Etiology Of Obstructive sleep apnea
•Descargar como PPTX, PDF•
3 recomendaciones•1,376 vistas

Brief discussion about etiology of OSA

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (10)
Similar a Etiology Of Obstructive sleep apnea
Similar a Etiology Of Obstructive sleep apnea (20)
Último
Último (20)
Etiology Of Obstructive sleep apnea
- 2. OSA Anatomic disorder bcoz of etiology lies in anatomic area e.g upper airway obstruction,retrognathia,tonsillar hypertrophy,macroglossia etc State dependant condition
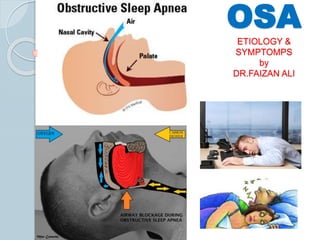
- 3. OSA can be defined as a cessation of breathing during sleep because of a mechanical obstruction such as a retro positioning of the tongue in the airway, a large amount of tissue in the upper airway, or even a partially collapsed trachea. (Semin Orthod 2009;15:63-69.)
- 4. History Obstructive sleep apnea (OSA) was first described by Charles Dickens in 1837. He coined the term “Pickwickian syndrome” but described a similar presentation of a typical OSA patient; obese, somnolent, and with an excessive appetite. It was only in 1956 that Sidney Burwell carefully documented a case of an OSA patient, rationalized the signs and symptoms, and made a distinction between this disease and other illnesses.
- 5. OSA Common respiratory sleep disorder characterized by 1. snoring 2. episodes of breathing cessation or absence of respiratory airflow (10 seconds) during sleep.
- 6. Characterized by recurrent interruptions of breathing during sleep due to temporary obstruction of the airway by lax, excessively bulky, or malformed pharyngeal tissues (soft palate, uvula, and sometimes tonsils), with resultant hypoxemia and chronic lethargy. (Epstein LJ, Kristo D, Strollo PJ, Friedman N, Malhotra A, Patil SP, Ramar K, Rogers R, Schwab RJ, Weaver EM, WeinsteinMD. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. Adult obstructive sleep apnea task force of the American Academy of Sleep Medicine. J Clin Sleep Med. 2009; 5:263-76) OSA
- 7. Upper airway has three major functions: 1. ventilation, 2. swallowing 3. speech. For ventilation, the upper airway must remain patent, but for the other functions, it must narrow or close. In addition, ventilation must be maintained when the nose is occluded or, alternatively, when
- 11. The apnea event is considered when the air flow is interrupted during sleep for a period of 10 s or more. Hypopnea is a reduction of at least 50% of the breathing capacity combined with a saturation decrease of the oxyhemoglobin in at least 3%.
- 13. Narrowing of air way Vibration of tissues of posterior airway SNORING
- 16. This disease affects an average 4% of adult males 2% of adult females increasing as of the fifth decade of life . The prevalence of the disease has been found to be 8% in men 2% of women in the United States (Semin Orthod 2009;15:94-98.)
- 17. About 80 percent to 90 percent of adults with OSA remain undiagnosed. OSA occurs in about two percent of children and is most common at preschool ages OSA with resulting daytime sleepiness occurs in at least four percent of men and two percent of women About 24 percent of men and nine percent of women have the breathing symptoms of OSA with or without daytime sleepiness
- 18. Risk factors according to American academy of sleep medicine People who are overweight (Body Mass Index of 25 to 29.9) and obese (Body Mass Index of 30 and above) Men and women with large neck sizes: 17 inches or more for men, 16 inches or more for women Middle-aged and older men, and post- menopausal women Ethnic minorities People with abnormalities of the bony and soft tissue structure of the head and neck
- 19. Risk factors according to American academy of sleep medicine Adults and children with Down Syndrome Children with large tonsils and adenoids Anyone who has a family member with OSA People with endocrine disorders such as Acromegaly and Hypothyroidism Smokers Those suffering from nocturnal nasal congestion due to abnormal morphology, rhinitis or both.
- 20. Positive risk factor Neck circumference(Indicate upper body obesity) greater than43.2 cm Nasal septal deviation, Internal or external valve collapse Turbinate hypertrophy, Nasal polyps, chronic sinusitis Macro glossia Retro positioning of mandible Enlargement of upper airway soft tissue structures Inferior positioned hyoid bone
- 22. Obesity Increase in size of soft tissue structures in upper airway Dec. functional size of upper airway Predispose toOSA
- 23. Classification of OSA Fujita et al simply categorized the upper airway obstruction as Retro palatal Retro glossal. The retro palatal level involves the soft palate, uvula, and palatine tonsils. The retroglossal level involves the tongue base and supraglottic structures.
- 24. Fujita et Type I obstruction is the presence of restriction only at the retro palatal level. Type II obstruction is the presence of restriction only at the retroglossal level. Type III is the presence of both obstructions at both levels
- 25. Moore classification of OSA Considered the airway obstruction as a spectrum of disease, starting from primary snoring as the mildest form,to upper airway resistance syndrome (UARS) and then to the different degrees of OSA; mild, moderate, and severe.
- 27. Index use for OSA AHI (A common measurement of sleep apnea is the apnea-hypopnea index (AHI). This is an average that represents the combined number of apneas and hypopneas that occur per hour of sleep.) RDI(respiratory distress index) Apnea index, Oxygen desaturation index (ODI)
- 28. Scales use to measure OSA Mallampati Scale Friedman Score The Epworth sleepiness score,
- 29. Sleep nasoendoscopy Identifies the level of and the degree of obstruction when the patient is asleep. Obstructions are classified as palatal, multilevel, or tonguebased with a grading system: Grade 1—palatal snoring; Grade 2—palatal level obstruction; Grade3—multisegmental involvement with intermittent oro- and hypopharyngeal collapse; Grade4—sustained multilevel collapse Grade5—tongue base obstruction.
- 31. Symptoms 1. Loud irregular snoring. 2. Snorts, gasps, and other unusual breathing sounds during sleep. 3. Long pauses in breathing during sleep
- 32. Excessive daytime sleepiness Hall mark of this disease causes impaired cognition increased accident rates multiple medical and dental disorder
- 33. 5. Fatigue 6. Obesity 7. Changes in cognitive functions such as alertness, memory, personality, or behavior 8. Impotence 9. Morning headaches19
- 34. Consequences Cardiovascular. 1. Systemic hypertension 2. Coronary heart disease 3. Cardiac arrhythmias 4. Sudden nocturnal death 5. Other (stroke, pulmonary hypertension) Social/behavioral. 1. Drowsy driving/accidents 2. Decreased work performance 3. Poor quality of life19 4. Increased mortality20-22
- 35. Dentofacial features Narrow upper airway dental arches Hypoplastic maxilla Retrognathic mandible Increased ant.facial height Increased craniocervical angulation than normal
- 36. Post.buccal cross bite Vertical maxillary excess