Presentation1, artifact and pitfalls of the knee, hip and ankle joints.
•Descargar como PPTX, PDF•
4 recomendaciones•1,548 vistas

Health&Medicine

Recomendados
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Presentation1, artifact and pitfalls of the knee, hip and ankle joints.
Similar a Presentation1, artifact and pitfalls of the knee, hip and ankle joints. (20)
Más de Abdellah Nazeer
Más de Abdellah Nazeer (20)
Último
Último (20)
Presentation1, artifact and pitfalls of the knee, hip and ankle joints.
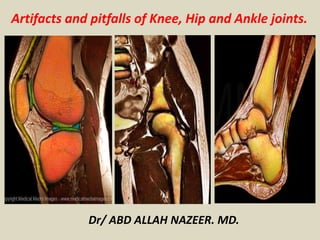
- 1. Artifacts and pitfalls of Knee, Hip and Ankle joints. Dr/ ABD ALLAH NAZEER. MD.
- 2. Knee Joint: Meniscofemoral ligaments extends from the posterior horn of lateral meniscus to the lateral aspect of medial femoral condyle. Consists of ligament of Humphrey, anterior to the posterior cruciate ligament (PLC), and ligament of Wrisberg, posterior to the PLC and larger Vahey and colleagues identified meniscofemoral ligaments in 50% of 109 MR scans. In 39% they causes appearance of pseudotear in sagittal images. The interposition of a thin layer of fat between the posterior horn of the lateral meniscus and ligament meniscofemoral simulates tear. It is necessary to follow these normal structures on subsequent images to do not interpret as meniscal injury
- 3. Coronal proton-density fast spin-echo (TR 3580 ms, TE 44 ms): example of Wrisberg meniscofemoral ligament (black arrow heads).
- 4. b. Transverse ligament The transverse ligament is identified on MR images of the knee as a hypointense structure that connects the anterior horn of the lateral and medial meniscus. It was detected by Sintzoff and colleagues in 78% of cases. The space filled by fat between the ligament and the meniscus can simulate tear in the anterior horn of lateral meniscus,but can also be seen in medial meniscus. Following sequential images confirm it is not a tear, but transverse ligament. Furthermore, isolated lesions in the anterior horn of the lateral meniscus are uncommon, detected in 6% of cases.
- 5. Proton-density fast spin-echo (TR 3580 ms, TE 44 ms) sequential images confirm it is just the transverse ligament.
- 7. A and B proton-density fast spin-echo (TR 3580 ms, TE 44 ms). Transverse ligament simulating tear in the anterior horn of lateral meniscus (white arrow in A). Ligament transverse showed in axial images (black arrowhead in B).
- 8. MENISCAL PITFALLS: -Speckled anterior horn of the lateral meniscus: it may mimic a meniscal tear of the anterior horn but it is a normal variant created by the insertion of fibers of the ACL into the meniscus. -Transverse intermeniscal ligament: it may mimic a meniscal tear of the anterior horn of both menisci. -Menisco-meniscal and menisco-femoral ligaments may also simulate a tear of the posterior horn of the lateral meniscus, but the continuity of these structures in consecutive slices on MRI helps to make an accurate diagnosis.
- 13. Popliteus tendon The popliteus tendon and its sheath stands between the articular capsule and lateral meniscus to insert in the lateral femoral condyle. The tendon sheath appears as a structure of high signal and can be interpreted as a lesion in the posterior horn of the lateral meniscus, especially in the presence of joint fluid (Herman and Beltran 775-81;Muglia et al. 161-66). Anatomical knowledge and following of images are essential for correct diagnosis.
- 14. Proton-density fast spin-echo (TR 3180 ms, TE 50 ms) sagittal image shows the popliteus tendon (short arrow). The direction of the pseudo tear (long arrow) is the same of the tendon.
- 16. Speckled anterior horn Frequently is observed a speckled appearance of the anterior horn of lateral meniscus, possibly occurs by the insertion of the anterior cruciate ligament. This aspect is found in approximately 56% of cases and should not be confused with injury
- 17. Sagittal proton-density fast spin-echo (A) and T1 weight images (B): speckled anterior horn of lateral meniscus (arrows).
- 19. Chondrocalcinosis The presence of meniscal calcification is a form manifestation of calcium pyrophosphate dihydrate of the deposition disease. This calcification may cause high signal in the meniscus and mimic tear. On the other hand, may obscure a real lesion. It is recommended radiography correlation. Meniscal ossicles are uncommon, often incidental, findings on radiography and cross-sectional imaging of the knee. The ossicle should follow bone marrow signal on all sequences: T1: hyperintense T2FS/STIR: hypointense
- 20. a-d Lateral knee joint of a 44-year-old man with single focal hyaline cartilage chondrocalcinosis at the medial tibia. (a) Coronal 3D T1-weighted gradient-echo sequence, (b) coronal reformation of 3D DESS, and a (c) coronal proton density-weighted FSE image showing a focal hypointensity in the hyaline cartilage (arrows). (d) PA radiograph showing a corresponding hyperdense calcification in this area (arrow). Calcium-containing crystal can clearly be depicted on gradient echo sequences (a, b) in comparison to FSE sequence (c)
- 23. Meniscal flounce Meniscal flounce is a normal find present in 0.2% of cases which is associated with ligamentous laxity. The meniscus has a folded appearance and it possibly has no clinical significance. A ring meniscus is a very rare anatomical variant of the lateral meniscus of the knee. The inner margin of a ring meniscus on coronal images can easily be mistaken for a bucket-handle meniscal tear displaced into the intercondylar space, so it is usually diagnosed during arthroscopy.
- 26. Ring meniscus. Coronal intermediate-weighted MR image (TR/TE, 3300/36) shows central triangular low-signal- intensity structure mimicking bucket-handle tear (arrowhead). Structure has smooth triangular appearance and remainder of lateral meniscus was normal without evidence of tear or loss of meniscal volume.
- 27. Oblique meniscomeniscal ligament. Midsagittal fat-suppressed T2-weighted MR image (A) (TR/TE, 3750/68) shows linear low-signal-intensity structure (arrowhead) within intercondylar notch mimicking displaced meniscal fragment. Axial fat-suppressed T2-weighted MR image
- 28. Wrisberg rip” and pseudotear.
- 29. Meniscocapsular recess resembling tear.
- 30. Fluid-filled popliteus recess mimicking a tear of the posterolateral meniscus. Coronal FS T2-WI (A) shows a fluid-filled popliteus recess mimicking a peripheral tear of the posterolateral meniscus (white arrow). Analysis of the axial (B) and sagittal images (C) as well as the typical location allows correct diagnosis of a pseudotear.
- 31. Pseudo jumper knee: The patellar tendinopathy is associated with sports activities and is also known as jumper's knee. This condition presents with pain, swelling and functional limitation. In studies of MRI appears as striates thickening and increased signal in the tendon. However, often there is a high signal and slightly increased thickness at eighter or both ends in asymptomatic patients. Schweitzer and colleagues found focal areas of signal in 74% and intratendon signal was also seen commonly in the inferior aspect of the tendon (32%). Therefore, it is important to always relate to clinical information. Furthermore, increased thickness of tendon tends to be higher in jumper's knee.
- 32. Sagittal proton-density fast spin-echo (A) and T1 weight images (B): observe the small areas of increased signal in A and B (arrows).
- 33. Pseudo iliotibial band friction The iliotibial band friction syndrome is a clinical condition associated with intense physical activity in which occurs friction of the iliotibial tract over the lateral femoral condyle. Joint fluid that accumulates in the lateral recess of the knee can simulate the iliotibial tract syndrome. However, in the syndrome fluid accumulates on both sides of the tract and there are alterations in the iliotibial tract, such as sign changes and thickening. Liquid only on the medial side of the iliotibial tract indicate joint fluid.
- 34. Coronal proton-density fast spin-echo (TR 2620 ms, TE 40 ms) shows a normal iliotibial tract (arrow) and fluid in the lateral recess (arrowheads). It should not be mistaken to iliotibial band friction syndrome.
- 35. Anterior cruciate ligament cyst Anterior cruciate ligament (ACL) is the most common site of cystic lesion inside the knee joint The cysts are most common in males and have an incidence up to 0.44% in MRI studies. Patients usually complain about painless and restriction of movement. Is important to mention that trauma may cause local changes that lead to cyst formation. These cysts eventually may simulate rupture of the ACL. Meanwhile, the clinical lesion is different and it presents with a drumstick appearance on sagittal images and cystic on coronal or axial images.
- 36. Mucoid degeneration of the anterior cruciate ligament (ACL). On sagittal T1-WI (A), the ACL is of intermediate signal intensity and the ligamentous structure has disappeared. On sagittal FS T2-WI (B), the ACL has a striated pattern with interspersed intact ligamentous fibers, resembling a celery stalk (white arrow). There is also an intraosseous ganglion cyst at the tibial insertion of the ACL (black arrowhead). Axial FS T2-WI (C) demonstrates the intermediate signal of the ACL with interspersed intact ligamentous fibers (black arrow).
- 37. A bipartite patella in which secondary or accessory ossification centers of the patella fail to unite with the main osseous body of the patella is a normal developmental variant seen in 2% of the population. The most common type is a bipartite fragment involving the superolateral pole of the patella (75%). A bipartite patella can be distinguished on MRI from a fracture by the location of the bipartite segment, presence of well-corticated margins to the accessory segment, and typical integrity of underlying articular cartilage of the patella overlying the incompletely united accessory ossification center. Marrow edema at the interface of the bipartite segment is suggestive of micromotion at the synchondrosis, and defects in the normally intact articular cartilage may be features associated with symptomatic anterior knee pain. The dorsal defect of the patella is a further variant thought to be related to normal enchondral ossification involving the superolateral patella, which is seen in up to 1% of individuals
- 38. Bipartite patella. Axial fat-suppressed T2- weighted MR image (TR/TE, 3500/70) shows osseous fragment (arrowhead) involving superolateral patella with low-signal-intensity interface with patella. There is osseous edema on both sides of interface. Overlying articular cartilage is intact but shows focal signal change. Dorsal defect of patella. Axial fat- suppressed T2-weighted MR image (TR/TE, 3350/60) shows focal osseous defect (arrowhead) involving lateral facet of patella. Overlying cartilage is intact.
- 41. DISTAL FEMORAL GROOVES: They are normal notches in the trochlear surface and the medial and lateral femoral condyles and they should not be mistaken from impaction fractures.
- 42. Prominent insertion of the medial gastrocnemius onto the posterior aspect of the distal femoral metaphysis:
- 43. We show an example of a normal cortical spur in the internal tibial metaphysis.
- 44. FEMORAL PSEUDO-OSTEOCHONDRITIS: It is seen in children and teenagers. It refers to the irregularity of the ossification of the femoral condyles but, unlike the osteochondritis dissecans, these femoral condylar irregularities will have intact overlying cartilage and marrow edema is usually absent.
- 45. BONE MARROW: Hematopoietic bone marrow hyperplasia: low signal on T1WI and high signal on T2WI in the femoral metaphysis with epiphysis spared. Its differential diagnosis includes pathological bone marrow infiltration.
- 47. 45-year-old woman with hematopoietic marrow involvement of distal femur. A, Proton density image (TR/TE, 2300/15) shows heterogeneous marrow signal intensity changes involving distal femoral diametaphysis (arrowheads). Signal intensity changes do not cross physeal scar, and there are areas of interspersed fat within involved area. Axial fat-suppressed T2-weighted MR image (TR/TE, 3550/70) shows mild patchy hyperintensity of distal femoral marrow (arrowheads).
- 48. Bone marrow reconversion. Sagittal T1-WI (A) and FS T2-WI (B) shows bone marrow of intermediate signal intensity in the distal femoral diaphysis and proximal tibia in a middle-aged heavy smoking female patient.
- 49. Hip Synovial herniation pits Femoral fibrocystic changes may occur anteriorly at the junction of the head and neck . Recently, it has been speculated that these fibrocystic changes are related to repetitive impingement of the femoral neck and the anterosuperior acetabulum.
- 50. Herniation pit.
- 51. Radial PD WI of the right hip (arthro-MRI). Synovial herniation pit (red circle).
- 52. Os acetabuli The origin of bone fragments along the acetabular rim, called os acetabuli or os acetabulare . It has been attributed that some acetabula may have secondary ossification centers, and this should not be confused to fractures or ossification of the labrum and/or acetabulum, secondary to the cam type femoroacetabular impingement syndrome. Acetabular ossification may also appear after trauma, rickets, osteomyelitis, and osteochondritis dissecans .
- 54. Transverse acetabular ligament The acetabulum closely covers the femoral head, with the exception of its anteroinferior aspect, where there is an absence of bone and cartilage. This anteroinferior aspect of the acetabulum is crossed by the transverse acetabular ligament (TAL). Also, the TAL forms a complete ring around the acetabulum. The transverse ligament attaches to the acetabular rim anteriorly and posteriorly and to the ligamentum teres femoris. The junction between TAL and the acetabular labrum occurs a normal cleft that can be mistaken for an acetabular labral tear .
- 56. Perilabral recess Similar to the shoulder, the hip joint capsule attaches to the osseous rim of the acetabulum, sustained posteriorly by the ischiofemoral ligament and anteriorly by the iliofemoral and pubofemoral ligaments. Between the medial joint capsule and the acetabular labrum may exist a normal sulcus, so called perilabral recess .
- 57. Joint recess.
- 58. Supra-acetabular fossa The supra-acetabular fossa is small cavity in the superior, weight- bearing region of the acetabulum. It is usually filled with fibrous tissue, covered by cartilage and should be easy distinguishable from an osteochondral lesion.
- 59. Superior anterior labrum rupture.
- 60. Tubular acetabular intraosseous contrast tracking: Intraosseous track of contrast material in MR arthrography may be found in hips at approximately 15%. These tracks are linear and blind-ending structures that originate from the acetabular fossa at or near its margin with the acetabular cartilage . This finding is thought to be an unlikely source of hip pain.
- 62. 52-yearold woman who underwent bilateral hip imaging for suspected unilateral acetabular labral tears. Consecutive axial fat-suppressed 3D fast low angle shot (TR/TE, 48/11; flip angle, 40°) MR arthrographic images in cranial–caudal sequence show asymptomatic hip. A, Anterior tubular track (A) originates from margin (arrow) of acetabular fossa close to articular cartilage (arrowhead). B, Anterior tubular track (A) originates from margin of acetabular fossa. Posterior tubular track (P) originates from junction (arrow) of posterior margin of acetabular fossa and articular cartilage. C, Posterior tubular track (P) originates from junction of posterior margin of acetabular fossa and articular cartilage. D, Dilatation of blind end of posterior tubular track known as clubbing phenomenon (asterisk) is evident
- 63. Stellate crease The stellate crease, also improperly called stellate lesion, is another anatomic variant and represents a uncovered area within the acetabular articular surface above the anterosuperior margin of the acetabulum . On MR imaging, the stellate crease can appear irregular and could be mistaken for an osteochondral lesion.
- 65. Iliopsoas bursa The iliopsoas bursa is located subjacent to the iliopsoas myotendinous junction and a communication either congenital or acquired may occur (15% of people). Obviously, a normal iliopsoas bursa is usually collapsed and not visible on MR imaging, although distention with a small amount of fluid may also be observed in asymptomatic hips. In MR arthrography, intra-articular contrast material may be easy seen.
- 66. Iliopsoas bursa in a patient with synovitis.
- 67. Accessory iliacus tendon: The accessory iliacus tendon is a common anatomy variation, seen in 66% of MR arthrograms, which may simulate iliopsoas tendon abnormality. On MR transversal images, accessory iliacus tendon is represented by a small tendon paralleling the iliopsoas major tendon, separated by a fat plane. Therefore, visualization of liquid instead of fat is prone to tendinopathy. Also, tendon pathology is frequently associated with iliopsoas bursitis.
- 69. Ankle: Pseudodefect of talar dome Pseudodefect of talar dome is a normal groove in the posterior aspect of the talus for the passage of the posterior talofibular ligament and should not be confused with osteochondral fracture. This is a very common finding, observed in most MRI studies. In a series involving 40 patients, the pseudodefect was found in 96% of cases. In a few cases that had been examined both ankles, the groove was present in 86%. It is seen on MRI images as an irregular area of low signal in the posterior aspect of the talus. This characteristic location and the absence of other findings make easy to recognize this pitfall and differentiates it from osteochondral injury.
- 70. 7-year-old boy with history of nonspecific nontraumatic foot and ankle pain. A, Coronal T1-weighted (A), coronal intermediate-weighted fat-suppressed (B), sagittal STIR (C), and sagittal T1-weighted (D) MR images show relatively prominent notch (arrows). Notch is filled by trace synovial fluid and partially contains articular cartilage. No subjacent subcortical osteosclerosis, ankle joint effusion, osteochondral lesions elsewhere in ankle, or bone marrow edema were present. No loose osteochondral body or other derangements were present on radiographs (not shown).
- 71. 48-year-old woman with nontraumatic nonspecific ankle pain. D, Coronal intermediate-weighted (A), coronal intermediate-weighted fat-suppressed (B), sagittal STIR (C), and sagittal T1-weighted (D) MR images show relatively prominent notch (arrows). Notch is filled by trace synovial fluid. No subjacent subcortical osteosclerosis, ankle joint effusion, osteochondral lesions elsewhere in ankle, or bone marrow edema were present. No loose osteochondral body or other derangements were present on radiographs (not shown).
- 72. T1-weighted sagittal image: osteochondral fracture. There is a bone defect of talar dome with low sign intensity (arrow).
- 73. Appearance variations in ligaments and tendons Tendons and ligaments usually appear as homogeneous and hypointense structures on MRI images. This appearance indicates that there are no injuries and that these structures must be intact. Nevertheless, they may have a different aspect in some cases, usually because of fatty tissue between the ligament and tendon fibers, which does not necessarily indicate injury. The following ligaments are often seen as a striated structure, with heterogeneous signal: posterior talofibular, posterior tibiofibular, talocalcaneal and anterior tibiotalar (deep deltoid). This appearance should not be confused with injury. Normal posterior talofibular ligament with irregular and frayed superior edge was found by Noto and colleagues in 13 of 30 cases. Similarly, the posterior tibial tendon can easily simulate injury, since it has multiple insertions, providing a complex image appearance
- 74. Normal striated signal intensity pattern in deep deltoid ligament (arrow).
- 75. Coronal proton-density fast spin-echo (A) and T1 weight images (B) shows inhomogeneity of posterior talofibular ligament (arrowheads).
- 76. Accessory bones and sesamoids First of all is necessary to differentiate sesamoids from accessories bones, which can be a source of confusion. Sesamoids are located in the intimacy of the tendon, in places where they change course and over bony prominences. There is a sesamoid bone in the peroneus longus tendon proximal to its entrance into the cuboid sulcus (os peroneum). Another one can be found in the posterior tibial tendon proximal to its insertion into the navicular tuberosity. Accessory bones are secondary ossification centers that can be found in various locations of the foot and ankle. They rarely have clinical significance. However, the navicular bone (especially type 2) may eventually present with symptoms, for example. The os trigonum is found in about 10% of population and also may present with pain (os trigonum syndrome). They are commonly found in imaging studies and should not be confused with fracture. They have regular appearance, rounded shape and typical location. There is no difficulty to make this differentiation.
- 77. T1-weighted sagittal image shows an os trigonum (arrow).
- 78. Axial T1-weighted MR images shows peroneus quartus muscle belly (white arrow) and its tendon inserting in calcaneal bone (black arrow).
- 79. T1-weighted sagittal image shows focal low signal intensity irregularly (arrow) and should not be confused with osteochondral fracture.
- 80. Accessory muscles It is not uncommon to find accessory muscles in the ankle. In most cases they do not have clinical significance and are often incidentally found. In a few instances may present as a palpable mass, simulating a tumor, or may cause compression of local structures(64, 68). The peroneus quartus muscle is found in up to 17-22% of the population. It originates in the lateral and distal aspect of the fibula, positioned posteromedial to peroneal tendons, and attachment is variable, including the calcaneus and cuboid bones and the peroneal tendons. Be careful not to confuse the peroneus quartus muscle with low-lying peroneus brevis muscle belly. The insertion site is different for each one. The peroneus quartus muscle is generally asymptomatic. However, eventually may associate with dislocation and injury in the peroneal tendons. The accessory soleus muscle is rarely found and it is usually asymptomatic. However, there are some cases in the literature that this anomalous muscle presents as soft tissue mass or with local pain. Another muscle described in the ankle is the flexor digitorum longus accessories, encountered in 6% of asymptomatic individuals, but may be associated with tarsal tunnel syndrome.
- 81. Axial T1-weighted MR image shows low position of the peroneus brevis muscle (arrow).
- 82. Accessory soleus with a fleshy insertion. Axial (9a) and sagittal (9b) T1-weighted MR images of a 43 y/o female with ankle pain. An accessory soleus (arrows) with a fleshy insertion on the medial calcaneus (red arrowhead) is apparent.
- 83. Peroneus quartus (peroneal calcaneal variant). Axial (11a), and sagittal (11b) T1-weighted MR images show a fleshy accessory peroneus quartus muscle (arrows) coursing posterior the peroneal longus (PL) and peroneus brevis (PB) tendons and inserting onto the retrotrochlear eminence of the calcaneus (asterisk).
- 84. Peroneocalcaneus internus (PCI). Sequential axial T2-weighted MR images in a 73 y/o female patient with heel pain, numbness, and a clinical diagnosis of tarsal tunnel syndrome. At the distal tibia, the PCI muscle (red) interdigitates with the flexor hallucis longus muscle (blue). Distally, the PCI tendon (red arrow) is seen lateral to the flexor hallucis longus tendon (blue arrow). Both tendons are highlighted by tenosynovial fluid (asterisk) posterior to the talus and sustentaculum tali. The neurovascular bundle is seen medial to these tendons (yellow outline). The PCI tendon inserts on the medial calcaneus below the sustentaculum tali (red arrowhead).
- 85. Thank You.