholinergics. These medications can calm an
overactive bladder and may be helpful for urge
incontinence.
Examples include oxybutynin (Ditropan XL),
tolterodine (Detrol), darifenacin (Enablex),
9. fesoterodine (Toviaz), solifenacin (Vesicare) and
trospium chloride.
Mirabegron (Myrbetriq).
• Mirabegron (Myrbetriq). Used to treat urge
incontinence, this medication relaxes the bladder
muscle and can increase the amount of urine your
bladder can hold. It may also increase the amount
you are able to urinate at one time, helping to empty
your bladder more completely.
Alpha blockers.
• Alpha blockers. In men who have urge incontinence
or overflow incontinence, these medications relax
bladder neck muscles and muscle fibers in the
prostate and make it easier to empty the bladder.
Examples include tamsulosin (Flomax), alfuzosin
(Uroxatral), silodosin (Rapaflo), and doxazosin
(Cardura).
Topical estrogen
• Topical estrogen. Applying low-dose, topical
estrogen in the form of a vaginal cream, ring or patch
may help tone and rejuvenate tissues in the urethra
and vaginal areas.
Neurologically Caused Incontinence
• Adrenergic antagonists are divided into alpha and
beta categories.
• Indication : Beta-adrenergic antagonists, used in the
treatment of hypertension.
• Alpha-adrenergic antagonists are used to decrease
the tone of internal urethral sphincters; they are
useful in the treatment of decreased urinary tone due
to overdistention of the urinary bladder.
Mechanism of Action
• Mechanism of Action : Alpha-adrenergic antagonists
work by blocking circulating epinephrine or
norepinephrine from binding to their receptors.
These drugs are also used to decrease blood
pressure.
Examples of alpha-adrenergic antagonists include
phenoxybenzamine
• (Dibenzyline), prazosin (Minipress), and nicergoline
(Sermion).
The main side effect of these drugs is weakness due
to decreased blood pressure.