
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Intrauterine growth restriction when to deliver by dr alka mukherjee & dr apurva mukherjee nagpur m.s. india
Similar a Intrauterine growth restriction when to deliver by dr alka mukherjee & dr apurva mukherjee nagpur m.s. india (20)
Más de alka mukherjee
Más de alka mukherjee (20)
Último
Último (20)
Intrauterine growth restriction when to deliver by dr alka mukherjee & dr apurva mukherjee nagpur m.s. india
- 1. Dr Alka Mukherjee Nagpur 1 INTRAUTERINE GROWTH RESTRICTION: WHEN TO DELIVER? DR ALKA MUKHERJEE DR APURVA MUKHERJEE NAGPUR M.S. INDIA
- 2. DR ALKA MUKHERJEE MBBS DGO FICOG FICMCH PGDCR PGDMLS MA(PSY) Director & Consultant At Mukherjee Multispecialty Hospital MMC ACCREDITATED SPEAKER MMC OBSERVER MMC MAO – 01017 / 2016 Present Position Director of Mukherjee Multispecialty Hospital Hon.Secretary INTERNATIONAL COUNCIL FOR HUMAN RIGHTS Hon.Secretary NARCHI NAGPUR CHAPTER (2018-2020) Hon.Secretary AMWN (2018-2021) Hon.Secretary ISOPARB (2019-2021) Organizing secretary AMWICON – 2019 Life member, IMA, NOGS, NARCHI, AMWN & Menopause Society, India, Indian medico-legal & ethics association(IMLEA), ISOPARB, HUMAN RIGHTS Founder Member of South Rapid Action Group, Nagpur. On Board of Super Specialty, GMC, IGGMC, AIIMS Nagpur, NKPSIMS, ESIS and Treasury, Nagpur for “ WOMEN SEXUAL HARASSMENT COMMITTEE.” mukherjeehospital@yahoo.com www.mukherjeehospital.com https://www.facebook.com/ Mukherjee Multispeciality https://www.instagram.com/ Achievement Winner of NOGS GOLD MEDAL – 2017-18 Winner of BEST COUPLE AWARD in Social Work - 2014 VIDARBHA RATNA PURASKAR - 2019 Past Position Vice President of NOGS(2016-2017) Organizing joint secretary ENDO-GYN Vice President IMA Nagpur (2017-2018) Organizing joint secretary ENDO-GYN 2019
- 3. INTRODUCTION • Pregnancies with intrauterine growth restriction (IUGR) - a major obstetric problem • Associated with increased neonatal morbidity and mortality • Adverse intrauterine environment may increase disease risk of hypertension, diabetes, coronary heart disease, and stroke in adulthood. • Affects up to 10% of all pregnancies. • Majority of such pregnancies will have a physiologically normal foetus that is simply small for gestational age (sga), the ability to differentiate such a foetus from the pathologically growth-restricted foetus is limited.”
- 5. • The management of growth restriction depends on the cause. In 40% of cases, however, the cause is not definite which also necessitates management.
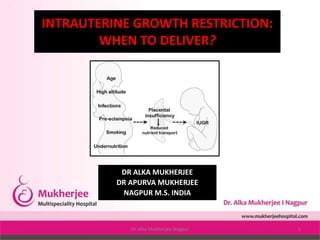
- 6. Causes of Intrauterine Growth Restriction • Maternal causes: • Chronic hypertension • Pregnancy-associated hypertension • Cyanotic heart disease • Class F or higher diabetes • Hemoglobinopathies • Autoimmune disease • Protein-calorie malnutrition • Smoking • Substance abuse • Uterine malformations • Thrombophilias • Prolonged high-altitude exposure • Placental or umbilical cord causes of IUGR include the following: • Twin-to-twin transfusion syndrome • Placental abnormalities • Chronic abruption • Placenta previa • Abnormal cord insertion • Cord anomalies • Multiple gestations
- 9. PATHO-PHYSIOLOGY OF IUGR • IUGR occurs when gas exchange and nutrient delivery to the fetus are not sufficient to allow it to thrive in utero. • This process can occur primarily because of maternal disease causing decreased oxygen-carrying capacity (eg, cyanotic heart disease, smoking, hemoglobinopathy), • A dysfunctional oxygen delivery system secondary to maternal vascular disease (eg, diabetes with vascular disease, hypertension, autoimmune disease affecting the vessels leading to the placenta), • Or placental damage resulting from maternal disease (eg, smoking, thrombophilia, various autoimmune diseases). • Evaluation of causative factors for intrinsic disorders leading to poor growth may include a fetal karyotype, maternal serology for infectious processes, and an environmental exposure history.
- 14. Perinatal Implications • IUGR causes a spectrum of perinatal complications: • fetal morbidity and mortality, • iatrogenic prematurity, • fetal compromise in labor, • need for induction of labor, and • cesarean delivery. • a increase in late fetal deaths among very small fetuses. • Almost 40 0% of stillborn fetuses not malformed are SGA. • Fetuses with IUGR who survive the compromised I-U environment - increased risk for neonatal morbidity - increased rates of necrotizing enterocolitis, renal failure thrombocytopenia, temperature instability - occur as a result of the alteration of normal fetal physiology in utero.
- 16. The brain-sparing effect • With limited nutritional reserve, the fetus redistributes blood flow to sustain function and to help in the development of vital organs - and results in increased relative blood flow to the brain, heart, adrenals, and placenta, with diminished relative flow to the bone marrow, muscles, lungs, gastrointestinal (GI) tract, and kidneys - may result in different fetal growth patterns. • Symmetrically small fetuses - early global insult (eg, aneuploidy, viral infection, fetal alcohol syndrome). • Asymmetrically small fetuses -small secondary to an imposed restriction in nutrient and gas exchange.
- 18. • Greater predisposition to develop a metabolic syndrome later in life - obesity, hypertension, hypercholesterolemia, cardiovascular disease, and type 2 diabetes - thrifty GENE HYPOTHESIS - intrauterine malnutrition results in insulin resistance, loss of pancreatic beta-cell mass, and an adult predisposition to type 2 diabetes. • Prepubertal individuals who had IUGR at birth show a greater insulin response than prepubertal individuals who had healthy growth as infants - increased risk of type 2 diabetes in adults who had restriction as infants stems, instead, from increased peripheral insulin resistance that allows the brain-sparing physiology to occur but with a permanent reduction in skeletal- muscle glucose transport. • This ultimately results in beta-cell burnout. • The causative pathophysiology is uncertain, the risk of a metabolic syndrome in adulthood is clearly increased among individuals who had IUGR
- 24. • ? An association between low birth weight and adult risk of ischemic heart disease. • ? Adult kidney function is adversely affected by restricted intrauterine growth. • ? Mental health problems morbidity academic impairment and poorer general health impaired fetal circulation, as demonstrated by Doppler studies, in association with IUGR results in worsened cognitive function in adulthood.
- 25. DETECTION OF INTRAUTERINE GROWTH RESTRICTION • Diagnosis by maternal physical examination - inaccurate 50% of cases. • A single fundaI height measurement at 32-34 weeks' -65- 85% sensitive and 96% specific for detecting the growth- restricted foetus. • When IUGR is suspected by maternal fundaI height, ultrasound for estimated foetal weight (EFW) assessment should be performed.
- 26. Diagnosis and Surveillance Criteria for diagnosis of IUGR • An EFW at or below the 10th percentile is used to identify fetuses at risk. (Short maternal or paternal height, the neonate's ability to maintain growth along a standardized curve, and a lack of other signs of uteroplacental insufficiency (eg, oligohydramnios, abnormal doppler findings) can be reassuring) • USG -an initial scan may be obtained in the middle of the second trimester (at 18-20 weeks) to confirm dates, evaluate for anomalies, and identify multiple gestations. A repeat scan may be scheduled at 28-32 weeks' gestation to assess fetal growth, evidence of asymmetry, and stigmata of brain- sparing physiology (eg, oligohydramnios, abnormal doppler findings).
- 27. • If the EFW is below the 10th centile, further sonographic evaluation should be performed, including Doppler flow studies, amniotic fluid assessment, and evaluation for structural abnormalities. • During initial evaluation, it is important to note whether growth restriction is symmetric, asymmetric, or a mixed pattern. • Intrinsic insults occurring early in pregnancy result in a symmetric growth restriction. • Extrinsic insults occurring later in pregnancy will likely result in asymmetric growth restriction. • Every tool must be used to identify the aetiology of IUGR.
- 29. THERAUPTIC OPTIONS • First, behavioral strategies to quit smoking result in a lower rate of low birth weight in babies at term among mothers who smoke. • Second, balanced nutritional supplements in undernourished women and magnesium and folate supplementation (in some studies) decrease the rate of SGA newborns. • Third, if malaria is the etiologic agent, maternal treatment of malaria can increase fetal growth.
- 30. The administration of steroids • The only intervention that has been shown to decrease neonatal morbidity and mortality is the administration of steroids to premature fetuses when delivery is anticipated. • Odds ratio reduction with steroids, from Bernstein et al, is as follows [7] : • Relative risk of death, 0.54; 95% CI, 0.48-0.62 • Relative risk of respiratory distress syndrome, 0.51; 95% CI, 0.44- 0.58 • Relative risk of intraventricular hemorrhage, 0.67; 95% CI, 0.61- 0.73 • Relative risk of severe intravascular hemorrhage, 0.5; 95% CI, 0.43-0.57 • Relative risk of necrotizing enterocolitis, no difference noted
- 31. The IUGR fetuses can be grouped as follows: • Small for gestational age (SGA): Small foetuses with no discernible pathology and with normal umbilical artery and middle cerebral artery Doppler results. • Growth restriction: Small foetuses with recognisable pathology/abnormal Doppler studies. • Idiopathic growth restriction: Small foetuses with no identifiable pathology/ abnormal Doppler studies.
- 32. STAGING SYSTEM • Staging of IUGR based on foetal biometry, Doppler cardiovascular changes, amniotic fluid volume, and clinical parameters. In addition, the staging system is applicable to pregnancies at any gestational age. The staging system is as follows: • Stage 0: Foetuses with EFW or an AC <10th percentile. Normal Doppler of the umbilical artery and middle cerebral artery. • Stage I: Foetuses whose EFW or AC is <10th percentile plus abnormal Dopplor flow of the umbilical artery or middle cerebral artery.
- 33. • Stage II: Foetuses whose EFW or AC is <10th percentile plus absent or reversed • Doppler flow of the umbilical artery. • Stage III: Fetuses whose EFW or AC is <10th percentile plus absent or reverend • Doppler flow of the ductus venosus. • Based on the amniotic fluid index (AFI), each IUGR foetus will be either (AFI <5 cm) or B (AFI 25 cm).
- 34. SITUATION-WISE MANAGEMENT • Situation 1 • Test results – AC less than fifth percentile, low AC growth rate, high ratio of head circumference to AC; BPS greater than or equal to 8 and AFV normal; abnormal UV and/or cerebroplacental ratio; normal MCA. • Interpretation – IUGR diagnosed, asphyxia extremely rare, increased risk of intrapartum distress. • Recommended management – Intervention for obstetric or maternal factors only, weekly BPS, multivessel Doppler every 2 weeks.
- 35. STAGING SYSTEM AND MANAGEMENT • Stage 0: SGA foetuses have a good prognosis , • managed as outpatient with dietary supplementation (NO donors, arginine granules, Protein supplementation) and • Doppler assessment every 2 weeks. • If the Doppler Teams normal, delivery at term. • If the Doppler becomes abnormal, these fetuses are managed as Stage I IUGR fetuses.
- 36. • Situation 2 • See the list below: • Test results – IUGR criteria met, BPS greater than or equal to 8, AFV normal, UA with absent or reversed end-diastolic velocities, decreased MCA. • Interpretation – IUGR with brain sparing, hypoxemia possible and asphyxia rare, at risk for intrapartum distress. • Recommended management – Intervention for obstetric or maternal factors only; BPS 3 times a week; weekly UA, MCA, and venous Doppler. SITUATION-WISE MANAGEMENT
- 37. • Stage 1: Fetuses having mild IUGR, affected mothers without pre-eclampsia are usually managed as outpatients. • Antenatal corticosteroids • In these fetuses - twice-weekly antenatal testing • If the non-stress testing (NST) remains reactive and the AFI remains >5 cm - delivery at 37 weeks' gestation. • If the umbilical artery Doppler becomes absent/reversed - manage as Stage II IUGR. STAGING SYSTEM AND MANAGEMENT
- 38. • Situation 3 • See the list below: • Test results – IUGR with low MCA PI; oligohydramnios; BPS greater than or equal to 6; normal IVC, DV, and UV flow. • Interpretation – IUGR with significant brain sparing, onset of fetal compromise, hypoxemia common, acidemia/asphyxia possible. • Recommended management – If at more than 34 weeks' gestation, deliver (route determined by obstetric factors). If at less than 34 weeks' gestation, administer steroids to achieve lung maturity and repeat all testing in 24 hours SITUATION-WISE MANAGEMENT
- 39. • Stage II: IUGR fetuses managed as inpatients. • During hospital management - twice-daily NST and daily biophysical profile (BPP). • If the NST reassuring and the BPP score between 6 and 8 - continuation of expectant management & • Antenatal corticosteroids at 28 weeks. • Delivery at 34 weeks. • If NSTs become non- reassuring or if the BPP score is <4/8 on 2 occasions at least 4 hours apart - immediate delivery By Caesarean delivery because fetuses with an absent/reversed flow of the umbilical artery may not tolerate labor induction. STAGING SYSTEM AND MANAGEMENT
- 40. • Situation 4 • See the list below: • Test results – IUGR with brain sparing, oligohydramnios, BPS greater than or equal to 6, increased IVC and DV indices, UV flow normal. • Interpretation – IUGR with brain sparing, proven fetal compromise, hypoxemia common, acidemia/asphyxia likely. • Recommended management – If at more than 34 weeks' gestation, deliver (route determined by obstetric factors and oxytocin challenge test [OCT] results). If at less than 34 weeks' gestation, individualize treatment with admission, continuous cardiotocography, steroids, maternal oxygen, and/or amnioinfusion and then repeat all testing up to 3 times a day depending on status. SITUATION-WISE MANAGEMENT
- 41. • Stage III: IUGR fetuses are managed the same as stage II except for delivery at 32 weeks' gestation, regardless of gestational age at time of diagnosis. • As with stage I and II - antenatal corticosteroids The advantage of the above scoring system is its simplicity. Only foetal biometry. Doppler evaluation, and the amniotic fluid index are needed. STAGING SYSTEM AND MANAGEMENT
- 42. • Situation 5 • See the list below: • Test results – IUGR with accelerating compromise, BPS less than or equal to 6, abnormal IVC and DV indices, pulsatile UV flow • Interpretation – IUGR with decompensation, cardiovascular instability, hypoxemia certain, acidemia/asphyxia common, high perinatal mortality, death imminent • Recommended management – If fetus is considered viable by size, deliver as soon as possible at tertiary center. Route determined by obstetric factors and OCT results. Fetus requires highest level of neonatal ICU care. SITUATION-WISE MANAGEMENT
- 43. • If the umbilical artery and middle cerebral artery Doppler are normal, Doppler study of the ductus venosus is unnecessary because it will be normal as well. • The presence MGR in the setting of pre-eclampsia should not deter standard management of pre-eclampsia. STAGING SYSTEM AND MANAGEMENT
- 44. • The diagnosis of severe IUGR before 32 weeks' gestation is associated with a poor prognosis, and therapy must be highly individualized. • Once a decision has been made to effect delivery, the mode of delivery is governed by evidence of acidemia, gestational age, and Bishop score. • Cesarean delivery without a trial of labor may be appropriate (1) in the presence of evidence of fetal distress by nonstress testing or reversed diastolic flow or (2) for traditional obstetrical indications for cesarean delivery (ie, malpresentation, prior cesarean delivery).
- 45. IMPORTANT CAUSES OF IUGR AND THEIR MANAGEMENT • The most important factor -when to deliver an IUGR fetus. • Repeat the investigations according to the extent IUGR and • Close monitoring is absolutely essential on a case-to-case basis and to delay delivery as close to fetal maturity as possible. • Gestational diabetes mellitus and the degree of glucose intolerance has to be identified during pregnancy. A diagnostic 75 g oral glucose tolerance test (OGTT) after overnight fast at least 8 hours should be tested at 24-28 weeks and must be repeated periodically to monitor glucose control.
- 46. • Patients with (GDM) must be taught the importance of self glucose monitoring (capillary). • Pre-pregnancy counselling and • Antenatal management are essential for optimising of glycaemic control, keeping glycosylated hemoglobin (HbA1C) less than 6.5-7%. • Dietary control, oral hypoglycaemic agents or properly chosen insulin and its dosage along with frequent monitoring -optimum results. • Try to prevent every complication of diabetes.
- 47. DIAGNOSIS • Diagnose - Abnormalities affecting the structure and function of the foetus as early as possible. • Screening methods for chromosomal abnormalities have improved over years, e.g. biochemical markers in 1 st and 2nd trimester of pregnancy, • Advances in ultrasonography, colour Doppler and 3D and 4D screening for birth defects; • Invasive tests such as amniocentesis, CVS, cordocentesis for foetal cord blood sampling
- 48. • Noninvasive prenatal foetal chromosomal study from maternal blood is available only at some centers. • Preimplantation genetic diagnosis is rarely utilized for couples with high risk of transmitting an inherited condition. • Depending on the case and type of anomaly, discontinuation of pregnancy may be decided after counseling. • Chronic urinary infection in pregnancy needs proper diagnosis and long-term treatment.
- 49. • Overall general health of the patient and • management of anaemia, hypothyroidism and infections • Investigate - Thromboembolic disease during pregnancy especially when there is recurrent IUGR. • Appropriate treatment by anti thrombotic and thrombolytic agents such as low molecular weight heparin, aspirin, steroids are given almost through the pregnancy and decision to deliver the patient depends on the results of monitoring.
- 50. • Hypertension during pregnancy causes placental ischaemia with endothelial dysfunction and IUGR. • Chronic reduction in uteroplacental perfusion - detect by series of tests—clinical, biochemical, sonographic and Doppler • Management with antihypertensive agents, nitric oxide donors, L- arginine treatment, low-dose aspirin - effective along with very close monitoring timely treatment and delivery. • Endothelial cell dysfunction - main component of the patho physiology of pre-eclampsia and in spite of medical treatment, the decision for timely delivery is most important.
- 51. Management of twins • Delivery depends on chorionicity, prenatal screening for chromosomal and structural abnormalities and placental evaluation. • Cervical length measurements and foetal growth studies in IUGR in twin pregnancy - most important especially in discordant and monochorionic twins. • A careful approach to diagnosis and management – for better outcomes, preventing unanticipated stillbirth and allowing appropriate timing of delivery.
- 52. • Integration of different testing modalities allows adjustment of monitoring interval based on Doppler parameters and a more precise prediction of acid-base, status based on biophysical variables. • The presence of a well-equipped neonatal intensive care unit (NICU) and a well-trained neonatologist – must. • For the obstetrician and the neonatologist - the balance of fetal risks of continuation of pregnancy the neonatal risks after birth that dictates the timing of delivery.
- 53. TIMING OF DELIVERY • There is a temporal sequence of Doppler changes preceding the onset of late decelerations. • Early Doppler changes occur in all the IUGR fetuses, • Whereas late Doppler changes occur in idiopathic IUGR and only in a few IUGR cases diagnosed in patients with pre- eclampsia. • In pre eclamptic patients - the changes are unpredictable, and can occur in a few hours, and in most cases, do not occur because delivery is done for maternal indication.
- 55. TIMING OF DELIVERY FOR VERY PREMATURE GROWTH-RESTRICTED FOETUSES • At the current time, it is not possible to identify optimal timing of delivery in very premature IUGR fetuses. • Mostly, the decision to deliver a growth-restricted foetus based on abnormal antenatal testing, an abnormal BPP or NST, or abnormal Doppler study. • In terms of survival rate, the growth-restricted foetus delivered at >25 and <30 weeks - most problematic.
- 56. • The very early IUGR foetuses are delivered in the presence of either NST or an abnormal BPP (<4/8 confirmed at 2 hours apart). • Fetuses diagnosed with stage I or higher IUGR involving abnormal Doppler studies should be monitored closely. • Still delivery solely on the basis of abnormal Doppler studies has not been proven beneficial and, in most cases, fetuses with abnormal Doppler studies do well in the setting of reassuring antenatal testing.
- 57. MODE OF DELIVERY FOR IUGR FOETUSES • Data seems to support caesarean delivery for a growth- restricted foetus when there is absent or reversed flow of the umbilical artery because these fetuses rarely tolerate attempts at vaginal delivery.
- 58. Future Directions and Prevention • Decline in the rate of IUGR from 61.5% in the historic controls to 13.3% in those treated with aspirin and dipyridamole. • A small decrease in the rate of preeclampsia but not IUGR (at the risk of increased chance of abruption) • using 150 mg of aspirin in pregnant women with abnormal UA Doppler findings. (increase in birth weight and an increase in placental weight.) • Beginning 100-150 mg/d of aspirin at less than 17 weeks' gestation decreased the rate of IUGR by approximately 65% and the rate of perinatal mortality by approximately 60%. • Despite the theoretical benefit of aspirin in many studies, the role of aspirin, if any, in the prevention of IUGR is still unclear.
- 59. SUMMARY • Intrauterine growth restriction (IUGR) secondary to placental insufficiency - a major cause of perinatal morbidity and mortality worldwide. • No single test that appears superior to the other available tests for determining the timing of delivery of the growth- restricted fetus. • The presence of a well trained neonatologist at the time of delivery - valuable. • A few days gained by the foetus in utero between 25 weeks and 30 weeks gestation, can make a difference in the future of the IUGR baby.