Presentation1.pptx, congenital abnormality of the sellar and para sellar regions
•Descargar como PPTX, PDF•
25 recomendaciones•2,170 vistas

This document discusses congenital abnormalities of the sellar and parasellar regions. It begins by stating that the aim is to show the embryological correlations of the pituitary gland and how knowledge of these correlations allows for understanding of congenital abnormalities in these regions. It then discusses MRI as the preferred imaging technique for evaluating these types of pathologies. The document goes on to provide examples of various congenital abnormalities that can be seen in the sellar and parasellar regions through MRI images, including transsphenoidal encephalocele, hypoplastic pituitary gland, ectopic posterior pituitary, hypothalamic hamartoma, infundibular hypoplasia, Rathke's cleft cyst, cranioph

Recomendados
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (20)
Similar a Presentation1.pptx, congenital abnormality of the sellar and para sellar regions
Similar a Presentation1.pptx, congenital abnormality of the sellar and para sellar regions (20)
Más de Abdellah Nazeer
Más de Abdellah Nazeer (20)
Último
Último (20)
Presentation1.pptx, congenital abnormality of the sellar and para sellar regions
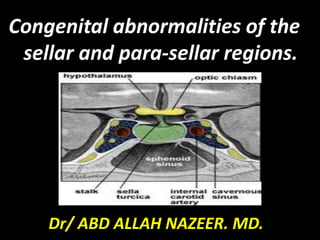
- 1. Congenital abnormalities of the sellar and para-sellar regions. Dr/ ABD ALLAH NAZEER. MD.
- 2. Aim of the lecture. To show the embryological correlations of the pituitary gland with adjacent structures which allow knowledge of interpretation of the sellar and para- sellar congenital abnormalities. Also to show imaging appearance of the congenital diseases of the sellar and para-sellar regions. .
- 11. Technique: MRI is the examination of choice for sellar and para-sellar pathologies due to its superior soft tissue contrast, multiplanar capability and lack of ionizing radiation. In addition, MRI also provides useful information about the relationship of the gland with adjacent anatomical structures and helps to plan medical or surgical strategy. MRI techniques in diagnosing pituitary lesions have witnessed a rapid evolution, ranging from non-contrast MRI in late 1980s to contrast-enhanced MRI in mid-1990s. Recently, a variety of advanced MR techniques have been evolved which are particularly helpful in evaluating specific cases. These include 3D volumetric analysis of pituitary volume, high-resolution MR imaging at 3 Tesla (T) for evaluating pituitary stalk.
- 12. The aim of MR imaging is to obtain a high- spatial-resolution image with a reasonable signal to noise ratio. It is important to identify the gland separate from the lesion if possible. Initially, pre-contrast T1- and T2-weighted spin echo coronal and sagittal sections are acquired using a small FOV (20×25 cm), thin slices (2-3 mm), and high-resolution matrix (256×512). Both the dynamic and routine post-contrast images and delayed scanning after 30-60 minutes may be combined in one study for optimum imaging.
- 13. Parameters. TR TE FLIP NXA SLICE MATRIX FOV PHASE OVERSAMPLE GAP 3000-4000 110 130 4 2-3mm 256x512 100-130 R> L 100% 10%
- 19. Transsphenoidal encephalocele. MRI and CT images of transsphenoidal encephalocele.
- 22. Markedly hypoplastic pituitary with absent bright spot. (A) Sagittal non- contrast T1- weighted and (B) contrast-enhanced T1-weighted imaging shows almost complete absence of the gland with an associated shallow sella (arrowheads). The upper infundibulum is present but the characteristic high T1-weighted signal is not seen on non contrast imaging.
- 23. Anterior pituitary aplasia and posterior pituitary ectopia. No anterior pituitary gland identified with a thin infundibulum.
- 28. Sagittal MRI of the hypothalamic−pituitary axis. The pituitary (lower arrow) is small and scalloped. There is absence of the normal posterior pituitary and stalk in and above the pituitary fossa, and an ectopic posterior pituitary bright spot where the infundibulum normally is (upper arrow). Ectopic neurohypophysis with small pituitary gland.
- 29. Ectopic posterior pituitary gland and the pituitary gland is hypoplastic (arrowhead).
- 40. Congenital disorder. Development of the adenohypophysis.
- 43. Rathke,s Cleft Cyst: CT : •75% hypodense •25% iso/hyperdense •Ca++ rare •May be difficult to differentiate from other benign cysts or craniopharyngioma.
- 50. Sagittal T1W, Fluid suppressed T2W and post contrast T1W images showing craniopharyngioma in child.
- 54. Miscellaneous.
- 56. Dermoid cyst.
- 57. Right para-and supra-sellar dermoid cyst.
- 61. THANK YOU.