
Recomendados
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (6)
Destacado
Destacado (9)
Similar a Celebrate life issue25
Similar a Celebrate life issue25 (20)
Más de Corrie T
Más de Corrie T (20)
Último
Último (20)
Celebrate life issue25
- 1. elebrateLife For Home TPN and Tube Feeding Patients Issue Focus: The Importance of Nutritional H E A LT H wHeN coPINg wITH Cancer A publication of September 2011 | Issue 25
- 2. Contents September 2011 | Issue 25 4 Quality of Life and Nutrition Support for the cancer Patient For most people, the main thing that determines quality of life is our ability to enjoy everything life has to offer with no major health symptoms. Learn about how nutrition support can help improve quality of life for cancer patients. 7 Eating Healthy to Help Prevent Cancer Celebrate Life The Quarterly Magazine for Home TPN Healthy food choices are a key to the prevention of many diseases, including cancer. A plant- and Tube Feeding Patients based diet is a great place to start to benefit from the disease-fighting abilities of diet. Celebrate Life Staff Carlota Bentley, Managing Editor Karen Hamilton, Clinical Editor 11 Nutrition and Cancer Care: Resource Organizations Laura Persons, Senior Editor Nancy Geiger Wooten, Senior Designer 12 The Effects of Cancer Therapy on Nutritional Well-Being Contributing Writers Elaine Arthur, RD Cancer treatment can affect nutritional health, while nutritional health can impact a cancer Michelle Barford, Consumer Tiffany Fancher, PharmD patient’s recovery. Learn how to anticipate, understand and alleviate nutrition problems as Linda Gravenstein, Consumer Advocate they relate to cancer therapy. Karen Hamilton, MS, RD, LD, CNSC Carol Ireton-Jones, PhD, RD, LD, CNSD 18 Home Care Therapies for Cancer Patients Roaxana Tamijani, MS, RD, LD Corrie Trottier, MS, RD, LD /N Pankaj Vashi, MD Cancer rates continue to rise in the U.S., but at the same time, treatment options have grown by leaps and bounds. Learn about what treatment options are available to cancer patients in Celebrate Life is published quarterly and provided as a free the comfort of their homes. service to parenteral and enteral consumers. Opinions expressed by contributing authors and sources are not 20 My Great Adventure necessarily those of the publisher. Information contained in this magazine is for educational purposes only and is not Sometimes nutrition support is short-term and uneventful — and sometimes it is anything intended as a substitute for medical advice. but! With a positive attitude and a sense of humor, Michelle Barford, a Coram nutrition Do not use this information to diagnose or treat a health problem or disease without consulting a qualified support patient, shares her dramatic story. physician. Please consult your physician before starting any course of treatment or supplementation, particularly 25 Tube Feeding: A Smart Weapon Against Cancer-Related Malnutrition if you are currently under medical care. Never disregard medical advice or delay in seeking it because of Studies have shown that cancer patients experience a good quality of life when they are something you have read in this publication. able to maintain their nutritional well-being. One way to battle cancer-related malnutrition © 2011 Coram Specialty Infusion Services. All rights reserved. No part of this publication may be distributed, — and one that can be used in the home — is enteral nutrition (EN), or tube feeding. reprinted or photocopied without prior written permission of copyright owner. All service marks, 29 Advocacy Corner: In Case of a Drop in Cabin Pressure, Put Your Mask trademarks and trade names presented or referred to in this magazine are the property of their respective owners. On First — A Survival Guide for the Caregiver of a Cancer Patient We welcome your comments, stories and suggestions. Please send all correspondence to: In the unsettling atmosphere of cancer, the caregiver is a patient’s lifeline. But to be an effective supporter and advocate, a caregiver must take precautions to stay strong. Read Coram Specialty Infusion Services Celebrate Life about how to take care of yourself as you care for your loved one. 555 17th Street, Suite 1500 Denver, CO 80202 COR09007-0911
- 3. A Note from Our Guest Editor Celebrate Life is a magazine dedicated to providing home nutrition care patients with very practical information and useful tips for managing their condition. It is a great honor to be guest editor of this issue, which focuses on cancer nutrition and includes articles on a variety of related topics. As a gastroenterologist and a medical director of the nutrition and metabolic support team at Cancer Treatment Centers of America (CTCA), I have always had a challenging job of managing severe cancer-associated malnutrition. Over the past two decades, home healthcare services have made big strides in helping my patients with their nutritional needs. With great evidence-based studies, we have shown that aggressive nutritional therapies using TPN and tube feeding can be delivered very efficiently and safely to cancer patients in the comfort of their own homes. I have dedicated the last 17 years to the nutritional needs of patients with advanced cancer. There are still skeptics who are reluctant to consider home nutrition therapy in patients with cancer; however, these numbers are dwindling rapidly. It gives me tremendous professional satisfaction to see the impact of home nutritional therapy on the quality of life of my patients. Therefore, I have included an article in this issue discussing this matter in detail. In another article, Carol Ireton-Jones and Roaxana Tamijani, two well-reputed dietitians, very eloquently discuss the role of healthy eating in preventing cancer. Lifestyle changes including exercise, weight reduction, abstaining from tobacco/alcohol, and eating healthy are important not only for healthy individuals, but also for patients who are under active treatment for cancer. Unfortunately, achieving nutritional well-being can be challenging for patients who are experiencing severe side effects from different modalities of cancer treatments. To address this, Karen Hamilton has written a detailed article that can help you better understand and manage these challenges. Pharmacists play a key role in helping our cancer patients at home. Tiffany Fancher’s article talks about therapies other than TPN and tube feeding that can be provided at home to aid our cancer patients. The role of a caregiver (a family member or a friend) is a vital part of the success of home nutritional care. An article by Linda Gravenstein — a TPN patient advocate — will help you better understand this role. For our tube-feeding patients, Elaine Arthur and Corrie Trottier have provided an in-depth commentary on how to successfully manage the different kinds of feeding tubes and specialized enteral formulas. Nutrition in cancer can be very complex. I am proud to be a contributor to this issue, which addresses the most important challenges for patients today. Enjoy this issue, and as always, we appreciate your feedback. Dr. Pankaj Vashi, MD Lead National Medical Director National Director — Gastroenterology & Nutrition Metabolic Support Cancer Treatment Centers of America at Midwestern Regional Medical Center 3
- 4. Q uality of Life and Nutrition Support for the Cancer Patient By Dr. Pankaj Vashi, MD 4 | Celebrate Life | October 2011, Issue 25
- 5. The definition of quality of life (QOL) is Nutrition Support Options: Enteral different for everyone. But for most people, Nutrition and Parenteral Nutrition the main factor that determines QOL is our An alternate means of nutrition support ability to enjoy everything life has to offer with should be considered in all cancer patients no major health symptoms. For cancer patients, when their oral intake of proteins and calories one factor that can cause health symptoms and drops below 60% of the recommended intake. have a serious impact on QOL is poor nutrition. Early interventions should focus on control For these patients, nutrition support can be an of symptoms (such as pain, nausea, vomiting, effective treatment option. diarrhea and poor appetite). Poor symptom control can have a negative effect on overall Poor Nutrition in Cancer Patients nutrition and QOL. Once the symptoms are Weight loss, loss of appetite, and fatigue with under control, oral supplementation of liquids generalized weakness are seen in more than and powders high in calories and protein should 60% of patients with advanced cancer. These be implemented. If a patient’s digestive tract is symptoms of malnutrition are more pronounced intact and functional, nutritional support with with pancreatic, stomach, lung and colon enteral nutrition (EN), or tube feeding, is always cancers. Malnutrition in cancer patients results preferred. EN can be given through several from multiple factors. Nausea, vomiting and types of feeding tubes: nasogastric, nasojejunal, diarrhea associated with cancer, as well as the gastrostomy or jejunostomy. These tubes are effects of cancer treatments, play a major role. differentiated based on where and how they are Also, cancer cells produce chemicals that can placed in the digestive tract. All commercially cause loss of appetite, weight loss and wasting. available enteral feeding formulas are designed Other factors include infections, surgeries and to deliver adequate amounts of calories, proteins underlying depression. and vitamins. Early detection and aggressive intervention of Unfortunately, a patient’s digestive tract may not malnutrition in cancer patients have been shown work well due to either severe gastrointestinal to have a positive impact on overall recovery and side effects of the cancer therapy, or conditions QOL. Unfortunately, the effect of malnutrition on such as malabsorption syndrome, or bowel QOL is not well recognized. In fact, in spite of very obstruction that cannot be treated surgically. In easy-to-use nutritional evaluation tools available patients with such digestive problems, parenteral to us, many professionals taking care of cancer nutrition (PN), or intravenous nutrition, is the patients don’t diagnose early malnutrition. It only nutrition support option. The role of PN in is not unusual for a physician to come across cancer patients is controversial — studies done a cancer patient who has lost more than 30% over 20 years ago showed a negative impact of of their usual body weight in a short period of PN on overall recovery in home PN patients. This time, whose professional caregivers have not was mainly due to the high incidence of central addressed this weight loss. line infections and metabolic complications. With improved care and better understanding of 5
- 6. related chemical functions in the body, we have Summary been able to significantly reduce many of the Nutrition support cannot cure a patient’s cancer, complications associated with home PN (HPN). but it can enable cancer patients to continue Recent studies on HPN in cancer patients have aggressive cancer treatments and improve shown it to have a positive impact on overall how well they function on a daily basis. QOL recovery and QOL. measurement helps us validate the use of nutrition support, which can be an expensive Tools to Measure Quality of Life therapy. While many studies have shown QOL assessment is a type of measurement that improved QOL in HPN and EN patients, there is can be used in addition to other nutritional need for a large prospective study using one evaluation tools. It helps health professionals of the standardized assessment tools. QOL and the patient to measure the impact of assessment should be routinely used in HPN and home nutritional support on overall well-being, EN patients to help evaluate the impact of such a symptom control, and emotional and functional complex therapy. capacity. Note: Before considering any nutritional There are many easy-to-use and well-validated interventions, it is important for you to discuss the instruments that measure health-related QOL. risks and benefits of nutritional support with your Most of these assessment tools address physical, medical and nutrition team. A team approach social and psychological elements. Some of involving a physician, dietitian, case manager, these tools are: social worker and your home infusion company • SF-36 Physical and Mental Health Summary is crucial for a smooth transition from hospital to home while receiving nutrition support. t Scale: This tool evaluates the physical, social, emotional and mental state of a patient. It is References: the most generic tool used for healthcare- 1. Mackenzie ML, et al. Home parenteral nutrition in advanced cancer: where are we? Appl. Physio. Nut. Met. 2008;33(1):1-11. related QOL evaluation. 2. Baxter JP et al. A review of quality of life of adult patients treated with long- • Karnofsky Performance Scale: This is a very term parenteral nutrition. Clinical Nutrition. 2006;25(4):543-53. 3. Bozzetti et al. Quality of life and length of survival in advanced cancer patients on home parenteral nutrition. Clinical Nutrition. 2002;21(4):269-71. simple and easy-to-use tool. 4. Aaronson NK et al. The European Organization for Research and Treatment • EORTC (European Organization for Research of cancer QLQ-C30: A quality of life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-76. and Treatment of Cancer) QLQ-C 30 Scale: 5. Huisman-de Waal et al. The impact of home parenteral nutrition on daily life — a review. Clinical Nutrition. 2007;26(3):275-88. This scale was developed initially for 6. Soo I et al. Use of parenteral nutrition in patients with advanced cancer. Appl. Physio. Nut. Met. 2008;33(1):102-6. international clinical trials. It is now used in 7. Marin Caro et al. Nutritional intervention and Quality of life in adult oncology many U.S. trials. patients. Clinical Nutrition. 2007;(3):289-301. • HPN–QOL: This tool was designed specifically for HPN patients and introduced last year. It has a 48-item questionnaire that focuses on physical, emotional and symptomatic issues. It is the most recently created tool, but is not widely used in the U.S. 6 | Celebrate Life | October 2011, Issue 25
- 7. Eating Healthy to Help Prevent Cancer: The Role of a Plant-based Diet By Carol Ireton-Jones, PhD, RD, LD, CNSD and Roaxana Tamijani, MS, RD, LD Proper nutrition is about fueling your body to enable it to perform * If you are on enteral nutrition at its highest capacity. Additionally, healthy food choices are a (EN, or tube feeding) or parenteral nutrition (PN, or intravenous key to the prevention of many diseases, including cancer. A plant- nutrition), you may be curious about nutrition for those based diet is a great place to start to benefit from the disease- formulas. When planning EN or PN regimens, your registered fighting abilities of diet. Of course, good nutrition can’t work in dietitian always keeps complete and personalized nutrition top a vacuum — other factors like exercise, avoiding tobacco and of mind. In fact, tube feeding reducing stress also help to decrease disease risk. In this article, we researchers are on the cutting edge of nutrition science and offer suggestions for good food choices. If you receive nutrition ensure optimal nutrient profiles for each formula. Similarly, each support* and are still able to eat foods, review the information PN formulation is developed by the clinician to provide the presented here. Work with your registered dietitian to determine most beneficial calorie, protein, carbohydrate, fat, vitamin and what will fit with your regimen and improve your oral nutrition to mineral content to meet each individual’s needs. best suit your health needs. 7
- 8. A Healthy Meal A Plant-Based Diet for a Plant-Based Diet: According to the American Dietetic Association, • Red beans and brown rice people following vegetarian diets have a significantly • Tossed green salad topped with lower risk of cancer and many other chronic diseases. So, what is a plant-based diet and how does that relate walnuts and strawberries, and olive- oil-and-vinegar dressing to people who like a cheeseburger now and then? A plant-based diet is one that focuses on whole grains, • 8-ounce glass of skim milk legumes (beans, peas and lentils), whole fruits, nuts and seeds, and vegetables as primary food choices. A Healthy Meal for a Plant-Based Diet Non-fat dairy products can be included in this diet to that Includes Animal Protein: provide additional protein. Lean meat, poultry and • Baked salmon fish can be part of a plant-based diet when included in moderation. • Sautéed spinach • Melted lean cheese and mushrooms Here’s a fun activity to practice thinking this way: mixed in whole-grain risotto write down your family’s 16 favorite foods from the • Glass of water plant groups: fruits, vegetables, nuts, seeds, legumes • Dessert of one cup of sliced mango, and whole grains. We recommend that you focus strawberries and blueberries on unprocessed foods. For example, list apples but not sugary applesauce; peanuts but not chocolate- covered peanuts; or boiled potatoes instead of potato chips. How can you incorporate plant foods in your diet? Just use your list! Start with nutrient-rich fruits and vegetables. Try to eat five to nine cups of fruits and vegetables a day (one cup is about the size of your fist). Fruits and vegetables that are in season are the best choices. What is in season where you are? See our website resources at the end of this article. And don’t forget lentils, beans and peas, which can provide a higher amount of protein than other plant foods (see ‘Plant-based Protein’ later in this article). Grains Grains are a great source of fiber and many nutrients. Choose multi-grain breads, whole grain rice and cereal, and try some less common grains like bulgur and quinoa. Steel cut oatmeal is great for its crunchy texture. To reach the recommended goal for fiber of about 25 grams/day, the USDA recommends eating at least three servings of whole grains a day. 8 | Celebrate Life | October 2011, Issue 25
- 9. Fats Nuts and Seeds Fat in the diet makes meals tasty and filling. By Walnuts, peanuts, almonds, pecans, pistachios, making better choices in the types of fats you pumpkin seeds and other nuts and seeds consume, you can also improve your health. provide essential fatty acids and antioxidants For instance, always avoid trans fats, and keep like vitamin E and lutein, which new research saturated fats to a minimum (you can see the fat concludes contribute to a reduced risk of many content of many foods on their ingredient labels). diseases such as cancer and heart disease. It When cooking, many of us now use liquid oil. only takes one ounce to make a serving of these Good choices are olive, canola and grapeseed oil. plant-based meat substitutes. Nuts and seeds are Olive oil can be used in salads or to sauté food, a tasty snack, and are often palate-pleasing when while canola oil is best for baking. incorporated into recipes. For example, green salads topped with sunflower seeds or walnuts, Plant-based Protein or slivered almonds sprinkled over sautéed Plant-based protein from non-meat sources can asparagus, are good ways to eat nuts with meals. provide what you need to maintain nutritional well-being. In fact, there is a strong relationship Supplements between consuming well-done meat, red meat, One question many people ask is: what and cured meat and an increased risk of various supplements should I take to prevent cancer? As cancers. Diets that use only or mostly plant- mentioned above, a key in cancer prevention is based protein tend to have a lower risk of cancer. a healthy, plant-based diet. However, if you also Beans and other legumes are good protein want to take a supplement, taking a multivitamin sources, and have the added benefit of fiber containing 100% of the RDA (recommended and many antioxidants that are associated with daily allowance) of vitamins and minerals is lowering disease risk. Legumes also do not have usually considered safe by most practitioners. the saturated fat and cholesterol that is found in Make sure your multivitamin contains vitamin D meat, making it “heart-healthy.” Legumes often and folate or folic acid. Recently, the Institute of easily replace meat in recipes to add a healthful Medicine’s Food and Nutrition Board increased punch to a meal. Some fabulous legumes and its recommended amounts of vitamin D intake protein sources include: in its proposed new reference values. Check with • Soy beans — Try edamame, soy veggie your doctor or dietitian to determine the vitamin burgers and other meat substitutes, tofu, D level that’s right for you and then supplement tempeh patties and soy milk/yogurt. accordingly. In some cancer treatment protocols, • Beans, peas and lentils — Try these in soups, additional vitamin D is not recommended. salads, pasta dishes and burritos. • Peanuts — Try these in trail mix snacks, A plant-based diet is evidenced to reduce the risk of cancer and other chronic diseases. Using your peanut butter, baking and sauces. plant-based food list and the following Online Health Resources, work with your licensed health practitioner to help you gain an edge on proper nutrition and reduce your risk of cancer and other chronic diseases. 9
- 10. Online Health Resources References 1. American Dietetic Association. Position paper on vegetarian diets. Available at: http://www.eatright.org/About/Content.aspx?id=8357. Accessed 8.22.11. Explore these Internet resources* for cancer 2. American Dietetic Association. Position paper on nutrient supplementation. and nutrition topics, risk calculators, support, Available at: http://www.eatright.org/About/Content.aspx?id=8409. Accessed 8.22.11. volunteer opportunities, research participation 3. MD Anderson Cancer Center. Meat, especially if it’s well-done, may increase risk of bladder cancer. Available at: http://www.mdanderson.org/newsroom/ and more. news-releases/2010/well-done-meat-may-increase-bladder-cancer-risk.html. Accessed 5.31.11. • The National Cancer Institute (NCI): 4. MD Anderson Cancer Center. Red meat consumption linked to colorectal cancer. Available at: http://www.mdanderson.org/newsroom/news- www.cancer.gov releases/2008/red-meat-consumption-linked-to-colorectal-cancer.html. • Accessed 5.31.11. The University of Texas MD Anderson 5. American Dietitic Association. ADA Evidence Analysis Library. Available at: http://www.adaevidencelibrary.com/. Accessed 5.23.11. Cancer Center: 6. Mayo Clinic. Beans and other legumes: types and cooking tips. Available at: http://www.mayoclinic.com/health/legumes/NU00260. Accessed 5.25.11. www.mdanderson.org 7. U.S. Department of Agriculture. SNAP-Ed Connection. Nutrition through the • The Center for Nutrition Policy and seasons. Available at: http://snap.nal.usda.gov/foodstamp/nutrition_seasons. php. Accessed 5.31.11. Promotion, U.S. Department of Agriculture: 8. Institute of Medicine. Dietary reference intakes for calcium and vitamin D. Available at: http://www.iom.edu/Reports/2010/Dietary-Reference-Intakes- www.choosemyplate.gov for-Calcium-and-Vitamin-D.aspx. Accessed 6.2.11. • 9. National Cancer Institute. Vitamin D and cancer prevention: strengths and Mayo Clinic guide to cooking legumes: limits of the evidence. Available at: http://www.cancer.gov/cancertopics/ factsheet/prevention/vitamin-D. Accessed 6.2.11. www.mayoclinic.com/health/legumes/ NU00260 • SNAP-Ed Connection’s “Nutrition Through the Seasons” program on buying and fruits and vegetables in season, from the U.S. Department of Agriculture: http://snap.nal.usda.gov/foodstamp/ nutrition_seasons.php • Institute of Medicine Food and Nutrition Board Report on Vitamin D: www.iom.edu/Reports/2010/Dietary- Reference-Intakes-for-Calcium-and- Vitamin-D.aspx t * Please note that some organizations may charge a fee for access to services. This listing is not an endorsement of these organizations, or information they may disseminate. We strongly suggest you discuss any information you receive from these organizations with a qualified professional before making any changes in your healthcare, insurance coverage or home care provider. 10 | Celebrate Life | October 2011, Issue 25
- 11. Nutrition and Cancer Care: Resource Organizations* American Cancer Society 800.227.2345 www.cancer.org American Dietetic Association 800.877.1600 www.eatright.org American Institute for Cancer Research 800.843.8114 www.aicr.org American Society of Clinical Oncology 888.282.2552 www.asco.org American Society for Parenteral and Enteral Nutrition 800.727.4567 www.nutritioncare.org National Cancer Institute 800.422.6237 www.cancer.gov National Center for Complementary and Alternative Medicine (NCCAM) 888.644.6226 (NCCAM Clearinghouse) www.nccam.nih.gov Office of Dietary Supplements 301.435.2920 www.ods.od.nih.gov Oncology Nursing Society 866.257.4667 www.ons.org * Please note that some organizations may charge a fee for access to services. This listing is not an endorsement of these organizations, or information they may disseminate. We strongly suggest you discuss any information you receive from these organizations with a qualified professional before making any changes in your healthcare, insurance coverage or home care provider. 11
- 12. The Effects of Cancer Therapy on Nutritional Well-Being Nutritional well-being varies for people starting cancer therapy. Some people start therapy with no nutrition problems; others start with a poor appetite, weight loss, and other nutrition-related issues. For the latter, cancer therapies can complicate treatment for nutritional problems. In turn, a patient’s nutritional health can affect his or her ability to tolerate cancer treatment. And both cancer therapy and nutritional health can impact the patient’s expected healing and recovery process. By Karen Hamilton, MS, RD, LD, CNSC 12 | Celebrate Life | October 2011, Issue 25
- 13. The cancer treatments used most often and the amount of healing needed. Nutritional include surgery, chemotherapy, radiation and complications are usually most significant with immunotherapy (cancer medications), each cancers and cancer treatments involving the of which can cause nutrition problems. But gastrointestinal (GI) tract, which extends from no matter what type of cancer therapy they the mouth to the anus. For example, if part undergo, individuals who receive aggressive of the bowel is removed to take out a tumor, a cancer treatment typically need aggressive patient may have trouble absorbing nutrients nutrition management. The key is to identify the for some time (nutrients are absorbed into the need early and provide nutrition support before body through the bowel). The amount of healing an individual becomes too debilitated. affects nutritional well-being because healing often increases energy needs and nutrient If you are receiving cancer therapy, your requirements. healthcare team will assess your baseline nutrition status and evaluate the possible impact Chemotherapy of your cancer treatment on your nutritional There are more than 100 different chemotherapy well-being and vice versa. Then your team will agents approved to treat cancer. Unlike surgery work with you to create a nutrition plan that and radiation therapy, which focus on one part of will help improve or maintain your nutritional the body, chemotherapy is a systemic treatment status as you go through cancer treatment. The (the drug goes throughout the body via the following information can help you anticipate bloodstream). As a result, chemotherapy has and understand nutrition problems as they relate the potential for more nutritional side effects to your cancer therapy. than these other treatments. The most common nutrition-related side effects of chemotherapy Surgery are poor appetite, taste changes, feeling full About 60% of individuals diagnosed with cancer earlier than usual, nausea, vomiting, sore will have some type of cancer-related surgery.1 mouth or throat, diarrhea and constipation. People who are poorly nourished and undergo Poor nutritional well-being and weight loss surgery are at higher risk for post-surgical may prevent a patient from regaining both complications. If the surgery is not urgent, health and acceptable blood counts between nutrition deficiencies should be corrected chemotherapy cycles. This can affect the patient’s beforehand to promote recovery and healing. To ability to stay on treatment schedules, which is do this, nutritional problems should be identified important in achieving a successful outcome. and the best treatment applied. This treatment can include oral liquid supplements, a change in Changes in diet are usually encouraged to best diet, or even tube feeding (enteral nutrition) or manage chemotherapy-related symptoms (see parenteral (intravenous) nutrition. Medications Table 1). Liquid supplements that are high in may be prescribed to enhance appetite, reduce calories and protein may be used to maintain nausea or help make bowel habits normalize. adequate calorie, protein and vitamin intake. Special formulas may be suggested for people After a surgical procedure, nutritional well-being with other medical conditions, such as diabetes is affected by the area of the body operated on or renal failure. 2, 3 13
- 14. symptoms caused Diet changes to consider by cancer Treatment Loss of appetite • Plan a daily menu in advance. • Make every bite count—choose foods high in calories and protein. • Pack snacks to keep on hand throughout the day. • Eat five or six small meals per day. Trouble swallowing • Consider high-calorie, high-protein milkshakes. • Chew food thoroughly. • Choose soft foods. Nausea and vomiting • Avoid foods that are spicy or very sugary, fatty or greasy. • Eat smaller, more frequent meals. • Avoid foods with strong smells, or have someone cook for you at their home to decrease strong odors in your home. • Eat slowly. • Drink beverages between meals, not during meals. • Don’t lie down right after a meal. • Rinse your mouth with lemon water after eating. • Try eating your meals when they are at room temperature. • Try distractions like watching TV during meals. Diarrhea • Avoid spicy, fatty or greasy foods. • Avoid foods high in insoluble fiber, such as raw fruit and vegetables, and coarse whole grains. • Avoid drinks that contain caffeine. • Try lactose-free or lactose-limited milk products. • Eat more foods containing soluble fiber, such as white rice, bananas, oatmeal, mashed potatoes and applesauce. • Drink plenty of fluids. Constipation • Eat more foods containing insoluble fiber, such as fresh fruits and vegetables and whole grains. • Drink plenty of fluids. Dry mouth • Practice good mouth care. Try a swish-and-spit solution of a ½-teaspoon of salt or baking soda with a glass of water five times daily. • Talk to your doctor about artificial saliva. • Avoid oral care products that contain peroxide or alcohol; these ingredients will dry your mouth. • Try sucking on mints or lemon hard candy. Sugarless gum may also be helpful. Mouth sores • Try soft or pureed food, or a liquid diet. • Avoid citrus or tomato-based foods. • Consider high-calorie, high-protein supplements. Taste changes • Try sucking on mints or lemon hard candy to keep your mouth tasting fresh. • Use plastic utensils. • Use herbs, seasonings and marinades in your cooking to increase food’s flavor. Table 1 Following a Healthy Diet It is important to maintain a healthy diet while receiving cancer therapy. Getting appropriate vitamins and nutrients can help your body cope with the stresses of treatment. Also, During Cancer Therapy by maintaining your calorie intake, it can help prevent or reduce weight loss. Here are some diet pointers for adults: 14 | Celebrate Life | October 2011, Issue 25
- 15. Radiation Therapy Nutrition management can help ease radiation Due to damage it can cause to cells in the side effects. A study of patients with colorectal digestive system, radiation therapy can make cancer receiving radiation therapy showed it harder to eat, and impair digestion and that dietary counseling can improve patients’ absorption of nutrients. Most side effects begin nutritional intake, status and quality of life.9 around the second or third week of treatment Many patients undergoing radiation therapy and dissipate two or three weeks after radiation can benefit from nutritional supplements therapy is completed. However, some side between meals. And if patients can’t eat enough effects can occur or continue long-term after to maintain their weight, aggressive nutritional treatment has been completed. 4, 5 Radiation side support can be considered, such as tube effects depend on the total dose of radiation, feeding or parenteral nutrition. Tube feedings the amount and length of time that radiation are usually well tolerated and are cost-effective. treatments are received, and on the area treated. Numerous studies demonstrate the benefit of • Radiation to the head and neck: Some of tube feedings begun at the onset of treatment (specifically treatment to head and neck regions) the more common side effects include taste changes, pain or trouble with swallowing, before significant weight loss has occurred.10 If dry mouth, thick saliva, and narrowing of tube feedings can’t be tolerated, TPN should be the upper esophagus (food tube). Patients considered. receiving radiation therapy to this region may have preexisting malnutrition because Immunotherapy they simply cannot take in enough food Immunotherapy medications include mono- due to chewing or swallowing issues. clonal antibodies, which are used to slow the • Radiation to the chest: Possible side growth of cancer cells; interferon, a common effects include a sore, inflamed esophagus, cancer drug; Interleukin-2, which is used to treat trouble swallowing, and esophageal reflux metastatic (spreading) renal cell cancer; and (when stomach contents back up into the granulocyte-macrophage colony-stimulating esophagus). factor, a common therapy used to increase the • Radiation to the pelvis or abdomen: production of white blood cells. Some of the Diarrhea, nausea, vomiting, enteritis more common side effects of these types of (infection of the small intestine), and drugs include fever, fatigue, weight gain, nausea, malabsorption of nutrients are possible vomiting and diarrhea, and loss of appetite. side effects. • Each day, try to eat at least seven servings of fruits and • Remove excess fats, sugars and salt from your diet. This vegetables, six servings of grain products, around six or is also beneficial because these items tend to be low in seven ounces of low-fat meat or fish, and three servings nutrients. of low-fat dairy products. • If you simply don’t have an appetite, consider eating • Drink plenty of nonalcoholic or non-caffeinated smaller “snack size” meals more frequently. Grazing, or beverages every day — about eight to ten eight-ounce eating six to eight small meals per day, may prevent you glasses per day. from feeling over-full or losing weight. 15 15
- 16. If ignored, and if severe, these symptoms can cause gradual or drastic weight loss, which may cancer Types with the Most significant lead to malnutrition. t Impact on Nutritional Well-being Head and Neck Cancers References 1. American Cancer Society website. Available at: www.cancer.org. Accessed • Parts of the body affected: The mouth, tongue, jaw, brain, April 11, 2011. eye and esophagus. • 2. Eldridge B. Chemotherapy and nutrition implications. McCallum PD, Polisena CG, eds.: The Clinical Guide to Oncology Nutrition. Chicago: The American Side effects of treatments: Reduced ability to speak, chew, Dietetic Association;2000:61-9. 3. Fishman M, Mrozek-Orlowski M, eds. Cancer Chemotherapy Guidelines swallow, smell and/or taste. and Recommendations for Practice. 2nd ed. Pittsburgh: Oncology Nursing Press;1999. • Treatment considerations: Many individuals with head and 4. Donaldson SS. Nutritional consequences of radiotherapy. Cancer Res. 1977 neck cancer are poorly nourished at the time of diagnosis. Jul;37(7 Pt 2):2407-13. 5. Unsal D, Mentes B, Akmansu M, et al. Evaluation of nutritional status in cancer This is partly because prior to surgery, they may undergo patients receiving radiotherapy: a prospective study. Am J Clin Oncol. 2006 Apr;29(2):183-8. chemotherapy or radiation therapy to shrink their tumors. 6. Chencharick JD, Mossman KL. Nutritional consequences of the radiotherapy These treatments can cause nutrition problems because they of head and neck cancer. Cancer. 1983 Mar 1;51(5):811-5. 7. McQuellon RP, Moose DB, Russell GB, et al.: Supportive use of megestrol reduce the patients’ ability to eat by causing mouth sores, acetate (Megace) with head/neck and lung cancer patients receiving radiation taste changes and pain. Many of these individuals benefit therapy. Int J Radiat Oncol Biol Phys. 2002 Apr 1;52(5):1180-5. 8. Polisena CG. Nutrition concerns with the radiation therapy patient. In: from feeding tube placement before surgery. This puts them McCallum PD, Polisena CG, eds.: The Clinical Guide to Oncology Nutrition. Chicago: The American Dietetic Association; 2000:70-8. in better shape to recover from surgery and supports them 9. Ravasco P, Monteiro-Grillo I, Vidal PM, et al.: Dietary counseling improves nutritionally afterward, with the goal of eventually taking an patient outcomes: a prospective, randomized, controlled trial in colorectal cancer patients undergoing radiotherapy. J Clin Oncol. 2005 Mar 1;23(7): oral diet. Medications may also help.* 1431-8. 10. Tyldesley S, Sheehan F, Munk P, et al.: The use of radiologically placed gastrostomy tubes in head and neck cancer patients receiving radiotherapy. Gastrointestinal (GI) Cancers Int J Radiat Oncol Biol Phys. 1996 Dec 1;36(5):1205-9. • Parts of the body affected: The lower esophagus, stomach, pancreas, liver, gallbladder, bile duct, and small and large intestine. • Side effects of treatments: Gastroparesis (paralyzed stomach that can’t easily push food into the small bowel), changes in digestion, poor absorption of nutrients, poorly controlled blood sugar, elevated lipid levels, fluid and electrolyte imbalance, bowel leak at the surgical site, dumping syndrome (too rapid processing of food by the body, preventing absorption), and vitamin and mineral deficiencies. • Treatment considerations: Surgery for GI cancer may take a tremendous toll on the body, but it can improve overall chances of survival. The use of tube feeding is common in the treatment of GI cancers. In cases where feeding tubes cannot be placed, or intolerance to tube feeding is noted (such as with persistent nausea, vomiting or diarrhea), parenteral nutrition can be provided. * In one study, head and neck cancer patients who received both megestrol acetate to aid in stimulating appetite, and education on diet modifications, were able to maintain their weight and reported a higher quality of life than those who did not receive any diet interventions. 6,7 16 | Celebrate Life | October 2011, Issue 25
- 17. Informational Teleconference Series Managing Stress During the Holidays Social and emotional coping skills for the holiday season. NoV 15, 2011 — 7:00 pm eastern / 4:00 pm Pacific • Toll-free 866.418.5399 • Passcode 3036728726 (when prompted) Featured Speakers: Linda gravenstein, Consumer Advocate, Coram Mary Patnode, MS, ed, LP, TPN Linda Gravenstein Mary Patnode Consumer and Vice President, Oley Foundation Board of Trustees “Managing Stress During the Holidays” is part of this free, informational teleconference series. The “Small Steps to Big Steps” series is a great way to learn about topics that affect nutrition consumers from the comfort of your own home. Missed a Call? If you’ve missed a call, don’t worry! You can still listen to it online at WeNourish.com/consumers/events.aspx. 17
- 18. Home Care Therapies for Cancer Patients by Tiffany Fancher, PharmD Cancer rates continue to rise in the U.S., but at the same time, treatment options have grown by leaps and bounds. Home care is one of those treatment options. A company that offers comprehensive home care services can provide the equipment and training needed for patients of all ages with all types of cancers to receive care at home. If you are a cancer patient, home care can allow you to remain in the comfort of your own home with your family and friends close by. Receiving care at home not only improves your quality of life, it also reduces your risk of developing hospital-acquired infections, and reduces costs. The primary goals of cancer home care are to keep patients comfortable, and to avoid hospitalization. Experienced, highly trained home care clinicians can work one-on-one with your oncologists to provide the individualized care needed to meet these goals. Home care therapy options for cancer patients may include hydration/fluids, nausea and vomiting medications, pain management therapies, antibiotics, growth factor therapy, and even chemotherapy. 18 | Celebrate Life | October 2011, Issue 25
- 19. Hydration Therapy Antibiotic Therapy Dehydration occurs when the body does not In patients receiving chemotherapy or radiation, have enough water and other fluids to carry out the cells that fight off infection are often reduced, its normal function. This can happen when more leaving the body more prone to illness. To make fluids are lost than are taken in. Dehydration up for the loss of these cells, antibiotics and may be classified as mild, moderate or severe. antifungals can be used to help rid the body of Anyone can become dehydrated, but people infections, and many of these medications can with certain symptoms are more likely to do be administered in the home. The reduced risk so. These symptoms, which include intense of hospital-acquired infections that home care vomiting, diarrhea, fever, and excessive sweating, provides is especially important in these patients are common in cancer patients. Intravenous with already reduced immune function. (IV) hydration/fluid can be given to patients in the home to help return the body to its normal Growth Factor Therapy function. Growth factor therapy, a treatment that stimulates cell growth, can be given at home Nausea/Vomiting Therapy to help the body fight off infections and help Nausea and vomiting are side effects seen with bring the immune system back up to its normal some cancer medications, such as chemotherapy. function. This treatment is typically given 24 hours If they are severe enough, a patient may become to 14 days after a patient receives chemotherapy. dehydrated and the body will not be able to Under the direction of their physician, patients function normally. The first step in treating can be taught by trained nurses to administer nausea and vomiting is to “break” the cycle as growth factor medications. quickly as possible. Many medications are used to control nausea and vomiting, and patients may require several medication changes during the Chemotherapy course of therapy in order to find the best drug to In addition to these treatments, even some stop the problem. In the home, this may involve a chemotherapy can be given in the home. This combination of oral, rectal and/or IV medications can be very convenient for a patient, who can to make the individual comfortable. Trained cut down on the number of trips made to the home care clinicians will help to determine if hospital to receive cancer treatments. However, the patient’s nausea and vomiting are being the home infusion company must take extreme appropriately treated. precautions to ensure that the patient, the patient’s family, and the nursing staff are well- protected and able to give chemotherapy safely. Pain Management Therapy Cancer and cancer treatments can be very painful, and difficult for patients to tolerate. Note: If you are having any of these treatments, Pain medications can be given in the home any concerns you have should be discussed openly in different forms, routes, and schedules — with your home care clinician or physician. Also, even around-the-clock — to keep the patient cancer treatments can have many side effects that comfortable. Equipment can even be set up to may be difficult to manage. It is important to have give additional medication if the patient’s pain trained clinicians available around-the-clock to suddenly increases. help alleviate these difficulties. t References: The Mayo Clinic. Available at: www.mayoclinic.com/health/dehydration/DS00561. Accessed 8.24.11; Coram Policy and Procedures 19
- 20. 20 | Celebrate Life | October 2011, Issue 25
- 21. My Great Adventure By Michelle Barford Sometimes nutrition support is short-term and uneventful — and sometimes it is anything but! With a positive attitude and a sense of humor, Michelle Barford, a Coram nutrition support patient, shares her dramatic story. Quite simply, the last three years have been was. Oh my goodness — we had never been an amazing journey that has tested my inner asked that before! The doctor was quite upset strength as well as the very core of my being. It and said that as a hospice patient, especially with started on March 2, 2008, a date that, for me, will all of my hospital admissions and near-death “live in infamy.” My husband, Mark — my very episodes, I should have been counseled on my best friend and loudest cheerleader — took me end-of-life directives and choices. I remember to the ER after I experienced severe abdominal clearly stating to him that this was NOT the end pain for 36 hours. I remained in the hospital for of my life — that the end would not happen for a over three months, undergoing two abdominal long, long time. I expected to be treated and kept surgeries, the last of which caused complications alive to fight another day! At that point, it hit me that resulted in the development of two fistulas1 that no matter how bad things seemed, it sure that made their way through to my skin. I also beat the alternative. I was still on the right side of received a diagnosis of carcinoid, a rare form of the grass. cancer. I thought this could not be happening to me, but the looks on the faces of my family and Keeping a Sense of Humor friends made me realize it was. I entered hospice,2 Throughout this whole ordeal, I’ve tried to keep had a PICC line3 placed in my arm, and was put a positive attitude. One day, my daughter Caitlin on pre-mixed IV nutrition solution (not one that and I went to the grocery store. I had a huge leak was customized to my needs, as for TPN).4 In my with the “girls” — what I called the fistulas. I told former life, I had been a hospice nurse. Never Caitlin, “To heck with this! I don’t care if I drip all would I have thought the word “hospice” could the way home. I am going to finish shopping! be associated with me as a patient. I already have the biggest butt in the store because of all the padding I’m wearing [to absorb I don’t remember much of the rest of that year, the leakage]. If it’s also wet, we’ll just add it except for having multiple episodes of sepsis5 to the long list of ‘silly Mom events’ that we and changes in the PICC location. There were relish telling everyone about!” times when the pain was constant. The drugs I was taking to control it made things confusing, From then on, the kids and I no longer and the fistulas would not stop leaking. In my looked at my illness with sad eyes. most private moments, I thought death wouldn’t Instead, we had races through the be such a bad thing. grocery store with the motorized carts. Or, we asked where the But then, during one of my many ER visits, one bathroom was in whatever store of the doctors asked me what my “DNR” 6 status we were in, and then went in 21
- 22. Glossary 1. Fistula: An abnormal passageway between two organs in the body. For example, an opening (wound) in the skin that connects to one or and out a dozen times, trip, but upon my return, I promptly more internal organs. watching the faces developed another bout of sepsis. This 2. Hospice: Palliative care (includes of the clerks as they time, my oncologist said we needed pain and symptom management, but not other medical care) for wondered what could to get it under control, and the only individuals who have a life- possibly be causing way to do that was through surgery threatening illness and a life this many trips to the to repair the fistulas and cut out the expectancy of less than six months. restroom. carcinoid. He found a doctor at MD 3. PICC line: A central venous access Anderson Cancer Center who was device that is placed in a vein in the arm. The catheter (tube) I also decided to name the willing to consult with us. We drove to is threaded up the vein into the two lumens7 of the PICC Houston, Texas, and for the first time in superior vena cava (a major blood line. I called them “Jack” and almost a year, I was hopeful. vessel in the chest). “Ginger,” because Jack Daniels 4. TPN (total parenteral nutrition): and ginger ale used to be my favorite In March 2009, I underwent three Nutrition solution that is sent through an IV (intravenous) into drink. I hadn’t had one in a long time, as surgeries to remove the carcinoid and the bloodstream. TPN provides alcohol generally aggravated the “girls.” repair my remaining intestines. The nutrition by bypassing the usual This was my way of staying connected surgeons removed a lot of tissue: all but digestive route. to a former indulgence that I could 125 mm of small intestine, 20% of the 5. Sepsis: An infection in the hopefully resume someday. large intestine, and the mid-abdominal bloodstream. Sepsis can be life- threatening. muscle where the fistulas were located. 6. DNR: Do not resuscitate. This is an Symptoms & Treatments In place of the muscle, they used order a patient can request when Continue pig tissue to stabilize my abdomen. I he or she does not want to receive Meanwhile, my oncologist continued would have only that tissue and my life-saving care during a medical skin protecting my internal organs. I emergency. his quest for information on carcinoid. 7. Lumen: A port of entry where I was his second patient with this also no longer had my belly button. medication and nutrition are diagnosis, so he had gotten up They couldn’t save it because of the hooked up to the central venous to speed on this rare, destructive fistulas. In addition to all of this, I had catheter. cancer. He wasn’t convinced that I a colostomy.8 I had thought I was done 8. Colostomy: A surgical operation with pouches and leakage, but the during which part of the colon was terminal because of the cancer, (large intestine) is diverted to an but was concerned because I kept doctor said the colostomy was needed artificial opening in the abdominal getting septic. My general health was because of the “short gut” 9 I would wall. This is done to bypass a declining due to the huge output likely develop. He assured me that the damaged part of the colon. After a colostomy could be reversed at any colostomy, a bag is worn outside of from the fistulas. I had continued pain. the body to carry waste. And CT scans showed sporadic partial time. He also said it would take about 9. Short gut: The reduced ability obstructions in my intestines. six months for my remaining small of the small bowel (intestine) intestine to adjust to its new length, at to absorb nutrients. Short gut Despite all of this, I decided to go which time the colostomy bag would is caused by bowel damage or no longer be needed. To help keep a significant small bowel removal. to upstate New York over Christmas sense of humor about the colostomy, I 10. Hickman catheter: A central venous with Mark and the kids. I thought this catheter that is placed in the chest would be my last visit to see all my decided to name it. And with a name wall and tunneled under the skin. brothers and sisters. My doctor was for it, in case I was out in public and It has a smaller amount of tubing very concerned about allowing me had an emergency, I could simply say that exits the body and is more “so and so needs attention.” So, “Edgar” easily concealed than a PICC line. A to go out of town, but sent me on my Hickman catheter is used for long- way with IV antibiotics. I survived the was born! term therapy. 11. The Oley Foundation: A nonprofit organization that provides information and support to patients 22 | Celebrate Life | October 2011, Issue 25 receiving nutrition support. oley.org
- 23. In May, I finally returned home. I was no longer I asked what he would do if he did operate again, on hospice, and was referred to Coram for home and he described a slightly different procedure. TPN management. Five months after I got home, He ended the conversation restating that unless my worst fears were once again realized — I I was in a life-threatening situation, he would not had another fistula. But this time it wasn’t going re-operate. through my abdominal wall out of my body; it was leaking into my abdominal cavity. The Three weeks later, I had an episode of sepsis that doctors at MD Anderson tried to repair it through landed me back in this surgeon’s office. At that non-surgical means, but nothing worked. My point, he said he would do the surgery! I was surgeon was adamant that I could not have scheduled for the following week, and when I another abdominal surgery. I could not believe woke up after the procedure, the surgeon came my bad luck. Besides the leaking colostomy, I also in with a big grin on his face. He explained that had an open, draining hole again that required he had gone hunting for the fistula this time and six to eight dressing changes a day. This was a lot found an errant suture stuck in the intestine. He to deal with. had cut it out, applied the plasma gel and started to close me up but thought, where was the cavity A Chance Meeting where all the drainage collected? He had then In February 2010, while I was at a Special made a longer incision, lifted a flap, and there Olympics event for my son, I saw a woman across it was — a collection of gunk the size of a small the gym who looked familiar. When she walked pancake. He had cleaned it all out and closed me past me I asked, “Do I know you?” When I told her up. He said I shouldn’t have any more problems my name, she gasped. She said she had been because he had fixed it all this time. After he left, I one of my nurses at the beginning of all of this, started to cry. I told my husband that angels were and that I was the sickest patient she had ever watching over me and brought that nurse to nursed. Because she’d moved away, she had me back in February. Without her I would never sometimes wondered what had become of me have gotten this surgeon’s name and had this — she hadn’t thought I would live this long! She opportunity for healing. What a blessing. told me that while she was caring for me, she had wanted to share with me the name of another In November 2010, I had not had a septic surgeon but had been unable to. So she gave me infection for 6 months and my doctor said it was the surgeon’s name, and two weeks later, when I okay for me to have a Hickman catheter10 placed. was in the hospital again with a severe infection, I was so excited! No more arm I asked my oncologist to consult with that tangles and dangling lines — I surgeon. The next day the surgeon came in and could hide the central line examined me. He said he thought he could help under my clothes. Things me, and I was scheduled for surgery the next day! were looking up. During the operation, he couldn’t find where the fistula actually was, but he applied plasma gel (a My Life Now type of surgical glue) to the intestine, and closed In the spring of 2011, everything me up. We were all so excited! But two months was going so well that my later, the abscess reappeared. I went back to see husband and I decided I could the surgeon, and he said that I was too high-risk do a “tag-a-long” on his business to try surgery again and he had done all he could. trip to Australia, Singapore and 23
- 24. up g stand- Michelle and her husband in enjoyin oon . Michelle y aftern Michelle and her husband at front of the Sydney Opera House . a Sunda the beach in Australia. paddling on Hong Kong. I contacted customs in the various me confirmation from the airline that I would be countries to find out if there were any restrictions allowed to check as many bags as I needed — or policies regarding bringing in all the medical and she said I was to go and have fun! She also supplies and oral medications I would need. told me about the Oley Foundation,11 which I Australia proved to be the most troublesome googled, and I decided to contact them when I country. I needed permits for the heparin and returned. Off we went to Australia and beyond! I had to have doctors’ orders, copies of all of the original prescriptions, and stated reasons Through It All… for everything I was taking both orally and My family and friends have been and continue to intravenously. This involved three doctors, two be fantastic! People I don’t even know have met pharmacies and Coram. weekly to pray for me and I firmly believe that because of all these prayers, I have lived to tell A week before we were set to leave, the airline this story. I am so grateful for the encouragement informed me that I couldn’t take my TPN on the I’ve been given and for all the help I continue plane as checked baggage. It all had to go on to receive. My doctors and their staff really care as carry-on luggage. I called the airline and was about me and do everything in their power to told that this was not going to be possible. After I ensure that I get the care I need. I joke with one hung up the phone, I started yelling in frustration of the nurse practitioners who saw me early to no one in particular — how could this be on. He described me at one time as “appearing happening? I had planned this meticulously for chronically ill.” I don’t look that way anymore. In four months! My registered dietitian at Coram fact, when he saw me after an extended lapse of called and listened to my ranting, and then time, he did a double take! I’ve grown to accept calmly said she would contact some people and Edgar (but don’t tell him that). And as for “Jack” get this straightened out. Then I was called by and “Ginger,” I never did reacquire my taste for my new best friend, Linda Gravenstein, a Coram Jack Daniels — I’ve moved on to Long Island Consumer Advocate and mother of a lifetime iced tea! Overall, it could be a lot worse. As I’ve TPN consumer. She said she would get me said, it sure beats the alternative. I’m grateful to on board all the airplanes with my supplies as continue to be on the right side of the grass. t checked luggage. Not to worry! And I didn’t (well, maybe a little bit!). Sure enough, Linda emailed 24 | Celebrate Life | October 2011, Issue 25
- 25. Tube Feeding: A Smart Weapon Against cancer-Related Malnutrition By Elaine Arthur, RD and Corrie Trottier, MS, RD, LD/N Studies have shown that patients diagnosed with cancer experience a good quality of life when they are able to maintain their nutritional well-being. 25 25
- 26. Being diagnosed with cancer can be overwhelming. If you have cancer, you know that there are many decisions to be made about anti-cancer treatment, and things to consider about the impact the disease and treatments will have on your quality of life. There is good news, though. Many studies have Table 1: Formula Options for Tube Feeding demonstrated that patients diagnosed with Formula Type Description cancer experience a good quality of life when they Intact Protein: Standard formula type; meets the needs Milk and/or soy protein- of most patients. Higher-calorie formulas are able to maintain their nutritional well-being. based can provide nutrition in smaller volumes of However, to stay healthy nutritionally, you need to formula. Hydrolyzed Protein: Designed for patients who do not absorb have weapons ready to do battle against cancer- Predigested milk protein standard formulas well enough. Higher- related malnutrition. One such weapon that may calorie formulas are available to meet needs in smaller volume. work for you, and which can be used in the home, Disease-Specific: Designed for patients with diabetes, renal is enteral nutrition (EN), or tube feeding. Milk and/or soy failure and lung disease who have failed or protein-based cannot use a standard formula. Hypoallergenic: Designed for patients with food allergies. Causes of Cancer-Related Amino acid-based Malnutrition Modulars: Include powder and liquid additives to Fat, carbohydrate or protein provide additional calories and protein for Malnutrition — when the body doesn’t have the additives patients who cannot meet their needs with nutrients it needs to function properly — can be formula alone. caused both by cancer and cancer treatments. to take in enough protein and calories from the Cancers that affect the gastrointestinal (GI) tract time you are diagnosed with cancer, through your generally cause the most nutrition problems. But treatment and recovery. This is key because during anti-cancer treatments for all types of cancer can cancer treatment, your energy needs are higher make it hard to eat and drink. For instance, about than when you’re healthy. Healthy people typically two weeks after radiation therapy, you may have need to take in about 1,800 to 2,300 calories. loss of appetite, nausea, dry mouth, and a change Protein needs are between 60 and 75 grams per in taste perception; it may even become hard to day. For people under cancer treatment, their swallow. Chemotherapy can produce side effects calorie and protein needs vary, depending on such as nausea and vomiting, which can make things such as their nutritional status before they you lose fluids, and perhaps lead to dehydration. were diagnosed, the type of cancer they have, and Surgery can affect swallowing, digestion and the method of treatment they are undergoing. For absorption of food. example, cancer patients who are underweight need between 2,300 and 2,600 calories every Cancer and Nutrition Needs day. For cancer patients with wounds or who are The first step in gaining or maintaining nutritional protein-deficient, between 100 and 150 grams health while treating cancer is to follow a healthy of protein are needed to help with healing and diet. Good nutrition helps you maintain your replenishing protein stores. weight and recover better. It is very important 26 | Celebrate Life | October 2011, Issue 25
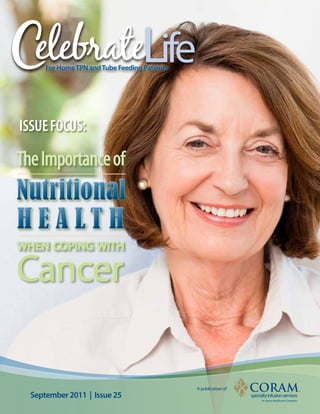
- 27. These nutrition needs apply whether or not you can eat food. Eating can be a battle when you’re not feeling well, but there are ways to make it Nasogastric Tube easier — you’ll find some of these ways in this issue’s article The Effects of Cancer Therapy on Nutritional Well-Being. But if you are unable to get enough nutrition from eating foods, or if you Esophagus simply can’t take in an oral diet without discomfort, tube feeding may be your next step. Stomach Gastrostomy Tube Types of Feeding Tubes Three types of feeding tubes are available. Your Jejunostomy Tube physician will help determine which type best Jejunum meets your needs. • A nasogastric tube (NG tube) can be used Large intestine Small intestine for temporary enteral support. This small, Different types of feeding tubes and their placement flexible tube goes in through the nose and passes down the esophagus into the • A jejunostomy tube (J-tube) is used for stomach. The tube is taped to the side of the patients who need a feeding tube to be patient’s face for comfort and to help keep placed into their small intestine. A J-tube the tube in place. Formula can be infused may also be placed surgically. A J-tube through an NG tube by any of the methods comes with a pump to deliver the formula. described in Table 2. • A gastrostomy tube (G-tube) is a more Tube Feeding at Home permanent feeding tube, typically used Using tube feeding at home may seem daunting, when tube feeding is needed for more than but your medical team will help you. The goal a month. A G-tube, which feeds into the of enteral support is to nourish the body, and stomach, is usually placed during surgery. your medical team will help make tube feeding A short section of the tube hangs out of the fit into your life as smoothly as possible. You will abdomen and can be taped off to the side be taught all aspects of tube feeding, including when not in use. A low-profile G-tube is one how to prepare your formula, how to clean the that is used for active patients on long-term tube site, and how to flush and take care of the enteral therapy. It does not extend beyond tube. Your medical team will also train you to be the abdomen’s surface and so does not safe with your equipment. For instance, you’ll need to be taped in place. Any method of learn how to move an IV pole safely around the formula delivery or infusion can be used house, avoiding tripping hazards such as area with a G-tube. rugs. You’ll also learn to store formula properly to avoid freezing or spoilage. For additional information about tube feeding, be sure to 27
- 28. visit our Nourish™ Nutrition Support Program’s transition. They’ll help make sure you can take in website at WeNourish.com. The site contains enough nutrients and fluids. They may suggest a wealth of information for both patients and keeping a food diary to help you track your caregivers. intake. Gradually you will advance to pureed foods, then to soft foods, and finally to solid Transitioning Back to Eating foods. A registered dietitian can help design a During your cancer treatment or afterward, you diet that works best for you and help make sure may move back from tube feeding to an oral you are eating healthily and gaining the right diet. Your medical team will help you with this amount of weight. t Table 2: Tube Feeding Method Options Method equipment Needed Description Technology/Knowledge Needed cost Bolus Formula, syringes Using a syringe, the patient first flushes the feeding tube May require some level of dexterity $ with water and then pours each dose of formula through (physical coordination). Mimics meal an open catheter-tip syringe. The formula is pushed in over schedule. Portable. 20 minutes and then the tube needs to be flushed again with water. Meal spacing is every 3-4 hours. Gravity Formula, syringes, IV pole, Using a syringe, the patient flushes the feeding tube with This method requires less dexterity. $$ gravity bags water, and then fills the gravity bag with a dose of formula Has a slower rate of feed without and connects it to the feeding tube. When a clamp is the need for a pump. Mimics a meal opened, the formula infuses by gravity over 40 minutes. schedule. After disconnecting, the patient again flushes the tube with water. The bag needs to be rinsed between uses. Meal spacing is every 3-4 hours. Pump Formula, syringes, IV pole, Using a syringe, the patient flushes the feeding tube with Easy to program, although some $$$ enteral pump with a carrying water, and then connects it to the pump set and fills the math may be needed to program the case pump set with the formula. The pump infuses the formula pump correctly. at a controlled rate for a specified amount of time. Some patients need intermittent doses throughout the day, some do better with a set cycle of therapy for part of the day, and some patients do best with continuous therapy 24 hours/ day. The patient does need to flush the tube with water on a schedule to meet their fluid needs and keep the tube from blocking off. Reference: National Institutes of Health, Medline Plus. Available at: www.nlm.nih.gov/medlineplus/ency/article/001042.htm. Accessed 8.24.11. 28 | Celebrate Life | October 2011, Issue 25
- 29. Corner By Linda Gravenstein, Consumer Advocate In Case of a Drop in Cabin Pressure, Put Your Mask On First: A Survival guide for the caregiver of a cancer Patient There are few diagnoses scarier than cancer. The possibility of toxic treatments, surgeries, depression, and unknown outcomes can be terrifying for the patient and family. In this unsettling atmosphere, the caregiver is a patient’s lifeline. A caregiver is a friend or family member who Get help with housework. cares for the patient, often helping to administer If you don’t have time to clean your loved one’s treatment and always providing emotional home, don’t be tempted to tell your loved one support. To be an effective supporter and that it can wait. Imagine being unable to leave advocate, a caregiver must take precautions to your house because of fatigue or nausea and stay strong. Airlines recognize the importance just watching the dust pile up around you — of caring for the caregiver; if you’ve ever flown, but not having the energy to do anything about you’ve probably heard the common safety it! There is a non-profit organization with over refrain reminding passengers that if the need for 547 partners that provide cleaning services oxygen arises, they should always put their own for cancer patients going through treatment. mask on first before helping someone else with Cleaning for a Reason requires only a letter from theirs. This translates to: If you are a caregiver, the treating doctor; applying is simple and the you have to take care of yourself first. In the case services are donated. For more information, visit of a cancer diagnosis, caregivers must be able cleaningforareason.org. to keep a healthy reserve of energy, positive attitude, time and money so that both the Accept help from friends. caregiver and their loved one can survive the Being the caregiver of a cancer patient can be rollercoaster of emotions that come with cancer rewarding, empowering and satisfying. At the testing and treatment. same time, it can be exhausting, depressing and expensive. You must recognize the toll it takes Following are some tips for taking care of yourself on you and seek appropriate help. For instance, as you care for your loved one. Every tip I share many caregivers are the main source of income here comes from personal experience or from for the patient. Taking time off from work can other caregivers that have been gracious enough jeopardize insurance benefits and household to share their journey. income. Accepting help is a must. 29