Antidiabetic drugs
•Descargar como PPTX, PDF•
15 recomendaciones•18,370 vistas

Antidiabetic drugs

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Antidiabetic drugs
Similar a Antidiabetic drugs (20)
Más de Subramani Parasuraman
Más de Subramani Parasuraman (20)
Último
Último (20)
Antidiabetic drugs
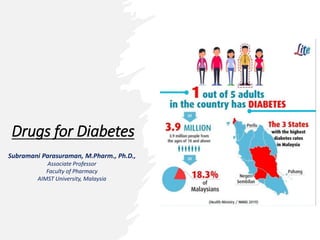
- 1. Drugs for Diabetes Subramani Parasuraman, M.Pharm., Ph.D., Associate Professor Faculty of Pharmacy AIMST University, Malaysia
- 2. Diabetes • Diabetes is a chronic disease that occurs either when the pancreas does not produce enough insulin or when the body cannot effectively use the insulin it produces. • Types: • Type I: Insulin-dependent diabetes mellitus (IDDM)/ juvenile onset diabetes mellitus • Cause: Loss of β-cell function in type 1 diabetes • Treatment: Exogenous insulin to control hyperglycemia • Type II: Noninsulin-dependent diabetes mellitus (NIDDM)/ maturity onset diabetes mellitus • Cause: Lack of sensitivity of target organs to insulin • Treatment: Weight reduction, exercise, dietary modification, hypoglycemic agents, insulin therapy
- 3. Diabetes • The incidence of diabetes is growing rapidly worldwide. • Malaysia has the highest rate of diabetes in Western Pacific region and one of the highest in the world and costing around 600 million US dollars per year. • The prevalence of diabetes raised from 11.2% in 2011 to 18.3% in 2019, with a 68.3% increase. According to a national survey report, in Malaysia in 2019, 3.6 million adults had diabetes. Diabetes is expected to affect 7 million Malaysian adults aged 18 and older by 2025. Ref: PMID: 35085366
- 4. Comparison of type 1 and type 2 diabetes
- 5. Insulin • Insulin is a two-chain polypeptide having 51 amino acids and MW about 6000. The A-chain has 21 while B-chain has 30 amino acids. Under basal condition ~1U insulin is secreted per hour by human pancreas. Human proinsulin
- 6. Insulin • Mechanism of action: Exogenous insulin is administered to replace absent insulin secretion in type 1 diabetes or to supplement insufficient insulin secretion in type 2 diabetes. • Pharmacokinetics: Insulin is a polypeptide; it is degraded in the gastrointestinal tract if taken orally. Therefore, it is generally administered by subcutaneous injection. Inhaled insulin formulation is also available • Adverse effects: Hypoglycemia, weight gain, local injection site reactions, and lipodystrophy. Hypoglycaemia is managed by administering glucose (or glucose yielding carbohydrate, e.g., sugar) 15–20 g orally reverses the symptoms.
- 7. Insulin preparations • Rapid-acting and short-acting insulin preparations • Intermediate-acting insulin • Long-acting insulin preparations • Insulin combinations • Insulin delivery devices
- 8. Insulin preparations • Rapid-acting and short-acting insulin preparations: • Five preparations fall into this category: regular insulin, insulin lispro, insulin aspart, insulin glulisine, and inhaled insulin. • Regular insulin (peck level at 50 to 120 minutes) is a short-acting, soluble, crystalline zinc insulin. • Insulin lispro (peck level at 30 to 90 minutes), aspart, and glulisine are classified as rapid- acting insulins. • Inhaled insulin is also considered rapid-acting. This dry powder formulation is inhaled and absorbed through pulmonary tissue, with peak levels achieved within 45 to 60 minutes. • Regular insulin should be injected subcutaneously 30 minutes before a meal, whereas rapid-acting insulins are administered in the 15 minutes proceeding a meal or within 15 to 20 minutes after starting a meal. • Rapid-acting insulin suspensions are commonly used in external insulin pumps, and they are suitable for IV administration.
- 9. Insulin preparations • Intermediate-acting insulin: Neutral protamine hagedorn (NPH) insulin is an intermediate-acting insulin formed by the addition of zinc and protamine to regular insulin. NPH insulin is used for basal (fasting) control in type 1 or 2 diabetes and is usually given along with rapid- or short-acting insulin for mealtime control. NPH insulin should be given only subcutaneously (never IV). • Long-acting insulin preparations: It has a slower onset than NPH insulin and a flat, prolonged hypoglycemic effect with no peak. Eg: Insulin glargine, Insulin degludec
- 10. Insulin preparations • Insulin combinations: Various premixed combinations of human insulins [70% NPH insulin + 30% regular insulin/ 50% NPH insulin + 50% regular insulin]. Use of premixed combinations decreases the number of daily injections but makes it more difficult to adjust individual components of the insulin regimen. • Insulin delivery devices: • Syringes • Pens • Durable pens • Pumps • Jet injectors • Others
- 11. Oral antidiabetic drugs • These drugs lower blood glucose levels in diabetics and are effective orally. The main drawback of insulin is - it must be given by injection.
- 13. Sulfonylureas • Sulfonylureas more potent and clinically superior. All first- generation compounds have been discontinued except tolbutamide which is infrequently used. • Mechanism of action: Sulfonylureas bind to a specific ‘sulfonylurea receptor’ (SUR1) located on the pancreatic β cell membrane and provoke a brisk release of insulin. • Pharmacokinetics: All SUs are well absorbed orally and are 90% or more bound to plasma proteins: have low volumes of distribution (0.2–0.4 L/kg). Most sulfonylureas are extensively metabolized in the liver, primarily by the CYP2C9 isoenzyme and excreted in urine. • Adverse effects: Incidence of adverse effects is quite low (3–7%). Hypoglycaemia, hypersensitivity and nonspecific side effects such as weight gain, Nausea, vomiting, flatulence, diarrhoea or constipation, headache and paresthesias.
- 14. Meglitinide/D-phenylalanine analogues • Drugs: Repaglinide, Nateglinide • Mechanism of action: Like the sulfonylureas, the glinides stimulate insulin secretion. These are KATP channel blockers with a quick and short lasting insulinemic action. • Pharmacokinetics: Glinides should be taken prior to a meal and are well absorbed after oral administration. Both glinides are metabolized to inactive products by cytochrome P450 3A4 (CYP3A4) in the liver and are excreted through the bile. • Adverse effects: Although glinides cause hypoglycemia and weight gain, the incidence is lower than that with sulfonylureas.
- 15. Dipeptidyl peptidase-4 (DPP-4) inhibitors • Drugs: Sitagliptin, Vildagliptin, Saxagliptin, Teneligliptin • Mechanism of action: These drugs inhibit the enzyme DPP-4, which is responsible for the inactivation of incretin hormones such as glucagon-like peptide (GLP-1). Prolonging the activity of incretin hormones increases release of insulin in response to meals and reduces inappropriate secretion of glucagon. • Pharmacokinetics: The DPP-4 inhibitors are well absorbed after oral administration. Food does not affect the extent of absorption. Sitagliptin are mostly excreted unchanged in the urine. Saxagliptin is metabolized via CYP450 3A4/5 to an active metabolite. All DPP-4 inhibitors except linagliptin require dosage adjustments in renal dysfunction. • Adverse effects: DPP-4 inhibitors are well tolerated, with the most common adverse effects being nasopharyngitis and headache.
- 16. Biguanide (AMPK activator) • Drugs: Metformin, Phenformin [Phenformin is banded in many countries because of higher risk of lactic acidosis] • Mechanism of action: Metformin is a complex drug with multiple sites of action. Metformin acts directly or indirectly on the liver to lower glucose production, and acts on the gut to increase glucose utilisation, increase GLP-1 and alter the microbiome. • Pharmacokinetics: Metformin is well absorbed after oral administration, is not bound to serum proteins, and is not metabolized. Excretion is via the urine. • Adverse effects: Side effects with metformin are frequent, but generally not serious. Others: Diarrhea, nausea, and vomiting, metallic taste, tiredness. Metformin does not cause hypoglycaemia except in overdose.
- 17. Thiazolidinedione (PPARγ agonist) • Drugs: Pioglitazone, Rosiglitazone • Mechanism of action: The thiazolidinediones (TZDs) are also insulin sensitizers. The TZDs lower insulin resistance by acting as agonists for the peroxisome proliferator–activated receptor-γ (PPARγ), a nuclear hormone receptor. Activation of PPARγ regulates the transcription of several insulin-responsive genes, resulting in increased insulin sensitivity in adipose tissue, liver, and skeletal muscle. The TZDs can be used as monotherapy or in combination with other glucose-lowering agents or insulin. • Pharmacokinetics: Oral administration, metabolized by CYP450, Pioglitazone- excreted in the bile and eliminated in the feces, Rosiglitazone - primarily excreted in the urine. No dosage adjustment is required in renal impairment. • Adverse effects: Liver toxicity, osteopenia, Pioglitazone may also increase the risk of bladder cancer, rosiglitazone carries a boxed warning about the potential increased risk of myocardial infarction and angina.
- 18. α Glucosidase inhibitors • Drugs: Acarbose, Miglitol, Voglibose • Mechanism of action: These drugs reversibly inhibit α- glucosidase enzymes and delay the digestion of carbohydrates, resulting in lower postprandial glucose levels. They do not stimulate insulin release or increase insulin sensitivity; these agents do not cause hypoglycemia when used as monotherapy. • Adverse effects: The most common adverse effects are flatulence, diarrhea, and abdominal cramping.
- 19. Dopamine D2 agonist • Drugs: Bromocriptine. Used as adjunctive treatment of type 2 DM. • Mechanism of action: Bromocriptine is thought to act on the circadian neuronal activities in the hypothalamus, to reset an abnormally elevated hypothalamic drive for increased plasma glucose, free fatty acids, and triglycerides in insulin-resistant patients. Contraindicated in patients with renal insufficiency.
- 20. Sodium-glucose co-transport-2 (SGLT-2) inhibitor • Drugs: Dapagliflozin, Canagliflozin • Mechanism of action: The SGLT2 is responsible for reabsorbing filtered glucose in the tubular lumen of the kidney. By inhibiting SGLT2, these agents decrease reabsorption of glucose, increase urinary glucose excretion, and lower blood glucose. Inhibition of SGLT2 also decreases reabsorption of sodium and causes osmotic diuresis reduce systolic blood pressure (not indicated for the treatment of hypertension). • Pharmacokinetics: Before the first meal of the day, metabolized by glucuronidation, avoided in patients with renal dysfunction • Adverse effects: Mycotic infections (in females), urinary tract infections, and urinary frequency, hypotension (elderly), Ketoacidosis
- 21. Bile acid sequestrant • Drug: Colesevelam • It is a bile acid binding resin which lowers cholesterol as well as glucose levels in blood. It is approved as add-on drug in type 2 DM patients who are not properly controlled by other antidiabetic drugs. The mechanism of action is not clear.
- 22. Oral hypoglycemic agents, dose range and dose frequency MEDICINE USUAL DAILY DOSE FREQUENCY Glibenclamide 5 mg 2.5–20 mg • Up to 10 mg as a single dose • >10 mg in divided doses • Taken with or immediately before food Glipizide 5 mg 2.6–40 mg • Up to 15 mg as a single dose • >15 mg in a twice daily dosage taken • immediately before meals Gliclazide 80 mg 30–120 mg • Daily Glimepiride 1/ 2 mg 1–4 mg • 2–3 per day Metformin 500 mg, 1g 0.5–1.5 g • 1–3 times/day taken with or immediately after food Repaglinide 0.5 mg, 1/ 2 mg 0.5–16 mg • 2–3 per day Pioglitazone 15 mg, 30 mg 4–8 mg • Daily Rosiglitazone 2 mg, 4 mg 4–8 mg • Daily Acarbose 50/ 100 mg 50–100 mg • TDS with food thrice a day Voglibose 0.2/ 0.3 mg 0.2–0.3 mg • TDS with food thrice a day Sitagliptin 50/ 100 mg 100 mg per day in BD regimen. In combination with metformin, or a sulfonylurea • With or without food Vildagliptin 50 mg • With or without food
- 23. Ref: https://www.puremed.com.my/world-diabetes-day-5-minutes-read/ [last assessed on 25-12-2022]
Notas del editor
- Paresthesia refers to a burning or prickling sensation that is usually felt in the hands, arms, legs, or feet, but can also occur in other parts of the body.
- Paresthesia refers to a burning or prickling sensation that is usually felt in the hands, arms, legs, or feet, but can also occur in other parts of the body.
- Paresthesia refers to a burning or prickling sensation that is usually felt in the hands, arms, legs, or feet, but can also occur in other parts of the body.
- Paresthesia refers to a burning or prickling sensation that is usually felt in the hands, arms, legs, or feet, but can also occur in other parts of the body.