COPD.pptx
•Descargar como PPTX, PDF•
0 recomendaciones•22 vistas

Chronic Obstructive Pulmonary Disease

Recomendados
Más contenido relacionado
Similar a COPD.pptx
Similar a COPD.pptx (20)
Último
Último (20)
COPD.pptx
- 1. CHRONIC OBSTRUCTIVE PULMONARY DISEASE by Dr. OGUNLADE A.F
- 2. OUTLINE • Definition • Respiratory Anatomy • Respiratory Physiology • Epidemiology • Risk Factors
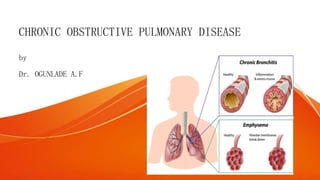
- 3. DEFINITION • Chronic obstructive pulmonary disease (COPD) is defined as a disease state characterized by persistent progressive respiratory symptoms and airflow limitation that is not fully reversible • includes emphysema • chronic bronchitis
- 4. DEFINITION • Chronic bronchitis is defined clinically as the presence of a chronic productive cough for 3 months during each of 2 consecutive years (other causes of cough being excluded). • Emphysema is defined pathologically as an abnormal, permanent enlargement of the air spaces distal to the terminal bronchioles, accompanied by destruction of their walls and without obvious fibrosis.
- 5. RESPIRATORY ANATOMY • Upper Respiratory Tract: Nasal cavity, Pharynx. Larynx, Upper part of trachea. • Lower Resoiratory Tract: Lower part of the trachea, Bronchial tree, Lungs • Functionally, the respiratory system can be divided into a conducting zone and a respiratory zone Conducting Zone- route for incoming and outgoing air, remove debris and pathogens from the incoming air, and warm and humidify the incoming air – nasal cavity, Pharynx. Larynx, trachea bronchial tree. • bronchi have walls consisting of cartilage and smooth muscle, epithelial lining with Cilia and goblet cells, submucosal mucus secreting glands, endocrine cells
- 6. RESPIRATORY ANATOMY Respiratory Zone- structures directly involved in gas exchange. • begins where the terminal bronchioles join a respiratory bronchiole, the smallest type of bronchiole, which then leads to an alveolar duct, opening into a cluster of alveoli.
- 8. RESPIRATORY PHYSIOLOGY- RESPIRATORY VOLUMES AND CAPACITIES • Tidal volume (TV) – amount of air moving in and out of the lungs with each breath (about 500ml on average) • Inspiratory reserve volume (IRV) – amount of air that can be taken in forcibly over the tidal volume • Expiratory reserve volume (ERV) – amount of air that can be forcibly exhaled over tidal volume • Residual volume – amount of air that always remains in the lungs; it cannot be exhaled. • Vital capacity – maximum amount of air that can be forcefully exchanged; VC = TV+IRV+ERV • Total lung capacity = VC+RV
- 10. EPIDEMIOLOGY • COPD is a disease of increasing public health importance around the world. • COPD is the third most common cause of death worldwide with 2.5million deaths per year(6%) and 4th most common cause of death in low income countries (WHO) • COPD affects >10 million persons in the United States. • In Africa, the estimated prevalence is 13.4% (Finney et al, 2012) • The prevalence of COPD in sub-Saharan Africa has been poorly studied. A meta-analysis of nine crosssectional studies (5 from
- 11. RISK FACTORS • Cigarette smoking (>10 packs per year) • Passive or second-hand smoking exposure • Extremes of age • Lower socio-economic group • Male gender • Increased airway responsiveness • Respiratory infections • Occupational exposures, -coal, gold, dust, and cotton. • Ambient air pollution • Alpha 1 antitrypsin deficiency
- 12. PATHOPHYSIOLOGY • Pathologic changes in chronic obstructive pulmonary disease (COPD) occur in the large (central) airways, the small (peripheral) bronchioles, and the lung parenchyma. • Most cases of COPD are the result of exposure to noxious stimuli, most often cigarette smoke. The normal inflammatory response is amplified in persons prone to COPD development. • Small airways may become narrowed by cells (hyperplasia and accumulation), mucus, and fibrosis, and extensive small airway destruction has been demonstrated to be a hallmark of advanced COPD.
- 13. EMPHYSEMA PATHOGENESIS • comprises a series of four interrelated events: • (1) Chronic exposure to cigarette smoke in genetically susceptible individuals triggers inflammatory and immune cell recruitment within large and small airways and in the terminal air spaces of the lung. • (2) Inflammatory cells release proteinases that damage the extracellular matrix supporting gas exchange surfaces of the lung. • (3) Structural cell death occurs through oxidant-induced damage, loss of cellular- matrix attachments leading to alveolar destruction. • (4) Disordered repair of elastin and other extracellular matrix components contributes to air space enlargement and emphysema.
- 15. EMPHYSEMA PATHOGENESIS • Furthermore, loss of alveoli leads to airflow limitation by 2 mechanisms. • First, loss of the alveolar walls results in a decrease in elastic recoil, which leads to airflow limitation. • Second, loss of the alveolar supporting structure leads to airway narrowing, which further limits airflow.
- 16. EMPHYSEMA PATHOGENESIS • Emphysema has 3 morphologic patterns: • Centriacinar • Panacinar • Distal acinar, or paraseptal
- 17. EMPHYSEMA PATHOGENESIS • Centriacinar emphysema - focal destruction limited to the respiratory bronchioles and the central portions of the acini. associated with cigarette smoking and typically most severe in the upper lobes. • Panacinar emphysema - entire alveolus distal to the terminal bronchiole. The panacinar type is typically most severe in the lower lung zones. generally develops in patients with homozygous alpha1- antitrypsin (AAT) deficiency. • Distal acinar emphysema, or paraseptal emphysema.- least common form and involves distal airway structures, alveolar ducts, and sacs. This form of emphysema is localized to fibrous septa or to the pleura and
- 18. CHRONIC BRONCHITIS PATHOGENESIS-FIXING • Damage to the endothelium impairs the mucociliary response that clears bacteria and mucus. • Inflammation and secretions provide the obstructive component of chronic bronchitis. • Neutrophilia develops in the airway lumen, and neutrophilic infiltrates accumulate in the submucosa. • The respiratory bronchioles display a mononuclear inflammatory process, lumen occlusion by mucus plugging, goblet cell metaplasia, smooth muscle hyperplasia, and distortion due to fibrosis. • These changes, combined with loss of supporting alveolar attachments, cause airflow limitation by allowing airway walls to deform and narrow the airway lumen.
- 19. CHRONIC BRONCHITIS PATHOGENESIS In contrast to emphysema, chronic bronchitis is associated with a relatively undamaged pulmonary capillary bed. • The body responds by decreasing ventilation and increasing cardiac output. • This V/Q mismatch results in rapid circulation in a poorly ventilated lung, leading to hypoxemia and polycythemia. • Eventually, hypercapnia and respiratory acidosis develop, leading to pulmonary artery vasoconstriction and cor pulmonale. • With the ensuing hypoxemia, polycythemia, and increased CO2 retention, these patients have signs of right heart failure and are known as "blue bloaters."
- 21. SYMPTOMS • Patients typically present with a combination of signs and symptoms of chronic bronchitis, emphysema, and reactive airway disease. Symptoms include the following: • Cough, usually worse in the mornings and productive of a small amount of colorless sputum • Breathlessness: The most significant symptom, but usually does not occur until the sixth decade of life • Wheezing: May occur in some patients, particularly during exertion and exacerbations
- 22. PHYSICAL EXAMINATION Relatively poor sensitivity in mild-to-moderate COPD • In severe COPD: • Cyanosis, visible in the lips and nail beds • Peripheral edema • Tachypnea and respiratory distress with simple activities • Use of accessory respiratory muscles and paradoxical indrawing of lower intercostal spaces (Hoover sign) • Sitting in the characteristic “tripod” position to facilitate the actions of the sternocleidomastoid, scalene, and intercostal muscles for a prolonged expiratory phase. • Elevated jugular venous pulse (JVP)
- 23. PHYSICAL EXAMINATION • Thoracic examination reveals the following: • Hyperinflation (barrel chest) • Wheezing – Frequently heard on forced and unforced expiration • Diffusely decreased breath sounds • Hyperresonance on percussion • Prolonged expiration • Coarse crackles beginning with inspiration in some cases
- 24. PHYSICAL EXAMINATION- PREDOMINANT CHRONIC BRONCHITIS (BLUE BLOATERS) • Patients may be obese • Frequent cough and expectoration are typical • Use of accessory muscles of respiration is common • Coarse rhonchi and wheezing may be heard on auscultation • Patients may have signs of right heart failure (ie, cor pulmonale), such as edema and cyanosis
- 25. PHYSICAL EXAMINATION- PREDOMINANT EMPHYSEMA (PINK PUFFERS) • Patients may be very thin with a barrel chest • Patients typically have little or no cough or expectoration • Breathing may be assisted by pursed lips and use of accessory respiratory muscles; patients may adopt the tripod sitting position • The chest may be hyperresonant, and wheezing may be heard • Heart sounds are very distant
- 27. • current evidence demonstrates that most patients have elements of both chronic bronchitis and emphysema and that the physical examination does not reliably differentiate the two entities.
- 28. INVESTIGATIONS • Post-bronchodilator spirometry- FEV1/FVC < 70%, with normal TLC. • The diffusing capacity may be reduced • Arterial blood gases and oximetry may demonstrate resting or exertional hypoxemia. • Elevated hematocrit suggests the presence of chronic hypoxemia, • α1AT assay
- 29. INVESTIGATIONS • Chest X Ray –Obvious bullae, paucity of parenchymal markings, or hyperlucency on suggests the presence of emphysema. –Increased lung volumes and flattening of the diaphragm suggest hyperinflation • Chest computed tomography (CT) scan –current definitive test for establishing the presence or absence of emphysema, the pattern of emphysema, and the presence of significant disease involving medium and large airways –It also enables the discovery of coexisting interstitial lung disease and bronchiectasis, –help determine the possible value of surgical therapy
- 30. INVESTIGATIONS-OTHERS • Hematocrit – Patients with polycythemia (hematocrit greater than 52% in men or 47% in women) • Serum potassium – Diuretics, beta-adrenergic agonists, and theophylline • Measure AAT in all patients younger than 40 years, in those with a family history of emphysema at an early age, or with emphysematous changes in a nonsmoker • Sputum evaluation will show a transformation from mucoid in stable chronic bronchitis to purulent in acute exacerbations • Pulse oximetry. • Electrocardiography can help establish that hypoxia is not resulting in cardiac ischemia and that the underlying cause of respiratory difficulty is not cardiac in nature • Right-sided heart catheterization can confirm pulmonary artery hypertension and
- 31. COPD SEVERITY ASSESSMENT • GOLD Spirometric calculation-population based method. COPD severity categories based on respiratory symptoms. • Modified Medical Research Council Dyspnea Scale (mMRC ) or COPD Assessment Test (CAT) and annual frequency of COPD exacerbations. • CAT is an 8-item COPD health status measure with Likert scale responses for questions about cough, phlegm, chest tightness, dyspnea on one flight of stairs, limitation in home activities, confidence in leaving the home, sleep and energy. Range of total score is 0–40.
- 35. THE REFINED ABCD ASSESSMENT TOOL
- 36. TREATMENT- STABLE PHASE COPD • TREATMENT GOALS –Provide symptomatic relief –Reduce future risk –Improve exercise tolerance, overall health status –Prevent and treat exacerbation AND complications –Reduce morbidity and mortality • Response to therapy should be assessed, and decisions should be made whether or not to continue or alter treatment.
- 37. TREATMENT- STABLE PHASE COPD • Some interventions have been demonstrated to improve survival of patients with COPD Smoking cessation. Oxygen therapy in chronically hypoxemic patients. Lung volume reduction surgery (LVRS) in selected patients with emphysema. Use of triple therapy significantly lowers mortality compared with dual bronchodilation
- 38. PHARMACOTHERAPY • General management: • smoking cessation –nicotine replacement therapy available as gum, transdermal patch, lozenge, inhaler, and nasal spray; –bupropion; and –varenicline, a nicotinic acid receptor agonist/antagonist. • Annual influenza vaccination • One-off pneumococcal vaccination every 5 years.
- 39. PHARMACOTHERAPY • Bronchodilator therapy: Short-acting Beta2-agonist (SABA) or short-acting muscarinic antagonist (SAMA) is first-line treatment. For patients who remain breathless or have exacerbations despite using short- acting bronchodilators the next step is determined by the FEV1. • FEV1 > 50% (Stage I & II): Long-acting beta2-agonist (LABA), for example salmeterol, or: Long-acting muscarinic antagonist (LAMA), for example tiotropium. • FEV1 < 50% (Stage III & IV): LABA + high-dose inhaled corticosteroid (ICS) in a combination inhaler, or: LAMA.
- 44. LTOT • Patients who receive LTOT should breathe supplementary oxygen for at least 15 hours a day. Oxygen concentrators are used to provide a fixed supply for LTOT. • Assess patients for LTOT if any of the following: • Oxygen saturations less than or equal to 92% on room air • Very severe airflow obstruction (FEV1 < 30% predicted). Assessment should be 'considered' for patients with severe airflow obstruction (FEV1 30-49% predicted). • Patients with a PaO2 of less than 55 mm Hg, a PaO2 of less than 59 mm Hg with evidence of polycythemia, or cor pulmonale. • Reevaluate these patients 1-3 months after initiating therapy.
- 45. OTHERS • Theophylline • PDE4 Inhibitors • `A1AT Augmentation Therapy • Mucolytics
- 46. NONPHARMACOLOGIC THERAPIES • Pulmonary Rehabilitation • Lung Volume Reduction Surgery • Lung Transplantation
- 47. EXACERBATIONS OF COPD • Exacerbations are a prominent feature of the natural history of COPD. • Exacerbations are episodic acute worsening of respiratory symptoms, including increased dyspnea, cough, wheezing, and/ or change in the amount and character of sputum. • The three cardinal symptoms of COPD exacerbation include –increases in dyspnea, –Increase in sputum volume, and –Increase in sputum purulence.
- 48. EXACERBATIONS OF COPD • Though symptoms of COPD exacerbations usually last for about 7 to 10 days, the patient may not fully recover for several weeks to months. • Patients with severe (FEV1 <50% predicted) or very severe airflow obstruction (FEV1 <30% predicted) on average have 1–3 episodes per year.
- 49. EXACERBATIONS OF COPD- RISK FACTORS • The strongest single predictor of exacerbations is a history of a previous exacerbation • Duration of COPD, • History of antibiotic or theophylline use, • Advanced age, • Increased ratio of pulmonary artery to aorta cross-sectional dimension, • Comorbid conditions (e.g., chronic heart failure, diabetes mellitus, GORD etc.). • Patients with increased sputum production, productive cough, and an elevated blood eosinophil count (>0.34 x 109 cells/L)
- 50. EXACERBATIONS OF COPD- RISK FACTORS • Environmental pollution, temperature, and pulmonary embolism are also known exacerbation triggers. • Chest Infections –Bacteria frequently implicated include Haemophilus influenzae(most common), Streptococcus pneumoniae and Moraxella catarrhalis. In addition, Mycoplasma pneumoniae or Chlamydia pneumoniae are found in 5–10% of exacerbations. –Viral respiratory infections are present in approximately one-third of COPD exacerbations. rhinovirus being the most important pathogen. • In 20–35%, no specific precipitant can be identified.
- 51. SEVERITY OF EXARCEBATION SEVERITY OF EXARCEBATION TYPE OF EXARCEBATION CHARACTERISTICS SEVERE TYPE 1 Increased dyspnea, sputum volume and sputum purulence MODERATE TYPE 2 Any 2 of the above 3 cardinal symptoms MILD TYPE 3 Any 1 of the above 3 cardinal symptoms and 1 or more of the following minor symptoms or signs - Cough - Wheezing - Fever without an obvious source - Upper respiratory tract infection in the past 5 days - Respiratory rate increase >20% over baseline - Heart rate increase >20% over baseline
- 52. TREATMENT - COPD EXARCEBATION • The goal of therapy when treating a COPD exacerbation are – The recovery to baseline clinical status. – Prevention of future exarcebations. – Prevention of hospitalization or reduction in hospital stay, – Prevention of acute respiratory failure and death,
- 53. INDICATIONS FOR ADMISSION FOR ACUTE EXARCEBATION. • Failure of outpatient treatment • Marked increase in dyspnea • Altered mental status • Increase in hypoxemia or hypercapnia • Onset of new physical signs (eg cyanosis, periphaeral edema) • Presence of serious comorbidities (eg heart failure or new onset arrhythmias)) • Freque nt exarcebations • Older age • Inability to tolerate oral medications such as antibiotics or steroids
- 54. INDICATIONS FOR ICU ADMISSION • Severe dyspnea that responds inadequately to initial emergency therapy. • Changes in mental status.(confusion, lethargy, coma) • Persistent or worsening hypoxemia (PaO2 <5.3Kpa, 4OmmHg) and severe/worsening resiratory acidosis (PH <7.25) despite supplemental oxygen and noninvasive ventilation. • Need for invasive Mechanical ventilation. • Hemodynamic instability-need for vasopressors.
- 55. TREATMENT - COPD EXARCEBATION • Bronchodilators Mild exacerbations- use of short-acting beta2-agonists (SABA), with or without short-acting anticholinergics Moderate-to-severe exacerbations- SABA+ systemic corticosteroid. Continued use of long-acting bronchodilators throughout the exacerbation or start as soon as possible before discharge. • Controlled oxygen therapy. Start at 24-28%. AIM: 88-92%. Adjust according to ABG: AIM: PaO2 8kpa with rise of PaCo2 <1.5kpa
- 56. TREATMENT - COPD EXARCEBATION • Steroids Give prednisolone 30 mg daily for 7-14 days. Prolonged courses offer no additional benefit. • Antibiotics Give antibiotics only if sputum is purulent or there are clinical signs of pneumonia. Improves FEV1, shortens duration of hospitalization and recovery time, reduce the risk of early relapse. • NIV should be considered within the first 60 minutes of hospital arrival in all patients with an acute exacerbation of COPD in whom a respiratory acidosis
- 58. REFERENCES • Adeloye D, Basquill C, Papana A, et al. An estimate of the prevalence of COPD in Africa: a systematic analysis. COPD 2015;12:71-81. 10.3109/15412555.2014.908834 • Ozoh OB, Awokola T, Bust SA. Medical student’s knowledge about the management of COPD in Nigeria. Int J Tuber Lung Dis 2014; 18: 117–21. • American Journal of Respiratory and Critical Care Medicine 2012;185:A6029 Chronic Obstructive Pulmonary Disease In Sub Saharan Africa: A Systematic Review Lydia J. Finney , Johanna Feary , Stephen B. Gordon , Jo Leonardi Bee , Kevin Mortimer , https://doi.org/10.1164/ajrccm-conference.2012.185.1_MeetingAbstracts.A6029 • Oxford handbook of clinical Medicine. 10th edition P184-187; P160;P812-814 • Summarizing the 2021 Updated GOLD Guidelines for COPD, US Pharmacist. US Pharm. 2021;46(7):30-35.
- 59. • venturi masks • examples of drugs and classes • HYPOXEAMIA DEFINITION • nasal prongs non rebreayhable • side eefect of steroids • NORMAL PAO2 PCO2 AND OTHERS • COR PULMONALE SX. Cyanosis • Polycythaemia • Peripheral oedema • Raised jugular venous pressure • ASTHMA VS COPD • RELEVANT ANATOMY • read oxford • when is theophylline indicated and other drugs • respiratory failure types • ARACHIDIONIC ACID PATHWAY FOR BROCHOCONSTRICTION
- 61. • Features suggesting a diagnosis of COPD • • Persistent dyspnoea on effort with cough and wheeze • • History of smoking or exposure to other risk factors • • Slow progression • • Abnormal post bronchodilator spirometry • Features that suggest the presence of asthma • • Young age at onset • • Diurnal or day-to-day variability and seasonal variation • • Presence of atopy and/or allergic rhinitis • • Significant bronchodilator responsiveness • Additional considerations in the diagnosis of asthma and COPD • • Asthma and COPD may co-exist, and distinguishing them may be difficult • • Asthmatics who smoke may have an accelerated decline in lung function • • COPD patients may have a raised eosinophil count and bronchodilator responsiveness
- 62. • AIRFLOW OBSTRUCTION • Airflow limitation, also known as airflow obstruction, is typically determined for clinical purposes by spirometry, which involves forced expiratory maneuvers after the subject has inhaled to total lung capacity. Key parameters obtained from spirometry include the volume of air exhaled within the first second of the forced expiratory maneuver (FEV1) and the total volume of air exhaled during the entire spirometric maneuver (forced vital capacity [FVC]). Patients with airflow obstruction related to COPD have a chronically reduced ratio of FEV1/FVC. In contrast to asthma, the reduced FEV1 in COPD seldom shows large responses to inhaled bronchodilators, although improvements up to 15% are common.
- 63. • HYPERINFLATION • In COPD there is often “air trapping” (increased residual volume and increased ratio of residual volume to total lung capacity) and progressive hyperinflation (increased total lung capacity) late in the disease
- 64. • hyperinflation can push the diaphragm into a flattened position with a number of adverse effects. – First, by decreasing the zone of apposition between the diaphragm and the abdominal wall, positive abdominal pressure during inspiration is not applied as effectively to the chest wall, impairing inspiration. – Second, because the muscle fibers of the flattened diaphragm are shorter than those of a more noRmally curved diaphragm, they are less capable of generating inspiratory pressures than normal. – Third, the flattened diaphragm must generate greater tension to develop the transpulmonary pressure required to produce tidal breathing. – Fourth, the thoracic cage is distended beyond its normal resting volume, the inspiratory muscles must do work to further inflate as recoil function is lost.
- 65. GAS EXCHANGE • The partial pressure of oxygen in arterial blood Pao2 usually remains near normal until the FEV1 is decreased to ~50% of predicted, and even much lower FEV1 values can be associated with a normal Pao2, at least at rest. • PaCO2 is usually elevated when FEV1 is <25% of predicted. • Non-uniform ventilation and ventilation-perfusion mismatching are characteristic of COPD, reflecting the heterogeneous nature of the disease process within the airways and lung parenchyma.
- 66. • Lung volume reduction surgery in selected patients: –If PCO2 ≥ 7.4 –Severe limitation of exercise capacity despite maximal therapy. –Predominant upper lobe emphysema. – Persistent symptoms despite a period of pulmonary rehabilitation
Notas del editor
- The conducting zone of the respiratory system includes the organs and structures not directly involved in gas exchange. The gas exchange occurs in the respiratory zone.
- Bronchial Tree Primary bronchi – right and left branches of the trachea that enter the lungs Secondary bronchi – branches of the primary that enter each lobe of the lungs Tertiary bronchi – more branches of the secondary bronchi Bronchioles – smallest branches within the lungs Alveolar ducts – microscopic branches of the bronchioles Alveoli – terminal air sacs where gas exchange takes place (anatomy resembles a bunch of grapes) Surfactant – mixture of lipoproteins that reduces the attraction between water molecules in the alveoli; it prevents collapse of the alveoli
- Increase frequency of bronchodilator use and consider giving via a nebuliser(Salbutamol 5mg/4h and Ipratropium 500mcg/6h) Acutely ill patients: 94-98%. Patients at risk of hypercapnia (e.g. COPD patients): 88-92%. Oxygen should be reduced in stable patients with satisfactory oxygen saturation.
- Replace with inhaled steroids after improvement.