
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (20)
Similar a Blood film examination
Similar a Blood film examination (20)
Más de ayeayetun08
Más de ayeayetun08 (10)
Último
Último (20)
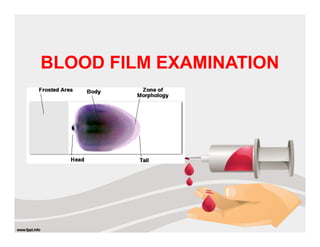
Blood film examination
- 2. BLOOD FILM PREPARATION made on clean glass slides Films may be spread by hand or by means of an automated slide spreader Manual Method
- 3. • Hemogram: measured and calculated parameters • Histograms: size distribution of WBC, RBC and Plt • Cytogram: WBC differential CBC on automated analyzers Flagging for abnormalities necessitates a manual PBS review
- 4. STAINING BLOOD AND BONE MARROW FILMS Romanowsky stains are used universally for routine stainingof blood films Giemsa’s Stain Leishman’s Stain Automatic staining machines are available that enable large batches of slides to be handled
- 5. EXAMINATION OF BLOOD FILMS examined systematically starting with macroscopic observation of the stained film assess whether the spreading technique was satisfactoryand to judge its staining characteristics and either any abnormal particles present
- 6. EXAMINATION OF BLOOD FILMS Microscopic examination- progressing from low- power to high-power Under low magnification to: (a) get an idea of the quality of the preparation (b) assess whether red cell agglutination, excessive rouleaux formation or platelet aggregation is present (c) assess the number, distribution and staining of the leucocytes (d) find an area where the red cells are evenly distributed and are not distorted
- 7. EXAMINATION OF BLOOD FILMS Having selected a suitable area, Inspection under high-power magnification for the final examination of unusual cells and for looking at fine details
- 8. 1. RBC Size, Shape Stain Arrangement Inclusions nucleated RBCs 2. WBC Total counts Differential counts Abnormal /immature WBC 3. Platelets Counts Abnormality 4. Parasites EXAMINATION OF BLOOD FILMS
- 9. RED CELL MORPHOLOGY NORMAL SHAPE - round, smooth contours SIZE- range of 7–8 μm (about the same as that of the nucleus of a small lymphocyte on the dried film) STAIN - Central pallor 1/3 of total area stain quite deeply with the eosin component of Romanowsky dyes, particularly at the periphery of the cell as a result of the cell’s normal biconcavity
- 10. Biconcave disc Diameter : 7 - 8 μm Central pallor occupy 1/3 rd of total Size : approx. same as nucleus of mature lymphocyte NORMAL RED CELL MORPHOLOGY
- 11. blood film from a healthy adult
- 12. ABNORMAL ERYTHROPOIESIS Anisocytosis- variation in size of RBC result of the presence of cells larger than normal (macrocytosis), cells smaller than normal (microcytosis) or both; frequently both macrocytes and microcytes are present
- 13. Microcytes results from a defect in haemoglobin formation characteristic of iron deficiency anaemia various types of thalassaemia and severe cases of anaemia of chronic disease. Anisocytosis
- 14. Anisocytosis Macrocytes classically found in megaloblastic anaemias also present in some cases of aplastic anaemia, myelodysplastic syndromes ,other dyserythropoietic states, in patients being treated with hydroxyurea, chronic alcoholic & chronic liver disease
- 15. Poikilocytosis –variation in shape of RBC produced in many types of abnormal erythropoiesis for example - megaloblastic anaemia - iron deficiency anaemia - Thalassaemia - Myelofibrosis ABNORMAL ERYTHROPOIESIS
- 16. Poikilocytosis Elliptocytes and ovalocytes present when there is dyserythropoiesis in megaloblastic anaemia (macro-ovalocytes) in iron deficiency anaemia (‘pencil cells’)
- 17. Target Cells refers to a cell in which there is a central round stained area and a peripheral rim of haemoglobinized cytoplasm separated by non- staining or more lightly staining cytoplasm result from cells having a surface that is disproportionately large compared with their volume are seen in films in chronic liver diseases, iron deficiency anaemia and thalassaemia Poikilocytosis
- 18. Sickle Cells - vary in shape between boat-shaped forms and sickles SPICULATED CELLS AND RED CELL FRAGMENTATION - Schistocytosis – Fragmented red cells - Acanthocytosis- abnormality of the red cell in which there are a small number of spicules of inconstant length, thickness -Stomatocytosis , Red cell inclusion bodies- Howell–Jolly Bodies Pappenheimer Bodies Basophilic stippling or punctate basophilia Poikilocytosis
- 19. Basophillic stippling Hereditary spherocytosis target cells
- 20. seen when there is extramedullary erythropoiesis Tear drop cells / dacrocytes • Osteopetrosis • Myelofibrosis • Bone marrow infiltrated with hematological or non-hematological malignancies • Iron deficiency anemia • Pernicious anemia
- 21. INADEQUATE HAEMOGLOBIN FORMATION Hypochromia refers to the presence of red cells that stain unusually palely two possible causes: a lowered haemoglobin concentration and abnormal thinness of the red cells
- 22. Hyperchromasia (Hyperchromia) deep staining of the red cells with a lack of central pallor seen in two circumstances - in the presence of macrocytes - cells are abnormally rounded Abnormally rounded cells may be either spherocytes or irregularly contracted cells
- 23. Spherocytosis cells that are more spheroidal (i.e. less disc like) than normal red cells but maintain a regular outline diameter is less and thickness is greater than normal result from genetic defects of the red cell membrane as in hereditary spherocytosis, haemolytic anaemia
- 24. Anisochromasia- Dimorphic Red Cell Population abnormal variability in staining of red with two distinct populations is characteristic of a changing situation It can occur during the development or resolution of iron deficiency anaemia
- 25. Polychromasia Blue-gray coloration of RBCS. Due RNA remnants Increased - Increased erythropoietic activity. Decreased - Hypoproliferative states. Hemolytic anemias •Blood loss anemias •Recovering anemia
- 26. Hypochromic Microcytic Anaemia Iron deficiency Anaemia Thalasemia Anemia of chronic disease
- 29. Hypochromic microcytic anemia of iron deficiency (peripheral blood smear)
- 30. Examination of peripheral blood film RBC shows Hypochromic Microcytic anaemia with moderate anisocytosis & poikilocytosis with the presence of elliptical forms, elongated pencil shaped cells WBC - white cell count and differential are normal Platelet - normal Comment: Hypochromic Microcytic anaemia Differential diagnosis: Iron deficiency anaemia Thalasaemia
- 31. Investigation of a microcytic hypochromic anaemia
- 32. Microcytosis Macrocytosis Target cells Spherocytes Red cell fragments Nucleated red blood Howell-Jolly body Basophilic stippling Polychromasia abnormal ribosom al RNA appears as blue dots
- 33. Shows marked anisocytosis, marked poikilocytosis, one unusually large macrocyte and one severely hypochromic cell
- 34. Blood film showing macrocytes, oval macrocytes & a hypersegmented neutrophil
- 35. Blood film showing hypochromia, microcytosis and poikilocytosis
- 36. Investigation of a macrocytic anaemia