
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Orthomyxovirus, Influenza.pptx
Similar a Orthomyxovirus, Influenza.pptx (20)
Último
Último (20)
Orthomyxovirus, Influenza.pptx
- 2. Important question • What are the structure / Unique properties of Influenza virus • What is antigenic shift and antigenic drift. *** • Lab diagnosis of influenza virus • What are the respiratory virus.
- 3. Respiratory Viruses • Almost all of the respiratory tract viruses have RNA as their genome; one has DNA. Most are enveloped viruses, whereas two, rhinovirus and adenovirus, are nonenveloped. • In addition, the enveloped respiratory viruses belong to several different virus families, namely, orthomyxoviruses, paramyxoviruses, and coronaviruses. • The feature that unites all of these viruses is their ability to infect the mucosal cells of the respiratory tract and cause significant symptoms there.
- 4. Clinical Features of Respiratory Viruses
- 5. Properties of Respiratory Viruses
- 7. INFLUENZA VIRUS- Properties • Influenza virus is an important human pathogen because it causes both outbreaks of influenza that sicken and kill thousands of people each year as well as infrequent but devastating worldwide epidemics (pandemics). • Influenza virus is the only member of the orthomyxovirus family. The orthomyxoviruses differ from the paramyxoviruses primarily in that the former have a segmented RNA genome (usually eight pieces), whereas the RNA genome of the latter consists of a single piece. • The term myxo refers to the observation that these viruses interact with mucins (glycoproteins on the surface of cells).
- 8. Human Influenza Virus- Properties • Influenza A virus causes worldwide epidemics (pandemics) of influenza, influenza B virus causes major outbreaks of influenza, and influenza C virus causes mild respiratory tract infections but does not cause outbreaks of influenza. Pandemics occur when a variant of influenza A virus that contains a new hemagglutinin against which people do not have preexisting antibodies is introduced into the human population. • Most cases of influenza are caused by H1N1 and H3N2 strains of influenza A virus .However, in 1997, an outbreak of human influenza (avian influenza, bird flu) caused by an H5N1 strain of influenza A virus began
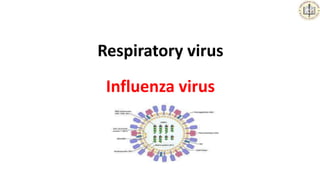
- 9. Human Influenza Virus- Structure • Influenza virus is composed of a segmented single-stranded RNA genome, a helical nucleocapsid, and an outer lipoprotein envelope. • The envelope is covered with two different types of spikes, a hemagglutinin and a neuraminidase. • Influenza A virus has 16 antigenically distinct types of hemagglutinin and 9 antigenically distinct types of neuraminidase. • Some of these types cause disease in humans, but most of the types typically cause disease in other animal species such as birds, horses, and pigs
- 10. Human Influenza Virus- Structure
- 11. Human Influenza Virus- Structure • The function of the hemagglutinin is to bind to the cell surface receptor (neuraminic acid, sialic acid) to initiate infection of the cell. The hemagglutinin is the target of neutralizing antibody (i.e., antibody against the hemagglutinin inhibits infection of the cell). • The neuraminidase cleaves neuraminic acid (sialic acid) to release progeny virus from the infected cell. • The hemagglutinin functions at the beginning of infection, whereas the neuraminidase functions at the end. • Neuraminidase also degrades the protective layer of mucus in the respiratory tract. This enhances the ability of the virus to gain access to the respiratory epithelial cells
- 12. Human Influenza Virus- Replication
- 13. Human Influenza Virus- Changes • Influenza viruses, especially influenza A virus, show changes in the antigenicity of their hemagglutinin and neuraminidase proteins; this property contributes to their capacity to cause devastating worldwide epidemics (pandemics). • There are two types of antigenic changes: (1) antigenic shift, which is a major change based on the reassortment of segments of the genome RNA and (2) antigenic drift, which is a minor change based on mutations in the genome RNA
- 14. Antigenic Shift • Antigenic shift reflects drastic changes in the sequence of a viral surface protein, changes too extreme to be explained by mutation. The segmented genomes of influenza viruses reassort readily in doubly infected cells. The mechanism for shift is genetic reassortment between human and avian influenza viruses. Influenza B and C viruses do not exhibit antigenic shift because few related viruses exist in animals.
- 15. Antigenic Shift • Many species of animals (e.g., aquatic birds, chickens, swine, and horses) have their own influenza A viruses. These animal viruses are the source of the RNA segments that encode the antigenic shift variants that cause epidemics among humans. For example, if an avian and a human influenza A virus infect the same cell (e.g., in a farmer’s respiratory tract), reassortment could occur and a new variant of the human A virus, bearing the avian virus hemagglutinin, may appear.
- 16. Antigenic Drift • Antigenic drift is caused by the accumulation of point mutations in the gene, resulting in amino acid changes in the protein. Sequence changes can alter antigenic sites on the molecule such that a virion can escape recognition by the host’s immune system.
- 17. Human Influenza Virus- Changes Antigenic shift in influenza virus. A human strain of influenza virus containing the gene encoding one antigenic type of hemagglutinin (colored orange) infects the same lung cell as a chicken strain of influenza virus containing the gene encoding a different antigenic type of hemagglutinin (colored black).
- 18. Human Influenza Virus- Changes Antigenic drift and antigenic shift account for antigenic changes in the two surface glycoproteins (hemagglutinin [HA] and neuraminidase [NA]) of influenza virus. Antigenic drift is a gradual change in antigenicity caused by point mutations that affect major antigenic sites on the glycoprotein. Antigenic shift is an abrupt change caused by genetic reassortment with an unrelated strain.
- 20. Important Properties of Orthomyxoviruses a
- 21. Human Influenza Virus- Antigens Influenza viruses have both group-specific and type specific antigens. • (1) The internal ribonucleoprotein in the nucleocapsid is the group-specific antigen that distinguishes influenza A, B, and C viruses. • (2) The hemagglutinin and the neuraminidase are the type specific antigens located on the surface. • Antibody against the hemagglutinin neutralizes the infectivity of the virus (and prevents disease), whereas antibody against the group-specific antigen (which is located internally) does not. • Antibody against the neuraminidase does not neutralize infectivity but does reduce disease by decreasing the amount of virus released from the infected cell and thus reducing spread of the virus to adjacent cells.
- 22. Transmission & Epidemiology • The virus is transmitted by airborne respiratory droplets. The ability of influenza A virus to cause epidemics is dependent on antigenic changes in the hemagglutinin and neuraminidase. • As mentioned previously, influenza A virus undergoes both major antigenic shifts as well as minor antigenic drifts. Antigenic shift variants appear infrequently, whereas drift variants appear virtually every year. • Epidemics and pandemics (worldwide epidemics) occur when the antigenicity of the virus has changed sufficiently that the preexisting immunity of many people is no longer effective. • The antigenicity of influenza B virus undergoes antigenic drift but not antigenic shift.
- 23. Pathogenesis & Immunity • Influenza virus infection causes inflammation of the mucosa of upper respiratory tract sites such as the nose and pharynx, and lower respiratory tract sites such as the larynx, trachea, and bronchi. Pneumonia, which involves the alveoli, may also occur. • After the virus has been inhaled, the neuraminidase degrades the protective mucus layer, allowing the virus to gain access to the cells of the upper and lower respiratory tract. • Immunity depends mainly on secretory IgA in the respiratory tract. IgG is also produced but is less protective. Cytotoxic T cells also play a protective role.
- 25. Pathogenesis of influenza A virus
- 26. Risk Factors- Influenza virus
- 27. Clinical Findings • After an incubation period of 24 to 48 hours, fever, myalgias, headache, sore throat, and cough develop suddenly. Severe myalgias (muscle pains) coupled with respiratory tract symptoms are typical of influenza. • Vomiting and diarrhea are rare. The symptoms usually resolve spontaneously in 4 to 7 days, but influenzal or bacterial pneumonia may complicate the course. • One of the well-known complications of influenza is pneumonia caused by either Staphylococcus aureus or Streptococcus pneumoniae. • Reye syndrome : is an acute encephalopathy of children and adolescents, usually between 2 and 16 years of age. The mortality rate is high (10–40%).
- 28. Diseases Associated With Influenza Virus Infection
- 29. Laboratory Diagnosis • Although most diagnoses of influenza are made on clinical grounds, laboratory tests are available. A PCR- based test that detects influenza virus RNA in respiratory specimens is commonly used in hospitals. • Enzyme-linked immunosorbent assay (ELISA) for viral antigen in respiratory secretions such as nasal or throat washings, nasal or throat swabs, or sputum. • Influenza can also be diagnosed by the detection of antibodies in the patient’s serum. A rise in antibody titer of at least fourfold in paired serum samples taken early in the illness and 10 days later is sufficient for diagnosis. Either the hemagglutination inhibition or complement fixation (CF) test can be used assay the antibody titer. • Other tests such as direct fluorescent antibody on respiratory specimens and virus isolation in cell culture can also be used.
- 30. Laboratory Diagnosis Fluroscence antibody test Hemagglutination inhibition test
- 31. Laboratory Diagnosis- Influenza virus
- 32. Treatment • Oseltamivir taken orally and zanamivir inhaled into the nose are the two most commonly used drugs for the treatment of influenza. They are neuraminidase inhibitors. • Amantadine , Rimantadin block the M2 ion channel, thereby inhibiting uncoating.
- 33. Prevention • The main mode of prevention is the vaccine, which contains both influenza A and B viruses. The vaccine is usually reformulated each year to contain the current antigenic strains. • There are two main types of influenza vaccines available, a killed vaccine and a live, attenuated vaccine. • Hemagglutinin is the most important antigen because it elicits neutralizing antibody. • Live, attenuated vaccine containing temperature-sensitive mutants of influenza A and B viruses. These temperature-sensitive mutants can replicate in the cooler (33°C) nasal mucosa where they induce IgA, but not in the warmer (37°C) lower respiratory tract. The live virus in the vaccine therefore immunizes but does not cause disease. There is no evidence of reversion to virulence. • killed vaccine is not a good immunogen, because little IgA is made and the titer of IgG is relatively low.
- 34. Avian Influenza , Swine Influenza • Avian Influenza Virus Infection in Humans H5N1 Influenza Virus H7N9 Influenza Virus • Swine Influenza Virus Infection in Humans Influenza A (H1N1)
- 36. Case study -1 • A three-year-old girl with a past history of failure to thrive, who was up to date with her childhood vaccines, presented Hospital emergency department with a five-day history of fever, coryzal symptoms and lethargy. Her general practitioner (GP) had commenced oral antibiotics a few days earlier but she had deteriorated in the preceding 24 hours with slurred speech and a fluctuating conscious state. • She had no neck stiffness or light sensitivity. Her parents and older sister were also unwell with coryzal symptoms at the time. In the emergency department she was confirmed to have a fluctuating Glasgow Coma Scale (9 to 13), with increased tone and brisk reflexes throughout. Blood tests suggested a viral illness, and she had normal inflammatory markers. • A CT scan of the brain did not identify a cause. Lumbar puncture was withheld, and she was commenced on intravenous antibiotics and acyclovir. She was then transferred to the intensive care unit for ongoing monitoring.
- 37. Case study -1 • The following morning she had right-sided weakness, and an MRI demonstrated extensive focal necrotic and haemorrhagic changes in the deep white matter and spinal cord (C4–C5) in keeping with acute necrotising encephalomyelitis (ANE) . A nasopharngeal aspirate was positive for influenza A . • Her cerebrospinal fluid demonstrated a mildly elevated white cell count. Bacterial culture and respiratory virus PCR on the cerebrospinal fluid was negative. • Once the diagnosis of ANE (secondary to influenza A) was confirmed, the child commenced a seven day course of antiviral medication (oseltamivir) and a three-day course of intravenous steroids (pulse methylprednisolone), followed by an oral weaning course of prednisolone.
- 38. Case study -1 Hyperintense signals involving bilateral external capsules and putamen (diagonal arrow points to right side) and thalami (horizontal arrow points to left side)
- 39. Case study -1 Learning points • Influenza can have serious consequences and be fatal in previously well children. • Neurological complications of influenza A occur in up to 10 per cent of hospitalised children. • ANE is a rare complication of influenza A, but causes death or severe neuro disability in up to 70 per cent children. • Early diagnosis and antiviral medication should be considered in hospitalised children and those children at high risk of complications.
- 40. Case study -2 • JP is a 29 year-old female presenting to the Emergency Department with dyspnea, myalgia, and rhinorrhea. Her symptoms began approximately 1 day ago and are continuous, steadily getting worse. She is having significant nasal discharge but minimal cough. Her 4 year-old son has experienced rhinorrhea as well over the past 3 days, but is not as ill as she is. She has no significant past medical history, and takes no routine medications. She reports receiving the flu vaccine when her child first fell ill, 3 days ago. She was a smoker but quit when she became pregnant 4 years ago.
- 42. Influenza viral infection showing patchy opacity