

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (20)
Similar a Genetic sonogram
Similar a Genetic sonogram (20)
Último
Último (20)
Genetic sonogram
- 3. NON - INVASIVE TOOL PROVIDES A TANGIBLE & REALISTIC MODALITY PATIENTS CAN VISIBLY SEE FOR THEMSELVES COST EFFECTIVE HIGH SENSITIVITY IN DETECTING MARKERS/ANOMALIES MORE SOPHISTICATED & HIGH- RESOLUTION USG
- 4. OBSERVATION CHROMOSOMAL ABNORMALITY HEAD TRISOMY-18,13 •Strawberry skull TRIPLOIDY •Hydrocephalus •Holoprosencephaly •Choroid plexus cyst FACE TRISOMY-13,18 •Cleft lip/cleft palate Meckel-Gruber syndrome •Low set ears TRIPLOIDY HEART TRISOMY-13,18,21 •VSD,ASD •Coarctation of aorta
- 5. OBSERVATION CHROMOSOMAL ABNORMALITY RENAL TRISOMY-13,18,21 • Horseshoe kidney TRIPLOIDY • B/L dilatation of renal pelvis • Cystic dysplasia HANDS/FEET TRISOMY-18,13,21 •Flexed overlapping fingers •Rocker bottom/club foot •Polydactyly •Wide gap b/w 1st &2nd toes (Sandal-gap) •Clinodactyly •Short femur/humerus
- 6. OBSERVATION CHROMOSOMAL ABNORMALITY G.I SYSTEM TRISOMY-13,18 Omphalocele TRISOMY-21 Duodenal atresia Echogenic bowel GENERAL Growth restriction TRISOMY-13,18,21 Hydrops TRIPLOIDY;45-XO
- 7. OBSERVATION CHROMOSOMAL ABNORMALITY PLACENTA Partial mole ANEUPLOIDY UMBILICAL CORD TRISOMY-18
- 8. NUCHAL TRANSLUCENCY With severe LYPHANGIECTASIA → overall swelling of the fetal soft tissue ↓ Thickening of the nuchal soft tissues ↓ NUCHAL TRANSLUCENCY
- 9. Refers to the normal subcutaneous fluid filled space between the back of the fetal neck & the overlying skin. The single most powerful marker available today for differentiating DS from euploid pregnancies.
- 11. POSSIBLE CAUSES OF ↑ FLUID FILLED SPACE(NT) Cardic failure secondary to structural malformation Abnormality in the extracellular matrix Abnormal or delayed development of the lymphatic system
- 12. CAUSES ANEUPLOIDIES SKELETAL DYSPLASIA Carnelia de Lange Achondrogenesis Noonan syndrome Ectrodactyly-ectodermal Smith-Lemli-Opitz dysplasia Joubert Multiple Pterygium Syndrome Apert Robert Syndrome Fryns CHROMOSOMAL ANOMALIES Trisomy-21 (most common) Trisomy-13,18,22 Triploidy Tetrasomy -12p
- 13. Imaged in the mid sagittal plane, ideally with the fetal spine down. Image should be adequately magnified so that only the fetal head ,neck & upper thorax fill the viewable area The fetal neck should be neutral-avoid measurements in the hyperflexed/hyper extended positions The skin at the fetal back should be clearly differentiated from the underlying amniotic membrane
- 14. Measurement calipers should be optimized to ensure clarity of the image and of the borders of the nuchal space in particular (TVS) The width of the lucency alone, excluding the width of the surface or occiput
- 16. PITFALLS PRESENCE OF An Encephalocele Nuchal cord An Amniotic band A loose amnion that can be mistaken for the nuchal skin edge
- 17. How to rectify? MAGNIFY THE IMAGE WAIT FOR SPONTANEOUS FETAL ACTIVITY → as the fetus bounces from the amnion ,the edges can be distinguished more reliably COLOR DOPPLER → presence of a umbilical cord in the vicinity of the fetal neck.
- 18. Cut off value of 3mm as a threshold for an abnormal nuchal translucency Normal NT thickens with increasing GA Currently, the more accepted method is to base the cut off on a progressive rise >95th percentile as a threshold. MOM Vs SD: MOM-reduction in false +ve rates
- 19. •Equal success (Braithwaite & Economides) METHOD Gestational Age Success rate TAS 10-13 WEEKS 98% to 100% TAS AT 14 WEEKS 90% TVS is needed
- 20. 10-14weeks of GA Detection rate False+ve rate Study group 77% 5% Fetal medicine foundation, London 63% 5% The SURUSS trial,UK 69% 5% The BUN trial, US 70%-64% 5% The FASTER trial, US
- 21. Nicholaides: First trimester NT =/> 3mm Detection rate→86% of Trisomic fetus False +ve rate→4.5% Pandya (1995): NT (mm) 3 4 5 >6 RISK ↑ 3 18 28 36 •TRISOMIES 13,18,21 •FETAL LOSS RATE =15% with NT of 5mm •↑ NT → ↑ RISK OF CONGENITAL HEART DEFECT •With Normal Karyotype & with abnormal karyotype
- 22. Progression from an abnormal NT to a normal one→ not necessarily indicative of a nomal Karyotype So the fetus with nuchal abnormalities → candidates for amniocentesis ,regardless of whether the abnormality resolves Among the women with advanced maternal age b/w 11-14wks GA→NT can be used to determine which patients would benefit from an early First trimester Amniocentesis/CVS, Vs delay of the invasive testing until 16 weeks for the safest possible procedure.
- 23. MAJOR CARDIAC ANOMALIES DIAPHRAGMATIC HERNIA ANT. ABD.WALL DEFECT FETAL AKINESIA/DYSKINESIA SYNDROME OTHERS- Cornelia de lange,Noonan,Smith-lemli- Opitz,Joubert,Apert&Fryns SKELETALANOMALIES→ Achondrogenesis,Ectrodactyly-ectodermal dysplasia,Multiple Pterygium syndrome,Robert syndrome
- 24. Localised nuchal fluid→CYSTIC HYGROMA(CH) FETAL HYDROPS DIFFUSE EDEMA SEPTATED CH: ANEUPLOIDY EUPLOID 50% 50% 50%-MAJOR structural malformation CARDIAC x12 SKELETAL DYSPLASIA
- 26. Presence of Septations within a nuchal swelling is ominous Non - Septate CH Septate CH 98%- transient 44%-transient 6%→ Abnormal 72%→ Abnormal Karyotype Karyotype Bronshtein et al.
- 27. NO NEED TO DELAY DECISION MAKING→ while awaiting serum marker results/using computerized risk calculation algorithms IMMEDIATE OPTIONS FOR CVS IF NO FETAL ANEUPLOIDY→ A DETAILED FETAL ANATOMIC EVALUATION + FETAL ECHOCARDIOGRAPHY AT 18-20 WEEKS
- 28. FASTER TRIAL- >3mm NT → CVS SHOULD BE OFFERED IMMEDIATELY,because of a minimum risk of aneuploidy of 1 in 6. NO ROLE FOR DELAYING DECISION MAKING while awaiting serum marker results,because such additional information does not meaningfully alter the original aneuploidy risk
- 29. GROWTH PATTERNS- CRL NASAL BONE DUCTUS VENOSUS SONOGRAPHY TRICUSPID REGURGITATION ANTERIOR ABDOMINAL WALL DEFECTS ENCEPHALOCELES LIMB DEFORMITIES HEART DEFECTS
- 30. Schemmer et al; CRL→ NOT significantly reduced with Trisomy-21,Turner Syndrome or Sex chromosome Trisomies → SIGNIFICANTLY reduced growth rates with Trisomies 13 & 18 and Triploidy
- 31. ABSENCE OF NASAL BONE & DS Cicero et al; (N= 701 fetuses with ↑NT) ABSENCE OF NB PRESENCE OF NB 73% 0.5% (43 OF 59) (3 OF 602) NOT RELATED TO ↑ NT COULD BE COMBINED INTO A SINGLE USG SCREENING MODALITIES PREDICTED SENSITIVITY OF 85% FOR 1% FALSE +VE RATE.
- 32. MID SAGITTAL PLANE FETAL PROFILE FACING UPWARD ADEQUATE MAGNIFICATION VISUALIZATION OF TWO PARALLEL LINES AT THE LEVEL OF THE FETAL NOSE→ 1. Superficial: fetal skin 2. Deeper: nasal bone NASAL BONE- MORE ECHOLUCENT AT THE DISTAL END.
- 33. INCIDENCE OF ABSENT NASAL BONE GENERAL HIGH RISK POPULATION POPULATION 17%-29% 48% LIMITED ROLE AS A SCREENING TOOL FOR GENERAL POPULATION
- 34. FORWARD TRIPHASIC PULSATILE FLOW→ NORMAL REVERSED FLOW AT THE TIME OF ATRIAL CONTRACTION →ANEUPLOIDY/FETAL CARDIAC MALFORMATION WITH NT → ↑ THE DETECTION RATE/↓ THE FALSE +VE RATE
- 35. PITFALLS The ductus venosus vessel- as small as 2mm at 10-14weeks Very difficult to get proper image SECONDARY SCREENING TEST IN THE HANDS OF EXPERIENCED SONOLOGIST
- 36. CHEST WALL-ANTERIOR THE FETAL HEART SHOULD BE ISONATED PARALLEL TO THE VENTRICULAR SEPTUM HIGH RISK PREGNANCIES AT 11-13 WEEKS Significant TR INCIDENCE NORMAL FETUS 4% DS Fetus 68% TRISOMY- 18 33% SECOND LINE TEST
- 37. AT 10-14 WEEKS Normal parameters GA(weeks) FHR (beats/min) 10 171 14 156 Higher than normal rate- TRISOMY-21 Lower than normal rates- TRIPLOIDY & TRISOMY-18
- 38. SENSITIVITY ABNORHAL FHR- 26% NT- 72% MATERNAL AGE- 48% MATERNAL AGE+ NT + FHR- 83% of detection rate at 5% false +ve rate
- 39. Authors Parameter Sensitivity False +ve rate Orlandi et al. NT alone 57% 5.8% NT + 87% 5.8% biochemistry & maternal age Noble et al; NT + 80-85% Biochemistry & maternal age BEST DETECTION RATE IN 1ST TRIMESTER- Urine free β- hCG , beta core & Oestriol + NT
- 40. 10-14 WEEKS NT SONOGRAPHY CYSTIC HYGROMA NO CYSTIC HYGROMA CVS SINGLETONE MULTIFETAL EUPLOID ANEUPLOID GESTATION GESTATION 18-20 WKS COUNCEL ANATOMY SCAN & FETAL ECHO
- 41. NT + NO CYSTIC HYGROMA SINGLETONE GESTATION MULTIFETAL GESTATION NT + SERUM MARKERS NT INTERPRETED WITH PAPP-A & β- hCG MATERNAL AGE ONLY RISK ↑ RISK ↑ RISK NOT↑ CVS EUPLOID CVS EUPLOID ANEUPLOID ANEUPLOID 18-20 WKS COUNCEL ANATOMY SCAN & COUNCEL FETAL ECHO
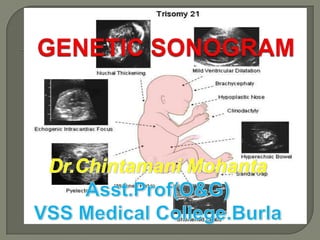
- 42. MOST COMMON SONOGRAPHIC MARKERS NUCHAL FOLD THICKENING ECHOGENIC INTRACARDIAC FOCUS SHORTENED LONG BONES HYPERECHOIC BOWEL RENAL PYELECTASIS CHOROID PLEXUS CYST CLINODACTYLY HYPOPLASTIC OR ABSENT NASAL BONE
- 43. EXCESS SOFT TISSUE IN THE POSTERIOR NECK AREA Measurement TS OF FETAL HEAD ANGLED POSTERIORLY TO INCLUDE THE CEREBELLUM & THE OCCIPITAL N T BONE OUTSIDE OF THE OCCIPITAL BONE OUTER SKIN EDGE
- 44. THE NUCHAL SKIN FOLD MEASUREMENT THRESHOLD AUTHORS Gestational Threshold Age Gray & Crane 14-17 wks 5mm 18-20 wks 6mm Wilson < 17wks 5mm
- 45. SENSITIVITY AUTHORS CUT OFF VALUE SENSITIVITY FALSE +VE Crane & >/= 5 mm 75% Gray Borrell & >/= 6 mm 33% 0.1% Colleagues Borrell & >/= 5mm 77.8% 2% Colleagues
- 46. May persists throughout the 2nd trimester Or regression may occur
- 47. ONCE AN ABNORMAL NUCHAL SKIN MEASUREMENT IS OBTAINED,THEREFORE ,AN AMNIOCENTESIS IS INDICATED, REGARDLESS OF WHETHER THE NUCHAL SKIN THICKNESS RESOLVES
- 48. TRISOMY-21 oSHORT STATURED oSHORT FEMURS oSHORT HUMERI RATIOS OF THE MEASURED - TO - EXPECTED FL OF </= 0.91, BPD. EXPECTED FL = - 9.3105 + 0.9028 x BPD
- 49. SENSITIVITY STUDY SENSITIVITY FALSE +VE RATE LOCKWOOD 50% 7% CALLEN 68% GRIST 50% 6.5%
- 50. Study Parameter Sensitivity False +ve Anomalies rate Brumfield BPD: FL 40% 2.2% TRISOMY- et al; >/= 1.8 18 & 21 Ginsberg -do- 53% 7% - do- et al; Ginsberg + NT 81% 7% - do- et al; NOT A HELPFUL TOOL FOR SCREENING OF DS USEFUL IN COMBINATIONS WITH OTHER SONOGRAPHIC MARKER Eg: HUMERUS LENGTH & PYELECTASIS
- 51. THE MEASURED- TO – EXPECTED HUMERUS LENGTH = - 7.9404 + 0.8492 x BPD < 0.90 as a cut - off STUDY METHODS SENSITIVITY FALSE +VE Callen HL 50% 6.25% Rodis et al; HL 54% FL 18% Biagiotti FL + HL ↑ ↓↓ Periti Cariati
- 52. Nyberg et al; Short FL + HL 11 fold ↑ risk of DS Johnsons et al; FL+ HL 53% - sensitivity Foot Length 7% - false +ve rate
- 54. An antero-posterior diameter of the renal pelvis >/=4 mm
- 55. STUDY METHOD SENSITIVITY FALSE +VE Callen PYELECTAS 25% IS Crane & -do- 18.7% Gray Corteville , -do- 17% 2% Dicks & Crane ISOLATED PYELECTASIS- ↑risk NOT SUFFICIENT TO INDICATE AMNIOCENTESIS USED IN COMBINATION WITH OTHER
- 56. THE BOWEL IS AS ECHOGENIC AS BONE 0.6% OF ALL 2ND - TRIMESTER FETUSES BE AWARE: High frequency transducer may tend to accentuate the echogenicity of the fetal bowel in NORMAL fetus
- 57. ↑ RISK OF IUGR PREMATURITY FETAL DEMISE POOR PERINAL OUTCOME APH CYSTIC FIBROSIS - Parental allele testing for CF carrier status is recommended IN-UTERO CMV INFECTION
- 58. MINERALIZATION IN THE PAPILLARY MUSCLE UNILATERAL BILATERAL
- 59. 90% in the left ventricles When the Right ventricle or both ventricles are involved ↑ risk of Chromosomal anomalies FETAL STATUS EIF in Left EIF in Right / B/L Ventricle Normal 88% 12% Down Syndrome 78% 22%
- 60. STUDY NORMAL TRISOMY- 21 TRISOMY- 13 Brown,Roberts 2% 16% 39% & Miller Callen 4.7% 18% Association of EIF & Chromosomal anomalies is low in low risk patient NO AMNIOCENTESIS Not associated with cardiac anomalies in low risk patient
- 61. NORMAL FETUSES - 0.3% TO 3.6% 1/3RD OF FETUSES WITH TRISOMY - 18 •16-21 WEEKS → TRANSIENT •BY 23RD WEEKS → USUALLY REGRESS •25-26 WEEKS → UNCOMMON
- 62. U/L SINGLE SMALL B/L MULTIPLE LARGE SIZE = 0.5 cm – 2cm Very large CPC → Fill almost the entire lateral ventricle & expands its walls → FALSE VENTRICULOMEGALY
- 63. + OTHER ISOLATED CPC SONOGRAPHIC FINDINGS CONSERVATIVE INVASIVE TESTING With detailed fetal sonographic anatomic survey by experts
- 64. EXAMINING THE UA TRANSVERSE VIEW OF A FREE RUNNING ALONGSIDE & LOOP OF CORD AROUND THE BLADDER Transverse view of the pelvis
- 65. 17% - CYTOGENETIC ABNORMALITY TRISOMY- 18 ( Most Common ) TRISOMY- 13 TURNERS SYNDROME (45X) TRIPLOIDY Commonly seen in normal fetuses It is non-specific The most common organ system involved – HEART , GI SYSTEM & CNS
- 66. A targeted & detailed fetal ISOLATED SUA – anatomic survey should be No ↑ incidence for a done with detailed chromosome evaluation of the heart abnormality
- 67. ILIAC WING ANGLE ILIAC LENGTH FRONTOTHALAMIC DISTANCE (BRACHYCEPHALY) SHORTENED FRONTAL LOBE ABNORMAL FHR ABNORMALLY SHORTENED EAR LENGTH FLAT FACIES CLINODACTYLY(with hypoplasia of the middle phalanx of the fifth digit) SANDAL GAP GREAT TOE SIMIAN CREASE OF THE PALM EAR LENGTH & WIDTH
- 68. LOW RISK NO further Testing Normal USG No markers present HIGH RISK DS risk adjustment LOW RISK NO further Testing 1-ISOLATED MARKER (Except-Nuchal fold/ Absent Nasal Bone Genetic Amniocentesis HIGH RISK >/=2 MARKERS/Thick LOW RISK Genetic Amniocentesis Nuchal Fold/ Absent Nasal Bone/Structural Anomaly HIGH RISK Genetic Amniocentesis
- 69. STRUCTURAL ABNORMALITIES ANEUPLOIDY MARKERS oCardiac defects Clinodactyly oCystic hygroma EIF oVentriculomegaly/hydrocephalus Hyperechoic bowel oEsophageal atresia Nuchal fold thickening /Tracheo-esophagial fistula Pyelectasis oDuodenal atresia Sandal gap oOmphalocele Short long bones Wide iliac angle OTHER FINDINGS SUA Brachycephaly Short ear length Flat facial profile Absent / hypoplastic Protruding tongue nasal bone Hydrops Hydrothorax Pericardial effusion Unfused amnion & chorion after 14 weeks
- 70. STRUCTURAL ABNORMALITY Cardiac defect Cystic hygroma Diaphragmatic hernia Omphalocele Esophageal atresia+/- TOF CNS-agenesis of corpuscallosum,ventriculomegaly,hydrocephalus,large cisterna magna,Dandy-Walker Malformation,cerebellar dysgenesis,neural tube defect CRANIOFACIAL- Strawberry-shaped skull,prominent occiput,dolichocephaly,ocular anomalies,micrognathia,cleft lip/palata,small,low set ears GENITO-URINARY- Hydronephrosis,horseshoe kidney,BOO,duplication abnormality,genital abnormality
- 71. EXTREMITY- Limb reduction abnormality,Radial aplasia,Clenched hands/Overlapping digits,Club feet,Rocker-bottom feet,Lower extremity/feet abnormality,Contracture/arthrogryposis/flexion deformity,movement disorders ANEUPLOIDY MARKERS- OTHER FINDINGS- Choroid plexus cyst IUGR,Amniotic fluid Strawberry-shaped skull abnormality,Umbilical Nuchal thickening cord cyst,Non immune hydrops Single Umbilical artery Shortened limbs
- 72. STRUCTURAL ABNORMALITIES- Cardiac defects,Cystic hygroma,Nuchal thickening,Omphalocele CNS- Holoprosencephaly,Agenesis of corpus callosum, Ventriculomegaly,Enlarged cisterna magna,Abnormal posterior fossa,Neural tube defects CRANIO-FACIAL- Microcephaly,Micrognathia,Cleft lip/palate,Facial defects,Ocular anomalies ,Sloping forehead,Small ears EXTREMITIES- Postaxial polydactyly,Overlapping digits,Camptodactyly,Radial aplasia,Rocker-bottom feet,Club feet UROGENITAL- Hydronephrosis,Cortical cysts,Horseshoe kidney,Echogenic kidney,Polycystic kidneys
- 73. ANEUPLOIDY MARKERS Echogenic Intracardiac Focus Pyelectasis Single Umbilical Artery OTHER FINDINGS Microcephaly IUGR Polyhydramnios
- 99. PAST Over the past decade & a half, AMNIOCENTESIS was reserved for woman of advanced maternal age PRESENT In the new millenium- major changes in the indications for INVASIVE GENETIC TESTING- such that advance maternal age alone will no longer be an indication FUTURE Whether a patient is at risk for fetal Aneuploidy will be based on the combination MATERNAL AGE,MULTIPLE BIOCHEMICAL SERUM MARKERS & perhaps a dozen SONOGRAPHIC MARKERS + a complete USG evaluation of the fetus.