4. INCIDENCE
Also called tic douloureax
Uncommon cranial nerve disorder
More common in women @ 50-60 years
of age – 3:2 ratio.
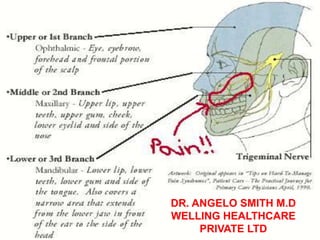
Trigeminal nerve is 5th cranial nerve
(CNV)
And has both motor and sensory
branches; mostly maxillary and
mandibular branches involved.
6. Causal Factors
Initiating pathologic events
include:
nerve compression by tortuous
arteries of the posterior fossa
blood vessels
demyelinating plaques
herpes virus infection
infection of teeth and jaw
7. Pathophysiology
Classical (idiopathic) form
There is no known cause for the, however, studies
point to an underlying vascular pathology as a cause
by irritation over the trigeminal (Gasserian) ganglion.
Age of onset – 52 – 58 yrs
Symptomatic (secondary) form,
There are known common causes affecting the CNV
Compression of the trigeminal ganglion
Demyelinating Disorder (axonal hyper excitability)
Age of onset – 30 – 35 yrs
8. Compression of the Trigeminal
Ganglion
Vascular
Tortous atherosclerotic branch of the
basilar artery
Basilar artery aneurysm
Cerebello-Pontine Angle (CPA) Mass
Meningioma
Chordoma
Neurinoma
Metastatic (nasopharyngeal Ca)
9. Demyelinating Disorder #2
(axonal hyperexcitability)
Multiple sclerosis (MS) – plaques
at the nerve root entry
After nerve injury
Post-trauma
Post-dental procedure
Post-mandibular trauma
11. Clinical manifestations
Abrupt onset with excruciating pain!!
Pain described as burning, knifelike, or
lighting like shock in the lips, upper or
lower gums, cheek, forehead, or side of
the nose.
Patient may twitch, grimace, frequent
blinking and tearing of eye (tic) may
occur.
Affects the face near the nose or mouth
(trigger points)
12.
13. Clinical manifestations
Attacks may be brief (2 or 3 minutes)
Unilateral
Episodes may be initiated by triggering
mechanism of light cutaneous stimulation as a
specific point (trigger zone) along nerve
branches.
With no demonstrable sensory nor motor deficits
Attacks may be restricted to 1 or 2 divisions of the
trigeminal nerve
Usually involves the 2nd branch (maxillary)
and/or 3rd branch (mandibular) division.
14. Precipitating stimuli
Chewing, brushing teeth, hot or
cold blast of air on the face,
washing the face, yawning, or
talking.
Patient may eat improperly,
neglect hygiene practices, wear
cloth over face, withdraw from
interaction with others.
18. Diagnostic studies
Need to rule out other
neurological causes of facial and
cephalic pain.
CT scan will rule out brain lesions,
vascular malformations. LP and
MRI will r/o MS.
There is no specific diagnostic
test for TN.
20. Therapeutic Options
Pharmacologic
Antiepileptic drugs
Anticonvulsant drugs have been used in
the management of pain since the
1960s and the clinical impression is that
they are useful for chronic neuropathic
pain, especially when the pain is
lancinating or burning.
Non-antiepileptic drugs
Surgical