Hematology_Comprehensive Blood Physiology Review
•
39 recomendaciones•1,895 vistas

Hematology_Comprehensive Blood Physiology Review

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Hematology_Comprehensive Blood Physiology Review
Similar a Hematology_Comprehensive Blood Physiology Review (20)
Más de Imhotep Virtual Medical School
Más de Imhotep Virtual Medical School (20)
Último
Último (20)
Hematology_Comprehensive Blood Physiology Review
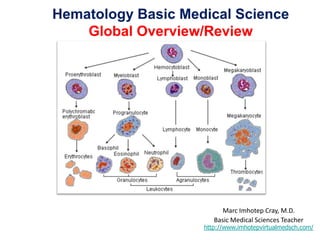
- 1. Hematology Basic Medical Science Global Overview/Review Marc Imhotep Cray, M.D. Basic Medical Sciences Teacher http://www.imhotepvirtualmedsch.com/
- 2. Lecture Outline • Basic properties & functions • Blood plasma • Red blood cells (erythrocytes) • White blood cells (leukocytes) • Platelets • Coagulation • Fibrinolysis • Defense mechanisms 2 Related resources: •WebPath Hematopathology: 70 Images The peripheral blood, bone marrow, lymph nodes, and spleen • HEMATOPOIESIS
- 3. Blood Properties • Sticky • Opaque • Salty-metallic taste • Color varies according to oxygen content • More dense than water and 5x more viscous • pH: 7.35-7.45 (reservoir for bicarbonate ions) • Temperature: 38°C • Volume (4-6 litres; adult). 3
- 4. Blood Basic Functions • Distributes – oxygen and nutrients (removes waste products) – hormones delivered to target organs • Regulates – body temperature, pH • Protects – against blood/fluid loss via hemostasis (coagulation) – against infection via contribution to inflammatory and immune responses. 4
- 5. Blood Plasma • Blood is composed of cellular and non-cellular elements. • If the cellular components are removed: plasma remains. 5
- 6. Blood Plasma • Contains all soluble elements including: – 90% water – 7% protein – 3% salts, sugars, lipids, gases, nutrients, metabolites. • Plasma proteins: – Albumin (60%): osmotic effect. – Globulins (36%): • alpha and beta globulins, transport proteins. • gamma globulins (antibodies/immunoglobulins). – Clotting proteins (4%): eg. fibrinogen and prothrombin Liver 6
- 7. Blood Cellular elements • Red blood cells: – anucleated, discoid structures, designed for O2 transport. • White blood cells: – mononuclear cells: monocytes and lymphocytes. • Vital for functioning of immune system. – polymorphonuclear cells: neutrophils, eosinophils and basophils. • Vital for non-specific defenses (ie inflammation) • Platelets (thrombocytes): – cell fragments derived from megakaryocytes. • Role during clot formation. 7
- 8. Cellular Elements Relative Numbers • Red blood cells: 5 x 106/mm3 8
- 9. Cellular Elements Relative Numbers • Red blood cells: 5 x 106/mm3 • White blood cells: 5 x 103/mm3 9
- 10. Cellular Elements Relative Numbers • Red blood cells: 5 x 106/mm3 • White blood cells: 5 x 103/mm3 • Platelets: 2.5 to 5 x 105/mm3 10
- 11. Red blood cells Erythrocytes • Survive for 100-120 days in circulation. • Remnants broken down by liver and spleen. • Renewed by division and differentiation of stem cells found in the bone marrow: 2 million/second! • Formation controlled in part by the hormone erythropoietin (EPO). – produced by kidney in response to low oxygen levels. • Other regulatory factors: – supplies of iron, amino acids and certain B vitamins – testosterone enhances EPO production. 11
- 12. Red blood cells Regulation of Erythropoiesis 12
- 13. Red blood cells Fate and Destruction • Dead red blood cells are removed by liver & spleen • Heme and globin components are re-used SPLEEN LIVER 13
- 14. Red blood cells Iron Requirements • 0.6 - 2mg required per day. • Absorbed in small intestine. • How is iron used? 14
- 15. Red blood cells Hemoglobin • 0.6 - 2mg required per day. • Absorbed in small intestine. • How is iron used? –To produce hemoglobin 15
- 16. Red blood cells Hemoglobin • Hemoglobin is a molecule specialized for transport of oxygen • Consists of four peptide chains or globins, and four heme molecules HEME 16
- 17. Red blood cells Hemoglobin • Each molecule of heme contains an iron atom • Each heme binds one molecule of oxygen 17
- 18. Red blood cells Iron Storage and Use • Free iron is toxic to body. • Majority is stored as hemoglobin/myoglobin. • Some of the remainder is stored inside cells as a protein-iron complex called ferritin. – Marrow, liver & spleen. • Transported in blood bound to transferrin. • Utilized by electron transport chain (cytochromes) 18
- 19. Red blood cells Iron Cycle • Majority of iron comes from recycling dead RBCs 19
- 20. Red blood cells Vitamin Requirements • Proliferation of RBC precursors requires: – DNA synthesis (ie. precursors have a nucleus). – Protein synthesis (synthesis of some amino acids) • Two B-complex vitamins play critical role: – Folate (50-100 g/day) • required for synthesis of purines and pyrimidines (ie. A, T, C, G and U bases found in nucleic acids). – Vitamin B12 (approximately 3g/day ) • required for synthesis of some amino acids. 20
- 21. Blood Typing • Based on type of glycoproteins present on the surface of red blood cells. • If foreign glycoproteins are presented to the immune system (ie transfusion of incompatible blood), then the RBC are clumped together and destroyed. • ABO blood groups are based on the expression of type A and type B glycoproteins (agglutinogens). • Rhesus groups: based primarily on agglutinogen D. 21
- 22. Blood Typing • AB: produce both glycoproteins – rare, can receive donations from A, B, AB or O. • A: produce type A glycoprotein. – Can receive donations from A or O. • B: produce type B glycoprotein. – Can receive donations from B or O. • O: produce neither A nor B. – Most common, can receive only O type. 22
- 23. Blood Typing • Rhesus (+) Most Common – produce agglutinogen D. • Rhesus (-) – don’t produce agglutinogen D. Antibodies to agglutinogen D are produced more slowly than those to types A and B. Rhesus (-) mothers have to be treated if carrying a rhesus (+) baby. 23
- 24. Blood Hematocrit • The % volume occupied by red blood cells is known as the hematocrit. • Volume occupied by white blood cells is relatively small. 24
- 25. White Blood Cells (Leukocytes) Granular leukocytes – Neutrophils (40-70%) – Eosinophils (acidophils, <5%) – Basophils (<1%) Agranular leukocytes – Lymphocytes (20-45%) – Monocytes (<10%) 25
- 27. GRANULOCYTES 1. Neutrophils • 40 - 75% of leukocytes • 10 - 14um diameter • Exhibit multi - lobed nuclei • Cytoplasm lightly stippled with indistinct granules - represents large lysosomes • Active phagocytes that ingest bacteria & cell fragments 27
- 29. • 1 - 6% of leukocytes • 10 - 14um diameter • Bilobed nucleus • Abundant large ovoid granules - stain bright red with eosin • Phagocytes that ingest antibody + antigen complexes • Release histaminase that inhibits inflammation GRANULOCYTES 2. Eosinophils 29
- 31. • < 1% of leukocytes • 10 - 16um diameter • U- or S-shaped bi-lobed nucleus • large blue cytoplasmic granules - exhibit basophilic staining • Granules contain materials that mediate inflammation - eg. histamine GRANULOCYTES 3. Basophils 31
- 33. • 20 - 30% of leukocytes • 6 - 9um diameter (small) • 9 - 15um diameter (large - 3%) • Round, densely stained nuclei • Pale non-granular cytoplasm • Small lymphocytes have relatively little cytoplasm - attack pathogens & regulate immune responses • Large lymphocytes make antibodies AGRANULOCYTES 1. Lymphocytes 33
- 35. • 2 - 10% of leukocytes • 14 - 24um diameter • Large, often indented, nuclei • Abundant grey-blue cytoplasm with fine granules • Cytoplasmic vacuoles often evident • Highly motile • Differentiate into macrophages which phagocytose pathogens & dead tissue AGRANULOCYTES 2. Monocytes 35
- 37. Eating-like behavior of cells. Performed by: –Neutrophils –Monocytes Targets: –Bacteria or other foreign materials. –Damaged/infected/abnormal cells. Phagocytosis 37
- 39. • Small cell fragments • Possess granules • 2.5 to 5 x 105/mm3 • Produced by megakaryocytes in marrow. • Regulated by thrombopoietin. • Contain granules. • Role in clotting Platelets 39
- 40. Platelets Role during clotting • React with extracellular matrix proteins when blood vessels are severed. • Stick to collagen and form plug. • Release variety of chemical mediators from granules. • Stimulate coagulation and wound healing. 40
- 41. Blood Clotting Consists of three basic phases: • Constriction of vessels • Reduces blood flow. • Platelet aggregation • Plugs hole in vessel wall. • Coagulation. • Reinforces platelet plug by forming fibrin mesh. 41
- 42. Coagulation • Cascade of chemical reactions that result in formation of a fibrin mesh. • Involves 12 different clotting factors – factor IV is calcium, (factor VI now recognised as V) •Critical events – Formation of prothrombin activator (Ca2+/TF or PF3). – Conversion of prothrombin (factor II) into thrombin. – Conversion of fibrinogen (factor I) into fibrin. 42
- 43. There are three pathways to consider:- COAGULATION PATHWAYS 1. Extrinsic pathway 2. Intrinsic pathway 3. Common pathway 43
- 44. 44
- 45. EXTRINSIC PATHWAY 1.There is a rapid initiation of coagulation when "Tissue Factor” (a protein-phospholipid complex normally present on vascular cells and activated monocytes), is exposed to factor VII in the presence of calcium. 2.The activated Tissue factor-VII complex activates factors IX and X (Factor IXa enhances the production of Xa, especially in the presence of the co-enzyme VIIIa). Blood clotting through the extrinsic system is quick (10 - 13 secs). 45
- 46. When tissue or endothelial cells are damaged they release tissue factor, which combines with two clotting factors to make the enzyme tissue thromboplastin EXTRINSIC PATHWAY 46
- 47. The pivotal molecule in both pathways is thromboplastin. The intrinsic pathway is triggered when thromboplastin is released from the platelets and the intermediates of the pathway are activated on the platelet surfaces. Each pathway requires Ca2+ and involves the activation of a series of procoagulants each serving to activate the next coagulant in line. The intermediate steps of each pathway fall to a common intermediary factor X. INTRINSIC PATHWAY 47
- 48. INTRINSIC PATHWAY 48 The aggregated platelet plug releases platelet factor 3, which combines with two clotting factors to make the enzyme platelet thromboplastin
- 49. The common pathway begins once either of the two types of thromboplastin are formed. When this happens, prothrombin is converted into the enzyme thrombin. Thrombin then takes the final step in the coagulation process by converting fibrinogen into fibrin. COMMON PATHWAY 49
- 50. • Platelets have inside them contractile proteins called thrombasthenins • When the platelets contract they reduce the size of the entire blood clot pulling the torn edges of the vessel closer together, reducing the size of the damaged area, and making repairs easier. CLOT RETRACTION 50
- 51. The continuous generation of cross-linked fibrin would create a clot capable of obstructing normal blood flow The Fibrinolytic system is present to keep clot formation in check by actually degrading the fibrin FIBRINOLYSIS 51
- 52. Once hemostasis is restored and the tissue is repaired, the clot must be removed from the injured tissue. This is achieved by the fibrinolytic pathway. The end product of this pathway is the enzyme plasmin, a potent proteolytic enzyme with a broad spectrum of activity. FIBRINOLYSIS Plasmin is formed by activation of the proenzyme, plasminogen by either plasma or tissue activators. Tissue plasminogen activators are found in most tissues, except the liver and the placenta, where they are synthesized by endothelial cells and are found concentrated in the walls of blood vessels. The two best characterised are vascular activator (commonly known as tissue plasminogen activator -- tPA) and urokinase. 52
- 53. Fibrinolysis works in a steady state with haemostasis. Damaged endothelium releases tissue plasminogen activator as well as plasminogen - both of which are adsorbed to the fibrin surface FIBRINOLYSIS 53
- 55. • Inflammation: non-specific. • Immune system: specific Defense Mechanisms 55
- 56. The body’s response to injury Inflammation 56
- 57. Anatomical: Redness, swelling, heat, pain, poor function. Histological: Leukocytes accumulate in inflamed tissues. Inflammation Signs and Symptoms 57
- 58. Acute: Short duration (hours, days) Possible neutrophil influx Chronic: Long duration (weeks, months) Immune system recruited (lymphocytes) Inflammation Degrees of severity 58
- 59. Blood vessels: changes in diameter and permeability. Leukocytes: chemotactic emigration. Both regulated by the production and release of inflammatory mediators. Inflammation Underlying Mechanisms 59
- 60. Crawling-like motility of cells. Powered by actin cytoskeleton. Displayed by variety of cell types. Utilised by leukocytes to emigrate and seek-out bacteria. Inflammation Amoeboid Migration/Diapedesis 60
- 61. Directed migration of cells in response to a concentration gradient of soluble stimulus: –eg. Products secreted by bacteria. –eg. Inflammatory mediators. Inflammation Chemotaxis 61
- 62. • Derived from plasma proteins: – e.g. products released during clotting. • Derived from cells: – e.g. histamine, cytokines. Only released/act locally. (hormonal-like specificity) Inflammation Inflammatory Mediators 62
- 64. Tissue damage Chemical mediators releasedIncreased vascular permeability Chemotaxis Fibrin mesh isolates injury site Increased numbers of white blood cells at injury site Pathogens contained & destroyed Pathogen Inflammatory Response 64
- 65. Additional Nonspecific Resistance Chemical defenses 1. Complement • group of about 20 serum proteins • when combined with foreign substances a “complement cascade” is activated • complement proteins rupture bacterial membranes 2. Interferon • stimulate body cells to resist viral infection • inhibits viral replication 65
- 67. The Immune System • Specific: via receptor ligand interactions. • Acquired: via “education” of lymphocytes. • Systemic: via emigration of lymphocytes. • Memory: via survival of lymphocytes. 67
- 68. The Immune System Specificity is driven by receptor-ligand type interactions. Two main pathways: 1. Humoral pathway (involves B lymphocytes). 2. Cell mediated pathway (uses T lymphocytes) 68
- 69. Humoral Pathway ANTIBODIES: proteins secreted by activated B lymphocytes, that bind to antigens (immunoglobulins). ANTIGENS: any chemical which elicits an immune response (usually foreign). 69
- 70. Basic Antibody Structure Antigen binding site Heavy chain Light chain Constant region Variable region 70
- 71. B-lymphocytes Produce antibodies against foreign proteins Antibodies (immunoglobulins - Ig) • proteins produced by plasma cells (mature form of B-lymphocytes) • bind to SPECIFIC foreign proteins 5 main classes 1. IgG - most abundant 2. IgM - first circulating Ig released 3. IgE - involved in inflammatory responses 4. IgA - body secretions 5. IgD - surface receptor 71
- 72. Humoral Pathway Antibodies and antigens bind each other to form IMMUNE COMPLEXES. ANTIGENIC DETERMINANT: The region of an antigen that is recognised. 72
- 75. Humoral Response Consequences of immune complex formation. 1. Neutralisation of toxic antigens. 2. Activation of leukocytes. 3. Formation of inflammatory mediators. 4. Destruction of bacteria. 75
- 76. • Antigen-receptor interactions occur on the cell surface. • Two types of interaction: – Antigen presenting cells (APC) and Helper T cells. – Cytotoxic T cells and abnormal cells. Cell Mediated Response 76
- 77. APC MHCII-antigen complex Antigen MHCII T-cell receptor Helper T cell Cytokines Released MHC = Major-Histocompatibility-Complex molecule. Cell Mediated Response 77
- 78. Infected Cell MHCI-antigen complex Virus MHCI T-cell receptor Cytotoxic T cell Infected cell Killed Cell Mediated Response 78
- 79. Virus infected cell Killer T cell Cell lysis initiated Time Cytotoxic T-cell Response 79
- 80. “Education” by Clonal Selection Memory cells ATTACK 80