Battered Baby Syndrome.pptx
•Descargar como PPTX, PDF•
2 recomendaciones•1,686 vistas

Battered Baby Syndrome child abuse Maltreatment syndrome

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Battered Baby Syndrome.pptx
Similar a Battered Baby Syndrome.pptx (20)
Último
Último (20)
Battered Baby Syndrome.pptx
- 1. Battered Baby Syndrome 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 1
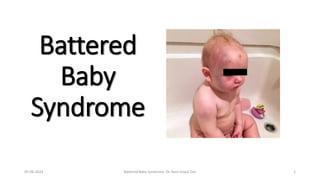
- 2. Definition: A battered child is one who has received repetitive physical injuries as a result of non-accidental violence produced by a parent or a guardian. Synonyms: 1. Caffey Syndrome 2. Caffey- Kempe syndrome 3. Maltreatment Syndrome 4. Parent-infant Traumatic Stress Syndrome 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 2
- 3. Features RELATED TO THE CHILD i. Age: The majority is below 3 years of age. ii. Sex: M:F ratio 2:1 iii. Status of the child: Illegitimate & unwanted children—pregnancy before marriage or failure of contraception. iv. Position in family: Eldest or youngest. The child may be a mentally abnormal one. 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 3
- 4. RELATED TO THE PARENT/GUARDIAN i. Marital status: Unmarried couple(western) ii. Age of parents: Parents are young iii. Educational status: Lower level of education iv. Addiction: Reckless life style, often indulging in drugs. v. Childhood history: History of battering during their childhood. vi. Psychological factors: Low tolerance threshold, impulsive nature, aggressive personality and imbalanced temperament. 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 4
- 5. Socio-familial factors 1. Low social background 2. Lack of equality & harmony between members of the family 3. Long-standing emotional problem 4. Financial hardship 5. Trouble at the place of work 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 5
- 6. Precipitating factors 1. Act of disobedience by the child. 2. Frequent crying may create annoyance. 3. Refusal to take food. 4. Soiling of napkin or bedclothes. 5. Any trifle act of the child may annoy the mentally challenged parents. 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 6
- 7. Features Arising Suspicion of Abuse • Vague & inconsistent history. • Late medical attention. • Injuries in different stages of healing. • In many cases, the parents later admit to have assaulted their children. 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 7
- 8. How to differentiate from accidental injuries A. Typically involve bony prominences 1. Head: Forehead, occipital or parietal region 2. Nose 3. Chin 4. Palm 5. Elbows 6. Knees and shin B. Match the history given by the parents. 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 8
- 9. Fig.: Surface injuries i. Surface injuries: • Bruises, abrasions and lacerations. • Laceration of the oral mucosa along with labial frenulum of the lower lip is a characteristic lesion. • Slap marks, lash mark, knuckle punches, pinch mark, bald patches on scalp due to pulling out the hair (traumatic alopecia) may be seen. 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 9
- 10. ii. CNS: Injuries are inflicted by throwing the child, striking the child with fist or object or against a wall, dropping the child or vigorous shaking of the infant (Shaken baby syndrome or infantile whiplash syndrome) leading to intracranial hemorrhage. • History: A strong suspicion of child abuse in a child presenting with altered mental status, unresponsiveness, coma, convulsions or with focal neurologic deficit. • The triad of injuries includes encephalopathy, retinal hemorrhages and SDH. SDH is the most consistent component of the triad and may be the first clinical sign identified on CT scan. 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 10
- 11. iii. Eyes: Retinal hemorrhages and lens displacement may be seen. iv. Visceral injuries: Injury to spleen, liver or hollow viscera can occur resulting in massive hemorrhage, shock and death of the child. v. Burns: Small circular pitted burns may indicate deliberate stubbing of cigarette ends on skin. Scalds are also common. vi. Skeletal injuries: Bony injuries include fractures, subperiosteal hematoma, and multiple deformities of the long bones and rib cage of the body due to multiple healed fractures and callus formation. 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 11
- 12. • The fractured ribs heal by callus formation in 1–2 weeks, giving characteristic appearance of a knob (knob fractures) • X-ray ‘string of beads’ appearance is seen in paravertebral gutter. • In whiplash movement of arms and legs, typical ‘corner’ or ‘bucket-handle’ fractures in the metaphyseal region may be seen 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 12
- 13. vii. CVS: Blunt trauma to chest may cause multiple rib fractures leading to lung and heart contusions, pneumothorax, haemothorax, rupture of diaphragm and cardiac tamponade. viii. Genitourinary system: Physical and sexual abuse should be considered in a child presenting with haematuria, dysuria, increased frequency of urination and enuresis. 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 13
- 14. Fig. : Internal injuries 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 14
- 15. Diagnosis 1. Nature of injuries. 2. Delay in seeking medical treatment. 3. Recurrent injuries. 4. Radiological manifestations, especially those involving the ribs, metaphyseal-epiphyseal injuries, and avulse fractures of the clavicle and acromion process. Head injury with or without skull fracture is the leading cause of death in child abuse followed by rupture of an abdominal viscus. 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 15
- 16. Sudden Infant Death Syndrome [Cot Death (UK) or Crib Death (US)] • Definition: Sudden and unexpected death of seemingly healthy infant whose death remains unexplained even after complete autopsy. • It is an autopsy diagnosis, and not a clinical diagnosis. 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 16
- 17. Features 1. Incidence: 0.2–0.4% of all live births. 2. Geographical distribution: Worldwide. 3. Age: 2 weeks to 2 years. Mid infancy is the most vulnerable age (peak 2– 4 months). 4. Sex: M:F ratio 3:2 5. Socio-economic status: Low and middle class family with poor housing condition, large family and lack of health consciousness. 6. Time of death: In most cases, early morning or after first feed in the morning. 7. Season: In most occasions, rainy and winter seasons in temperate zones. 8. Twins: More among twins (two-fold) as opposed to singletons. Prematurity and low birth weights increases the risk of SIDS. 9. Addiction: Smoking and drug abuse by pregnant women increases risk. 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 17
- 18. Cause No definite cause is known. 1. Prolonged sleep apnea: Most acceptable of the suggested causes. A periodic failure to breath during sleep makes them susceptible to hypoxia. 2. Respiratory infection: Viremia which leads to sleep depression of respiratory center and death. 3. Cow’s milk allergy: Local hypersensitivity of the respiratory tract lumen cause laryngeal spasm. 4. Accidental Asphyxia: Bedclothes and pillow 5. Overlying: Sleeping or intoxicated mother. 6. Sleeping position: sleep prone or on their side increases the risk of SIDS. 7. Family history: Increased risk 8. Miscellaneous causes: Conduction system anomalies; hypoparathyroidism; deficiency of Se, Ab, Ca, Mg and vitamins B, C, D and E; house-mite allergy; Sodium overload in feeds and hypothermia. 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 18
- 19. Postmortem Findings • Post mortem findings are negative. • Trachea contains milky vomit, sometimes bloodstained with shed epithelial cells. • Multiple petechial hemorrhages on heart (posterior epicardial surface), lungs and thymus—agonal in nature. • Pulmonary edema is common. • Milk or bloodstained froth on child’s mouth or bedding. • Hands are often clenched around fibers from bedclothes. 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 19
- 20. Medico-legal Aspects • SIDS is a natural death in which the parents may be wrongfully linked for having criminal involvement or negligence. • Some infanticide cases may be presented as cot death cases. 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 20
- 21. Munchausen Syndrome by Proxy [Factitious Disorder] • MSBP is a form of abuse in which parent or guardian fabricates or produces symptoms of an illness in a child in order to gain sympathy or attention for themselves. • The parents frequently have abnormal or borderline personality disorder. • Diagnosis may require a high level of suspicion and may be met with considerable resistance from family. 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 21
- 22. Features 1. The child may be brought with vague complaints inflicted by the parent intentionally and repeatedly. • Bleeding caused by anticoagulants & simulated by exogenous blood • Seizures by suffocations, shaking or intoxications • Vomiting by giving ipecac syrup • Fever triggered by injecting contaminants into IV lines 2. The parent or guardian derives some non-economic benefit at the expense of the victim. 3. Some perpetrators ‘doctor shop’ while some maintain a constant relationship with one or more health care providers. 4. When confronted, the parent or guardian usually denies any allegations. 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 22
- 23. Diagnosis 1. The illness does not conform to the expected presentation. 2. Signs & symptoms are not substantiated by laboratory findings. 3. Failure of wounds to heal. 4. The child becomes ill or worsens when the parent or guardian is present, with recovery when separated. 5. Positive toxicological analysis for something not prescribed. 6. Admitted to multiple hospitals & seen by multiple physicians. 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 23
- 24. PRECIPITATE LABOUR • Labour terminating in a very short time than that taken on the average, either in a primipara or multipara. • Delivery occurs suddenly and rapidly without the knowledge of the mother. • The foetus is normal or premature. • It is possible in multiparae, but is extremely rare in primiparae. • A woman may be delivered unconsciously during fits or periods of coma, hysteria, hypnosis, under the influence of narcotic drugs, anaesthetics, and even deep drunkenness. 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 24
- 25. CAUSE OF DEATH (1) Suffocation by falling into a lavatory pan (2) Head injury and fracture of the skull (3) Haemorrhage from the torn end of the cord 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 25
- 26. Medicolegal Importance (1) The mother or her relatives may be accused of killing the infant. (2) In a case of murder, death of the child may be attributed to precipitate labour. Mother is examined for: a. Birth passage as compared to the head of foetus b. Signs of recent, rapid & sudden delivery, multiparity, old perineal tear etc. Foetus is to be examined for: a. Absence of moulding of head b. Umbilical cord & placenta for length and strength c. Injury over the head d. Evidence of mud, sand, gravel over the scalp 05-06-2023 Battered Baby Syndrome Dr. Nani Gopal Das 26
- 27. OSCE= OBJECTIVE STRUCTURED CLINICAL EXAMINATION OSPE= OBJECTIVE STRUCTURED PRACTICAL EXAMINATION
- 28. OSCE/OSPE on Infanticide Q. Take history from the mother of the child aged 3 years, who is showing different injuries at different stages of healing and the child is crying unconsolably with deformity of left arm? Sr. No. Competency Domain Level Core Practical 1. Student should be able to define Battered Baby Syndrome K- Knowledge K- Knows Core Yes 2. Student should recognise signs & symptoms of Battered Baby Syndrome S- Skill SH- Shows How Core Yes 3. Student should be able to document the findings in support of his opinion S- Skill SH- Shows How Core Yes 4. Student should be able to diagnose Battered Baby Syndrome S- Skill SH- Shows How Core Yes
- 29. Examiner check list for Questions Sr. No. Act/ Procedure/ Skill done by student Yes No Marks 1. Introduces self to the mother of the child 2. Taks informed consent from the mother/ guardian 3. Asks about present incident and time taken to seek medical attention 4. Takes history of rest of the injuries of different duration 5. Takes history of problem in the family/ socioeconomic background 6. Takes history about number of children/ wanted or unwanted child 7. Informs child helpline/ police about Battered Baby Syndrome 8. Makes provisional diagnosis of Battered Baby Syndrome Play card questions (each question carries 1 mark) 1. Give examples of precipitating factors in such cases. 2. What are the radiological manifestations of trauma in such a case?