Peripheral Nervous System Therapy
•
8 recomendaciones•1,930 vistas

PTP&M009 PTM of Peripheral Nervous System trauma and disea…

Recomendados
Recomendados
Más contenido relacionado
Destacado
Destacado (12)
Último
Último (20)
Peripheral Nervous System Therapy
- 1. PHYSICAL THERAPY PRINCIPALS & METHODS PTP&M:009 Revision: 01 Page: 1 of 19 PHYSICAL THERAPY MANAGEMENT OF PERIPHERAL NERVOUS SYSTEM TRAUMA AND DISEASE RELATED PATIENTS NOTICE: This specification, and the subject matter disclosed therein, embody proprietary information which is the confidential property of Mullsons Health & Wellness, which shall be copied, reproduced, disclosed to others, published, and could be used in whole or part, for any purpose, without the express advance written permission of a duly authorized agent of the Company. This specification is subject to recall by Mullsons Health & Wellness at any time. PHYSICAL THERAPY MANAGEMENT OF PERIPHERAL NERVOUS SYSTEM TRAUMA AND DISEASE RELATED PATIENTS SPEC. BY: Abdulrehman S. Mulla DATE: 04/09/2009 REVISION HISTORY REV. DESCRIPTION CN No. BY DATE 01 Initial Release PT009 ASM 04/09/2009 MEDICINE:IT’S A NOBLE PROFESSION, IT SERVES HUMANITY 1/19
- 2. PHYSICAL THERAPY PRINCIPALS & METHODS PTP&M:009 Revision: 01 Page: 2 of 19 PHYSICAL THERAPY MANAGEMENT OF PERIPHERAL NERVOUS SYSTEM TRAUMA AND DISEASE RELATED PATIENTS NOTICE: This specification, and the subject matter disclosed therein, embody proprietary information which is the confidential property of Mullsons Health & Wellness, which shall be copied, reproduced, disclosed to others, published, and could be used in whole or part, for any purpose, without the express advance written permission of a duly authorized agent of the Company. This specification is subject to recall by Mullsons Health & Wellness at any time. TABLE OF CONTENTS PAGE 1.0 PERIPHERAL NERVOUS SYSTEM: 3 1.1 PERIPHERAL NERVOUS SYSTEM DISORDERS: 7 1.1.1 CAUSES OF PERIPHERAL NERVOUS SYSTEM DISORDERS: 7 1.1.2 CLINICAL CLUES TO CAUSES OF PERIPHERAL NERVOUS SYSTEM* DISORDERS: 8 1.3 TREATMENT: 8 1.4 TYPES OF PERIPHERAL NERVOUS SYSTEM DISORDERS: 9 1.4.1 COMPRESSIVE NEUROPATHY: 9 1.4.2 SCIATICA: 10 1.4.3 PERIPHERAL NEUROPATHY: 11 A. CAUSES OF PERIPHERAL NEUROPATHY: 11 1.4.4 SPINAL INFECTIONS: 12 A. SYMPTOMS; 12 B. DIAGNOSIS: 12 C. TREATMENT OPTIONS: 12 1.4.5 SPINAL MENINGITIS: 14 1.2 NEUROLOGY PHYSICAL THERAPY: 15 1.2.1 MEDICALLY-BASED FITNESS WORKS WITH A BROAD RANGE OF CONDITIONS INCLUDING: 16 1.2.2 NERVE DISORDERS SPECIFIC PROGRAMMING: 17 A. PHYSICAL THERAPY FOR SPINAL NERVE DISORDERS: 17 B. VESTIBULAR THERAPY: 18 MEDICINE:IT’S A NOBLE PROFESSION, IT SERVES HUMANITY 2/19
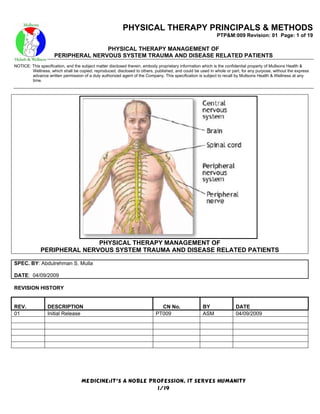
- 3. PHYSICAL THERAPY PRINCIPALS & METHODS PTP&M:009 Revision: 01 Page: 3 of 19 PHYSICAL THERAPY MANAGEMENT OF PERIPHERAL NERVOUS SYSTEM TRAUMA AND DISEASE RELATED PATIENTS NOTICE: This specification, and the subject matter disclosed therein, embody proprietary information which is the confidential property of Mullsons Health & Wellness, which shall be copied, reproduced, disclosed to others, published, and could be used in whole or part, for any purpose, without the express advance written permission of a duly authorized agent of the Company. This specification is subject to recall by Mullsons Health & Wellness at any time. PERIPHERAL NERVOUS SYSTEM TRAUMA AND DISEASE: 1.0 PERIPHERAL NERVOUS SYSTEM: MEDICINE:IT’S A NOBLE PROFESSION, IT SERVES HUMANITY 3/19
- 4. PHYSICAL THERAPY PRINCIPALS & METHODS PTP&M:009 Revision: 01 Page: 4 of 19 PHYSICAL THERAPY MANAGEMENT OF PERIPHERAL NERVOUS SYSTEM TRAUMA AND DISEASE RELATED PATIENTS NOTICE: This specification, and the subject matter disclosed therein, embody proprietary information which is the confidential property of Mullsons Health & Wellness, which shall be copied, reproduced, disclosed to others, published, and could be used in whole or part, for any purpose, without the express advance written permission of a duly authorized agent of the Company. This specification is subject to recall by Mullsons Health & Wellness at any time. The human peripheral system has two types of nerves based on location: Spinal nerves (31 pairs) connect with the spinal cord and innervate most areas of the body. Cranial nerves (12 pairs) connect vital organs directly to the brain. SPINAL NERVES: MEDICINE:IT’S A NOBLE PROFESSION, IT SERVES HUMANITY 4/19
- 5. PHYSICAL THERAPY PRINCIPALS & METHODS PTP&M:009 Revision: 01 Page: 5 of 19 PHYSICAL THERAPY MANAGEMENT OF PERIPHERAL NERVOUS SYSTEM TRAUMA AND DISEASE RELATED PATIENTS NOTICE: This specification, and the subject matter disclosed therein, embody proprietary information which is the confidential property of Mullsons Health & Wellness, which shall be copied, reproduced, disclosed to others, published, and could be used in whole or part, for any purpose, without the express advance written permission of a duly authorized agent of the Company. This specification is subject to recall by Mullsons Health & Wellness at any time. I Olfactory II Optic III Oculomotor IV Trochlear V Trigeminal VI Abducens VII Facial VIII Auditory IX Glossopharyngeal X Vagus XI Accessory XII Hypoglassal CRANIAL NERVES MEDICINE:IT’S A NOBLE PROFESSION, IT SERVES HUMANITY 5/19
- 6. PHYSICAL THERAPY PRINCIPALS & METHODS PTP&M:009 Revision: 01 Page: 6 of 19 PHYSICAL THERAPY MANAGEMENT OF PERIPHERAL NERVOUS SYSTEM TRAUMA AND DISEASE RELATED PATIENTS NOTICE: This specification, and the subject matter disclosed therein, embody proprietary information which is the confidential property of Mullsons Health & Wellness, which shall be copied, reproduced, disclosed to others, published, and could be used in whole or part, for any purpose, without the express advance written permission of a duly authorized agent of the Company. This specification is subject to recall by Mullsons Health & Wellness at any time. Spinal and cranial nerves can also be classified on the basis of function: The somatic nerves relay sensory information from receptors in the skin and muscles and motor commands to skeletal muscles (voluntary control). The autonomic nerves sends signals to and from smooth muscles, internal organs (visceral functions) cardiac muscle, and glands (involuntary control). There are two types of autonomic nerves the parasympathetic and sympathetic nerves: Parasympathetic nerves tend to slow down body activity when the body is not under stress. They originate in the brain and the sacral region of the spinal cord. Their ganglia are in walls of organs. They promote housekeeping responses, such as digestion. Sympathetic nerves increase overall body activity during times of stress, excitement, or danger. They also call on the hormone epinephrine to increase the "fight-flight" response. They originate in the thoracic and lumbar regions of the spinal cord. Their ganglia are near the spinal cord. Most organs receive input from both sympathetic and parasympathetic nerves, usually with opposite effects on the organ. Most organs are continually receiving both sympathetic and parasympathetic stimulation. For example, sympathetic nerves signal the heart to speed up MEDICINE:IT’S A NOBLE PROFESSION, IT SERVES HUMANITY 6/19
- 7. PHYSICAL THERAPY PRINCIPALS & METHODS PTP&M:009 Revision: 01 Page: 7 of 19 PHYSICAL THERAPY MANAGEMENT OF PERIPHERAL NERVOUS SYSTEM TRAUMA AND DISEASE RELATED PATIENTS NOTICE: This specification, and the subject matter disclosed therein, embody proprietary information which is the confidential property of Mullsons Health & Wellness, which shall be copied, reproduced, disclosed to others, published, and could be used in whole or part, for any purpose, without the express advance written permission of a duly authorized agent of the Company. This specification is subject to recall by Mullsons Health & Wellness at any time. 1.1 PERIPHERAL NERVOUS SYSTEM DISORDERS: 1.1.1 CAUSES OF PERIPHERAL NERVOUS SYSTEM DISORDERS: SITE TYPE EXAMPLES Spinal muscular atrophy types I–IV Inherited Polio, infections by coxsackievirus and other enteroviruses (rare) Acquired, acute Amyotrophic lateral sclerosis, paraneoplastic syndrome, postpolio syndrome, Motor neuron* Acquired, chronic progressive bulbar palsy Nerve root Acquired Herniated disk, infections, metastatic cancer, neurofibroma, trauma Acute brachial neuritis, diabetes mellitus, hematoma, local tumors (eg, schwannoma), metastatic cancer, neurofibromatosis (rare), traction during Plexus Acquired birth, severe trauma Hereditary adult-onset neuropathies, hereditary sensorimotor neuropathies, Peripheral nerve Hereditary hereditary sensory and autonomic neuropathies Hepatitis C, HIV infection, Lyme disease, syphilis In undeveloped nations: Infectious Diphtheria, parasites Chronic inflammatory demyelinating polyradiculoneuropathy, Guillain-Barré Inflammatory syndrome and variants, vasculitis Amyloidosis, diabetes mellitus, dysproteinemic neuropathy, ethanol with undernutrition (particularly deficiency of B vitamins), ICU neuropathy, Metabolic leukodystrophies (rare), renal insufficiency Botulism in infants, congenital myasthenia (very rare), Eaton-Lambert Neuromuscular syndrome, myasthenia gravis, toxic neuromuscular junction disorders (eg, junction — due to nerve gas) Distal muscular dystrophy (late distal hereditary myopathy; rare), Duchenne's muscular dystrophy and related dystrophies, fascioscapulohumeral muscular dystrophy, limb-girdle muscular dystrophy, Muscle fibre Dystrophies oculopharyngeal dystrophy (rare) Channelopathies Familial periodic paralysis, myotonia congenita (Thomsen's disease), (myotonic) myotonic dystrophy (Steinert's disease) Central core disease, centronuclear myopathy, nemaline myopathy (very Congenital rare) Acromegaly, Cushing's syndrome, diabetes mellitus, hypothyroidism, Endocrine thyrotoxic myopathy Inflammatory Infection (viral more than bacterial), polymyositis and dermatomyositis Acid maltase deficiency, carnitine deficiency, glycogen storage and lipid Metabolic storage diseases (rare) Upper motor neuron disorders (e.g. spinal muscular atrophies) technically involve the CNS because the cell body of the motor neuron is located in the spinal cord. MEDICINE:IT’S A NOBLE PROFESSION, IT SERVES HUMANITY 7/19
- 8. PHYSICAL THERAPY PRINCIPALS & METHODS PTP&M:009 Revision: 01 Page: 8 of 19 PHYSICAL THERAPY MANAGEMENT OF PERIPHERAL NERVOUS SYSTEM TRAUMA AND DISEASE RELATED PATIENTS NOTICE: This specification, and the subject matter disclosed therein, embody proprietary information which is the confidential property of Mullsons Health & Wellness, which shall be copied, reproduced, disclosed to others, published, and could be used in whole or part, for any purpose, without the express advance written permission of a duly authorized agent of the Company. This specification is subject to recall by Mullsons Health & Wellness at any time. 1.1.2 CLINICAL CLUES TO CAUSES OF PERIPHERAL NERVOUS SYSTEM* DISORDERS: Finding Cause to Consider Diffuse disorders (e.g., toxic-metabolic, hereditary, infectious, or inflammatory disorders; most immune- Symmetric, diffuse deficits mediated disorders) Unilateral deficits Focal disorders (e.g., mononeuropathies, plexopathies) Deficits localized to one or more peripheral nervous system structures (e.g., nerve root, spinal nerve, nerve plexus, single peripheral nerve, multiple mononeuropathy) Lesion in a peripheral nervous system structure Stocking-glove distribution of deficits Diffuse peripheral polyneuropathies, possibly axonal Disproportionate weakness of proximal muscles Diffuse muscle dysfunction, as occurs in diffuse (eg, difficulty walking stairs, combing hair) with myopathies Possibly disorders of the neuromuscular no sensory deficits junction if the eyes are affected Chronic, progressive weakness affecting mostly distal muscles with no sensory deficits Motor neuron disorders Buzzing and tingling with motor weakness and decreased reflexes Demyelination Profound motor weakness with minimal atrophy Acquired demyelinating polyneuropathy Deficient pain and temperature sensation; weakness proportional to atrophy; disproportionately mild reflex abnormalities, usually more distal than proximal Vascular disorders (e.g. vasculitis, ischemia) 1.3 TREATMENT: Treatment of underlying disorder Supportive care, often by multidisciplinary team Treatment is directed at the underlying disorder when possible. Otherwise, treatment is supportive. A multidisciplinary team approach helps patients cope with progressive neurologic disability: Physical therapists may help patients maintain muscle function. Occupational therapists can recommend adaptive braces and walking devices to help with activities of daily living. Speech and language therapists may provide alternative communication devices. If pharyngeal weakness develops, nurses feed patients with extreme care. A gastroenterologist may recommend percutaneous endoscopic gastrostomy. If respiratory weakness develops, pulmonary specialists are needed to determine whether noninvasive respiratory support (e.g. bilevel positive airway pressure) or tracheostomy with full ventilatory support should be used. Early in fatal disorders, health care practitioners must talk frankly with patients, family members, and caregivers to determine the level of intervention acceptable (see Medicolegal Issues: Advance Directives). These decisions should be reviewed and confirmed at various stages of the disorder. MEDICINE:IT’S A NOBLE PROFESSION, IT SERVES HUMANITY 8/19
- 9. PHYSICAL THERAPY PRINCIPALS & METHODS PTP&M:009 Revision: 01 Page: 9 of 19 PHYSICAL THERAPY MANAGEMENT OF PERIPHERAL NERVOUS SYSTEM TRAUMA AND DISEASE RELATED PATIENTS NOTICE: This specification, and the subject matter disclosed therein, embody proprietary information which is the confidential property of Mullsons Health & Wellness, which shall be copied, reproduced, disclosed to others, published, and could be used in whole or part, for any purpose, without the express advance written permission of a duly authorized agent of the Company. This specification is subject to recall by Mullsons Health & Wellness at any time. 1.4 TYPES OF PERIPHERAL NERVOUS SYSTEM DISORDERS: Compressive neuropathy Spinal infections Sciatica Spinal meningitis Peripheral neuropathy 1.4.1 COMPRESSIVE NEUROPATHY: Compressive Neuropathy (nu-rop-ah-thee) occurs when nerves in the spine are compressed. This disorder often affects older people. The nerves that exit the spinal canal become trapped, compressed, and swollen. Foraminal stenosis can be extremely painful and debilitating. The effects may temporarily damage or permanently destroy nerves. Foraminal stenosis (foe-ray-min-al sten-oh-sis, e.g. spinal stenosis) is an example of a compressive neuropathy. A slipped, herniated (her-knee-ate-ed), ruptured or bulging disc may cause nerve compression. Nerves may also be compressed or even displaced by the growth of bone spurs. A compressive neuropathy may cause pain to radiate into one or both buttocks, down the legs below the knees and may be felt in the ankles and feet. Pain may be accompanied by sensations of tingling, numbness, and weakness. These types of symptoms are generally referred to as "sciatica." MEDICINE:IT’S A NOBLE PROFESSION, IT SERVES HUMANITY 9/19
- 10. PHYSICAL THERAPY PRINCIPALS & METHODS PTP&M:009 Revision: 01 Page: 10 of 19 PHYSICAL THERAPY MANAGEMENT OF PERIPHERAL NERVOUS SYSTEM TRAUMA AND DISEASE RELATED PATIENTS NOTICE: This specification, and the subject matter disclosed therein, embody proprietary information which is the confidential property of Mullsons Health & Wellness, which shall be copied, reproduced, disclosed to others, published, and could be used in whole or part, for any purpose, without the express advance written permission of a duly authorized agent of the Company. This specification is subject to recall by Mullsons Health & Wellness at any time. 1.4.2 SCIATICA: Sciatica (sy-attic-ka) is a symptom of a compressive neuropathy involving one or several of the lower spinal nerves that make up the sciatic nerve. It is a common ailment named for the sciatic nerve, which is a collection of smaller nerves descending from the spine and joining together to resemble a cable. The spinal nerves come together in the pelvis to form the sciatic nerve. The sciatic nerve then travels down through each buttock into the legs. At certain points, such as in the posterior thighs, nerves branch off from the main sciatic cable. This is why sciatic pain may be felt in various muscles of the leg. SCIATIC NERVE The spinal cord ends in the lumbar area and continues through the vertebral canal as spinal nerves. Because of its resemblance to a horse's tail, the collection of these nerves at the end of the spinal cord is called the cauda equina. These nerves send and receive messages to and from the lower limbs and pelvic organs. A direct blow to the sciatic nerve in the leg may occur when falling down. This may injure the sciatic nerve. The force from falling down could initiate bleeding around the nerve and cause nerve compression and pain. If a disc or bone spur protrudes into the spinal nerves that become the sciatic nerve, the problem may become severe. A bone spur could displace a spinal nerve creating intense pain. Fortunately there are non-surgical treatments available to help reduce inflammation and associated pain. These treatments include medication and steroid injections. When nonsurgical treatment fails and, depending on the patient's symptomatology, surgery may be considered. In some cases a surgical procedure called a laminotomy (lamb-in-ah-toe-me) may be performed to give the surgeon greater access to the offending intervertebral disc. Removal of the disc is called a discectomy or microdiscectomy (under magnification). MEDICINE:IT’S A NOBLE PROFESSION, IT SERVES HUMANITY 10/19
- 11. PHYSICAL THERAPY PRINCIPALS & METHODS PTP&M:009 Revision: 01 Page: 11 of 19 PHYSICAL THERAPY MANAGEMENT OF PERIPHERAL NERVOUS SYSTEM TRAUMA AND DISEASE RELATED PATIENTS NOTICE: This specification, and the subject matter disclosed therein, embody proprietary information which is the confidential property of Mullsons Health & Wellness, which shall be copied, reproduced, disclosed to others, published, and could be used in whole or part, for any purpose, without the express advance written permission of a duly authorized agent of the Company. This specification is subject to recall by Mullsons Health & Wellness at any time. 1.4.3 PERIPHERAL NEUROPATHY: Peripheral Neuropathy is a degenerative, toxic, or nutritional condition affecting the nerves that branch into the body's extremities such as the arms, hands, legs, and feet. Diabetes or even certain drugs can cause peripheral neuropathy. The disease causes the peripheral or distant parts of nerves to shrink. Eventually the affected nerves may deteriorate to the point that the nerves can no longer carry impulses. Sensory (feeling) and motor (movement) function may be lost. Symptoms may include burning or a feeling of pins and needles, numbness in the toes or fingers, and weakness when gripping an object or while walking. Medication may help to slow the effects of peripheral neuropathy but may not cure or stops its progression. Peripheral Neuropathy may be generally categorized by the type of nerve that is damaged (e.g., motor, sensory or autonomic). However, this condition may also be categorized by where it occurs in the body. For instance, nerve damage that occurs in only one area of the body is called mononeuropathy. If the damage is present in multiple areas of the body it is referred to as polyneuropathy. When the condition is present on both sides of the body the condition is called symmetric neuropathy. Peripheral Neuropathy may also be categorized by cause. For example: Diabetic Neuropathy (the result of diabetes), nutritional neuropathy (the result of a nutritional deficit), etc. When a cause cannot be identified the condition is called idiopathic neuropathy. A. CAUSES OF PERIPHERAL NEUROPATHY: Diabetic peripheral neuropathy Prolonged use of crutches Charcot-Marie-Tooth syndrome Staying in one position for too long Uremia Tumor AIDs Intraneural hemorrhage Nutritional deficiencies Cold exposure Nerve entrapment Radiation exposure Nerve compression Certain medicines Carpal tunnel syndrome Certain toxic substances Trauma Atherosclerosis Penetrating injuries Systemic lupus erythematosus Contusions Scleroderma Fractures Sarcoidosis Dislocated bones Rheumatoid arthritis Polyarteritis nodosa MEDICINE:IT’S A NOBLE PROFESSION, IT SERVES HUMANITY 11/19
- 12. PHYSICAL THERAPY PRINCIPALS & METHODS PTP&M:009 Revision: 01 Page: 12 of 19 PHYSICAL THERAPY MANAGEMENT OF PERIPHERAL NERVOUS SYSTEM TRAUMA AND DISEASE RELATED PATIENTS NOTICE: This specification, and the subject matter disclosed therein, embody proprietary information which is the confidential property of Mullsons Health & Wellness, which shall be copied, reproduced, disclosed to others, published, and could be used in whole or part, for any purpose, without the express advance written permission of a duly authorized agent of the Company. This specification is subject to recall by Mullsons Health & Wellness at any time. 1.4.4 SPINAL INFECTIONS: Spinal Infections are rare and painful. Immediate medical attention is always necessary. If an infection is not detected and treated, the effected area swells and causes pain to radiate into adjoining tissue. A spinal infection may cause permanent injury or take root in the epidural cavity (ep-e-do-ral). This cavity is a fatty area near nerve roots and provides space for an infection or abscess. Epidural cavities are found in the cervical (sir-ve-kal), thoracic (thor-as-ick), and lumbar (lum-bar) spine. An MRI may be performed to confirm a spinal infection. Nonsurgical treatment may include intravenous or oral antibiotics combined with bed rest. In some cases surgical intervention may be necessary to eradicate the infection. A. SYMPTOMS; The symptoms of a spinal infection include fever, chills, headache, neck stiffness, pain, wound redness and tenderness, and wound drainage. In some cases patients may notice new weakness, numbness, or tingling sensations in the arms and/ or legs. The symptoms may be very severe, or they may be very subtle in some cases. Your doctor may order a series of tests to look for an infection if one is suspected. B. DIAGNOSIS: These tests may include plain x-rays, computerized tomography (CT or CAT) scans, or MRI scans. In some cases further, specialized testing is required when the diagnosis is still in question. These include nuclear medicine bone scans and nuclear medicine tagged white blood cell scans. Your doctor will want to obtain cultures to determine the type of bacteria or fungus that is causing the infection. Blood cultures are often obtained to screen for evidence of infection. Cultures of your wound or the area of infection may be taken. In cases of deep infections of the vertebrae (bone) or the intervertebral disk, a needle culture may be required. This is often done with x-ray guidance with local anesthetic medication given at the needle entry site. Your doctor may also order additional blood tests to screen for signs of an infection. These tests include a white blood cell (WBC) count, c-reactive protein (CRP) and an erythrocyte sedimentation rate (ESR). These values may be slightly elevated after an operation, but usually return to normal values within a few weeks. Abnormal elevation may represent a sign of infection. C. TREATMENT OPTIONS: The nonsurgical management of spinal infections consists of antibiotic or antifungal medications. The type and the duration of the treatment depends on the severity of the infection and the organism causing the infection. Antibiotics or antifungal medications may be necessary intravenously (IV) and/ or orally. The duration of the treatment typically ranges from as short as 7-10 days, to as long as 6-12 weeks. You may need to have a special intravenous line, called a central line, placed for a long course of antibiotics. This allows, in some cases, for the medications to be administered at home with the assistance of a home health care agency or a visiting nurse. Your doctor may recommend using a brace to support the spine until healing occurs and to help with the pain. Surgery may be required for many postoperative infections to wash away much of the bacteria and infected tissue. In addition, surgery may be required in cases where there is evidence of instability of the spine as a result of the infection. In cases in which there is severe weakness as a result of a spinal infection, surgery may be required to relieve the pressure on the spinal cord caused by the infection. MEDICINE:IT’S A NOBLE PROFESSION, IT SERVES HUMANITY 12/19
- 13. PHYSICAL THERAPY PRINCIPALS & METHODS PTP&M:009 Revision: 01 Page: 13 of 19 PHYSICAL THERAPY MANAGEMENT OF PERIPHERAL NERVOUS SYSTEM TRAUMA AND DISEASE RELATED PATIENTS NOTICE: This specification, and the subject matter disclosed therein, embody proprietary information which is the confidential property of Mullsons Health & Wellness, which shall be copied, reproduced, disclosed to others, published, and could be used in whole or part, for any purpose, without the express advance written permission of a duly authorized agent of the Company. This specification is subject to recall by Mullsons Health & Wellness at any time. The surgical options to treat spinal infections range from simply washing out the wound and re-closing to more extensive debridements and removal of infected tissues. In some cases it is not possible to close the wound at the time of surgery, and a packing dressing is left in place. This is often changed two to three times a day until the wound heals over a period of several weeks. A combination of surgery and long term antibiotics are often required to completely treat some spinal infections. During the course of your treatment, your doctor may follow your white blood cell (WBC) count along with your C-reactive protein (CRP) or erythrocyte sedimentation rate (ESR) as markers of the response to therapy. These levels may be elevated in the early period after surgery, but they usually return to normal within a few weeks. Re-elevation or failure of these values to return to normal after treatment may indicate recurrent or residual infection. MEDICINE:IT’S A NOBLE PROFESSION, IT SERVES HUMANITY 13/19
- 14. PHYSICAL THERAPY PRINCIPALS & METHODS PTP&M:009 Revision: 01 Page: 14 of 19 PHYSICAL THERAPY MANAGEMENT OF PERIPHERAL NERVOUS SYSTEM TRAUMA AND DISEASE RELATED PATIENTS NOTICE: This specification, and the subject matter disclosed therein, embody proprietary information which is the confidential property of Mullsons Health & Wellness, which shall be copied, reproduced, disclosed to others, published, and could be used in whole or part, for any purpose, without the express advance written permission of a duly authorized agent of the Company. This specification is subject to recall by Mullsons Health & Wellness at any time. 1.4.5 SPINAL MENINGITIS: Spinal Meningitis (men-in-ji-tis) is an infection that causes inflammation of the membranes in the brain and spinal cord. This is a serious disease and may require hospitalization. Treatment includes intravenous or oral antibiotics combined with bed rest. Symptoms may include fever, weakness, pain that radiates from the spine, muscle spasm, sensitivity to touch, decreased spinal flexibility, fatigue, sweating, and weight loss. When a child is affected, symptoms may include his refusal to stand or sit because it is painful. Increased backache may be an indication in older children and adults. Neck pain and sensitivity to light are common symptoms. The organs of the central nervous system (brain and spinal cord) are covered by 3 connective tissue layers collectively called the meninges. Consisting of the pia mater (closest to the CNS structures), the arachnoid and the dura mater (farthest from the CNS), the meninges also support blood vessels and contain cerebrospinal fluid. These are the structures involved in meningitis, an inflammation of the meninges, which, if severe, may become encephalitis, an inflammation of the brain. MEDICINE:IT’S A NOBLE PROFESSION, IT SERVES HUMANITY 14/19
- 15. PHYSICAL THERAPY PRINCIPALS & METHODS PTP&M:009 Revision: 01 Page: 15 of 19 PHYSICAL THERAPY MANAGEMENT OF PERIPHERAL NERVOUS SYSTEM TRAUMA AND DISEASE RELATED PATIENTS NOTICE: This specification, and the subject matter disclosed therein, embody proprietary information which is the confidential property of Mullsons Health & Wellness, which shall be copied, reproduced, disclosed to others, published, and could be used in whole or part, for any purpose, without the express advance written permission of a duly authorized agent of the Company. This specification is subject to recall by Mullsons Health & Wellness at any time. 1.2 NEUROLOGY PHYSICAL THERAPY: High velocity accidents and sporting incidents carry a risk of causing a spinal cord injury (SCI), a serious but uncommon condition which can also be caused by ischaemia, infections or tumours. Younger people are the biggest group likely to suffer this injury due to their risky pursuits but it can occur in someone of any age, road accidents accounting for the greatest proportion. Due to the complex nature of the condition a multi-disciplinary approach is essential, involving several health care professionals, to facilitate the highest degree of independence in the patient. Paraplegia and quadriplegia are the terms used for the resulting conditions. The emergency medical situation is dealt with first, keeping the person alive and ensuring their breathing is clear. Once in the hospital the doctors test the patient to find out what spinal level has been damaged as this determines much of the physiotherapy and medical management. Low spinal injury such as in the lumbar area will not have consequences for the patient's ability to breathe and they will have good arm and trunk power to work on independence. A high thoracic or cervical injury paralyses some of the rib muscles, reducing the ability for spontaneous breathing and limiting arm power, making rehabilitation much more difficult. Assessment of the patient's respiratory status is the initial concern of the physiotherapist, often in the intensive care unit. The physiotherapist will attempt to encourage the patient to expand their lungs, deep breathe and cough any secretions up to clear their chest. Paralysis of the lower trunk can reduce propulsive force and thereby the effectiveness of coughing, a process which the physiotherapist helps by stabilizing the lower abdomen during attempted coughing. Suction may be needed in severe cases and coughing can be promoted by using a cough assist machine. Transfer of the patient to the ward follows the intensive care period and by now they should be medically stable. The patient may undergo spinal fusion surgery with internal fixation to stabilized the fractured segments, avoiding the need to wait for the typical healing period of the spine which is three months. Now the early rehabilitation of the patient can begin, with the physiotherapist checking closely on the patient's respiratory ability, exercising the non-paralyzed areas for strength and mobility and undertaking regular passive movements to the paralyzed limbs to keep and to increase the ranges of motion. If the spine is unstable, which it often is in spinal trauma resulting in paraplegia, a spinal surgeon will stabilized the spine, usually with instrumentation and bone grafting. This allows the patient to start their rehabilitation without the long wait for the spinal fractures to heal naturally. Initial physiotherapy management is to monitor the respiratory status, encourage active movement of unaffected areas and perform passive movements of paralyzed body parts to retain and improve the ranges of motion which will be required later for independence. Positioning the spinal cord injured patient is very important for safety of the fracture site, for pressure care of the skin and for preparing the patients body for the positions they will need to live as independently as possible. The frog position is one of the postures the physiotherapist will place the patient in, with the hips bent up and the knees placed out to the side so the soles of the feet are touching. The patient will need this position to manage their sitting balance to lean forward to move the legs, to self-catheterise and to get to their feet to put on socks and manage foot care. The next stage of rehabilitation involves getting the patient up into a wheelchair but initially the patient's blood pressure can react badly by dropping strongly so they are sat gradually up in bed and then transferred to a chair with the back on a slope and with elevating leg rests. Tolerance of being upright is gradually extended and sitting balance practiced on the edge of a plinth, with the physiotherapist closely monitoring any poor trunk control. The physiotherapist will move on to strengthening and to teaching transfers into a wheelchair and once the patient has developed reasonable sitting balance and accustomed themselves to transfers and being out in a wheelchair for MEDICINE:IT’S A NOBLE PROFESSION, IT SERVES HUMANITY 15/19
- 16. PHYSICAL THERAPY PRINCIPALS & METHODS PTP&M:009 Revision: 01 Page: 16 of 19 PHYSICAL THERAPY MANAGEMENT OF PERIPHERAL NERVOUS SYSTEM TRAUMA AND DISEASE RELATED PATIENTS NOTICE: This specification, and the subject matter disclosed therein, embody proprietary information which is the confidential property of Mullsons Health & Wellness, which shall be copied, reproduced, disclosed to others, published, and could be used in whole or part, for any purpose, without the express advance written permission of a duly authorized agent of the Company. This specification is subject to recall by Mullsons Health & Wellness at any time. periods of time it is appropriate for them to be transferred to a spinal injuries unit where they can receive specialized help from a multi-disciplinary team for the many aspects of their condition they need to master to be as independent as possible. 1.2.1 MEDICALLY-BASED FITNESS WORKS WITH A BROAD RANGE OF CONDITIONS INCLUDING: Balance Deficits Stroke Nerve disorders Polyneuropathies Multiple Sclerosis Dizziness Brain Injury Vestibular Spinal Cord Injury Coordination Peripheral Neuropathy MBF Physical Therapy restores physical function and improves the efficiency of movement by addressing the individual client's functional limitations. Our therapists treat the functional deficits you have in order to improve your daily life. MBF takes an active approach in treatment, and problem solves long-term solutions with individualized programs treating the whole body. Our care is transferable to daily life activities making clients happier, healthier, and more independent. MBF Physical Therapists excel in treatment of the neurological system. MBF has been working with individuals with neurological impairments since 1996. There have been three Master's and two PhD degrees earned through research performed at Medically-Based Fitness. We utilize outcome based research and the most current research to guide our programming. We have concrete outcomes that improve the active approach to therapy in order to advance the life of every client. MEDICINE:IT’S A NOBLE PROFESSION, IT SERVES HUMANITY 16/19
- 17. PHYSICAL THERAPY PRINCIPALS & METHODS PTP&M:009 Revision: 01 Page: 17 of 19 PHYSICAL THERAPY MANAGEMENT OF PERIPHERAL NERVOUS SYSTEM TRAUMA AND DISEASE RELATED PATIENTS NOTICE: This specification, and the subject matter disclosed therein, embody proprietary information which is the confidential property of Mullsons Health & Wellness, which shall be copied, reproduced, disclosed to others, published, and could be used in whole or part, for any purpose, without the express advance written permission of a duly authorized agent of the Company. This specification is subject to recall by Mullsons Health & Wellness at any time. 1.2.2 NERVE DISORDERS SPECIFIC PROGRAMMING: MBF is a resource to individuals with NERVE DISORDERS disease for information, education, and treatment. MBF Physical Therapy enables an individual to compensate for the changes brought on by NERVE DISORDERS disease by providing programming that is specifically developed for individuals limited by this disease. The treatment will include therapies to address immediate limitations and develop long term programs to promote functional independence through the disease process. The physical therapy includes education for the individuals and their caregivers. A. PHYSICAL THERAPY FOR SPINAL NERVE DISORDERS: Balance and Coordination Immobility Gait Trunk and Joint Mobility Weakness Motor Programming Pain Fatigue Posture MEDICINE:IT’S A NOBLE PROFESSION, IT SERVES HUMANITY 17/19
- 18. PHYSICAL THERAPY PRINCIPALS & METHODS PTP&M:009 Revision: 01 Page: 18 of 19 PHYSICAL THERAPY MANAGEMENT OF PERIPHERAL NERVOUS SYSTEM TRAUMA AND DISEASE RELATED PATIENTS NOTICE: This specification, and the subject matter disclosed therein, embody proprietary information which is the confidential property of Mullsons Health & Wellness, which shall be copied, reproduced, disclosed to others, published, and could be used in whole or part, for any purpose, without the express advance written permission of a duly authorized agent of the Company. This specification is subject to recall by Mullsons Health & Wellness at any time. B. VESTIBULAR THERAPY: Vestibular therapy encompasses a multitude of diagnoses and subjective complaints. A vestibular therapist can effectively treat patients who are dizzy for reasons including: Benign Paroxysmal Positional Vertigo (BPPV); Fall risk, Vestibular Hypofunction or Injury; Deconditioning, Meniere's Disease; Neurological injuries such as MS, TBI, or concussion with resultant complaints of General imbalance, dizziness. The treatment received will vary depending on the etiology/cause of the patient's complaints. Some patients are seen only a few visits and are symptom-free very quickly. Other patients have to be seen for a longer duration of time, but will also notice dramatic changes in their subjective complaints, dizziness, or imbalance; as well as in objective measures. MEDICINE:IT’S A NOBLE PROFESSION, IT SERVES HUMANITY 18/19
- 19. PHYSICAL THERAPY PRINCIPALS & METHODS PTP&M:009 Revision: 01 Page: 19 of 19 PHYSICAL THERAPY MANAGEMENT OF PERIPHERAL NERVOUS SYSTEM TRAUMA AND DISEASE RELATED PATIENTS NOTICE: This specification, and the subject matter disclosed therein, embody proprietary information which is the confidential property of Mullsons Health & Wellness, which shall be copied, reproduced, disclosed to others, published, and could be used in whole or part, for any purpose, without the express advance written permission of a duly authorized agent of the Company. This specification is subject to recall by Mullsons Health & Wellness at any time. MEDICINE:IT’S A NOBLE PROFESSION, IT SERVES HUMANITY 19/19
- 20. Filename: PTP&M009 PTM of Peripheral Nervous System trauma and disease Medical Journal Directory: C:UsersAnjumDocumentsShadab MullaMullsons Medical Journals Template: C:UsersAnjumAppDataRoamingMicrosoftTemplates Normal.dot Title: PHYSICAL THERAPY MANAGEMENT OF PERIPHERAL NERVOUS SYSTEM TRAUMA AND DISEASE RELATED PATIENTS Subject: Author: Abdulrehman Mulla Keywords: Comments: Creation Date: 4/11/2009 8:12 AM Change Number: 18 Last Saved On: 6/4/2009 3:48 PM Last Saved By: Abdulrehman S. Mulla Total Editing Time: 500 Minutes Last Printed On: 6/4/2009 3:48 PM As of Last Complete Printing Number of Pages: 19 Number of Words: 4,328 (approx.) Number of Characters: 24,674 (approx.)