Poster UPASICON 2016, Allahabad - Won Third Prize
•
2 recomendaciones•436 vistas

Post-bullhorn Injury Abdominal Wall Hernia: Role of Laparoscopic Tissue Repair
Recomendados

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Poster UPASICON 2016, Allahabad - Won Third Prize
Similar a Poster UPASICON 2016, Allahabad - Won Third Prize (19)
Más de Dr Kaushal Deep Singh Mathuria
Más de Dr Kaushal Deep Singh Mathuria (18)
Último
Último (20)
Poster UPASICON 2016, Allahabad - Won Third Prize
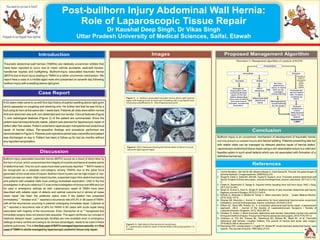
- 1. Traumatic abdominal wall hernias (TAWHs) are relatively uncommon entities that have been reported to occur due to motor vehicle accidents, seat-belt injuries, handle-bar injuries and bullfighting. Bullhorn-injury associated traumatic hernia (BATH) due to blunt injury leading to TAWH is a rather uncommon mechanism. We report here a case of a middle-aged male who presented on seventh day following bullhorn injury with a swelling above right groin. . Introduction A43 years male came to us with five-day history of painful swelling above right groin which appeared on coughing and straining only. He further told that he was hit by a bull using its horn at the same site 1-week back. Patients all vitals were within normal limit and abdomen was soft, non-distended and non-tender. Clinical features (Figure 1) and radiological features (Figure 2) of the patient are summarized. Since the patient was hemodynamically stable, patient was planned for laparoscopic repair of defect after few weeks. Patient underwent laparoscopic transperitoneal anatomical repair of hernial defect. Per-operative findings and procedure performed are demonstrated in Figure 3. Patients post-operative period was uneventful and patient was discharged on day-3. Patient has been in follow-up for last six months without any reported complication. Case Report Bullhorn-injury associated traumatic hernia (BATH) occurs as a result of direct blow by the horn of a bull, which compromises the integrity of muscles and fascia at weaker points (1-6) of abdominal wall. Only six such cases have been previously reported. BATH needs to be recognized as a separate sub-category among TAWHs due to the great force generated at the small area of impact. Bullhorn blunt injuries can be high-impact or low- impact (as was our case). High-impact injuries, suspected major intra-abdominal injuries and patients with unstable vitals must undergo immediate exploration. USG is the first investigation in all such cases but CT scan is the investigation of choice over MRI as it can be used in emergency settings as well. Laparoscopic repair of TAWH have been described with reliable repair of defects and optimal outcome but in almost all cases mesh repair has been the preferred option even if the patient has presented (7) (8) immediately. Honaker et al. reported a recurrence rate of 8.3% in 38 cases of TAWH, with all the recurrences occurring in patients undergoing immediate repair. Coleman et (9) al. reported a recurrence rate of 26% for TAWH in 80 cases with acute repair being (10) associated with majority of the recurrences. Even, Damschen et al. recognized that immediate surgery does not prevent late sequelae. This again reinforces our concept of relatively delayed repair. Laparoscopic facilities are now available even in emergency settings at many centres and owing to its obvious advantages, needs to be used in these patients judiciously. This is the first case of BATH managed laparoscopically and first case of TAWH in adults managed by laparoscopic anatomic tissue only repair. Discussion Images Figure 1: A - Bullhorn-associated traumatic hernia above right inguinal region with healing bruise at lower part of swelling with a suprapubic scar of previous cystolithotomy; B – Site of laparoscopic ports Figure 2: CECTAbdomen showing the hernial defect of about 2 cm just above the right inguinal region Figure 3: A- Split defect in the fascial and muscle layer; B - Laparoscopic anatomic repair of hernial defect with polypropylene 1-0 sutures Flowchart 1: Management algorithm of a patient of BATH Presentation Immediate Delayed Evaluate the hernial defect size, location, contents by CECT Unstable Stable Emergency Exploration with anatomical/mesh repair of hernial defect depending upon size of defect and local tissue strength, hematoma, laceration CECT Abdomen No intra- abdominal injury or injury that can be managed conservatively Major/operable abdominal injury Managepatient conservatively for 3-4 weeks Delayed anatomical (=2cm defect)/mesh repair (>2 cm defect); laparoscopic > open Usually no major or associated injury and/or stable patient Proposed Management Algorithm Bullhorn injury is an uncommon mechanism of development of traumatic hernia and may present as isolated muscle and fascial splitting. Patients presenting late but with stable vitals can be managed by delayed elective repair of hernial defect. Laparoscopic anatomical tissue repair using a non-absorbable suture is a valid and feasible option in such small defects which are not associated with formation of a definitive hernial sac. Conclusion 1. Comin Novella L, del Val Gil JM, Moreno Muzas C, Oset Garcia M. The bull: the great danger of summer festivals. Cirugia espanola. 2008;83(4):215. 2. Singal R, Dalal U, Dalal AK, Attri AK, Gupta R, Gupta A, et al. Traumatic anterior abdominal wall hernia: A report of three rare cases. Journal of emergencies, trauma, and shock. 2011;4(1):142- 5. 3. Chate N, Deshmukh S, Dange A. Inguinal hernia resulting from bull horn injury. ANZ J Surg. 2011;81(12):943. 4. Singh B, Kumar A, Kaur A, Singla R. Bullhorn hernia: A rare traumatic abdominal wall hernia. Nigerian Journal of Surgery. 2015;21(1):63-5. 5. Nirhale D, Athavale V, Bhatia M, Tomar V. Silent traumatic hernia. Sudan Medical Monitor. 2015;10(4):137-9. 6. Dharap SB, Noronha J, Kumar V. Laparotomy for blunt abdominal trauma-some uncommon indications. Journal of emergencies, trauma, and shock. 2016;9(1):32-6. 7. Wilson KL, Davis MK, Rosser JC, Jr. A traumatic abdominal wall hernia repair: a laparoscopic approach. JSLS : Journal of the Society of Laparoendoscopic Surgeons / Society of Laparoendoscopic Surgeons. 2012;16(2):287-91. 8. Honaker D, Green J. Blunt traumatic abdominal wall hernias: Associated injuries and optimal timing and method of repair.The journal of trauma and acute care surgery. 2014;77(5):701-4. 9. Coleman JJ, Fitz EK, Zarzaur BL, Steenburg SD, Brewer BL, Reed RL, et al. Traumatic abdominal wall hernias: Location matters. The journal of trauma and acute care surgery. 2016;80(3):390-6; discussion 6-7. 10.Damschen DD, Landercasper J, Cogbill TH, Stolee RT. Acute traumatic abdominal hernia: case reports.The Journal of trauma. 1994;36(2):273-6. References Thank You Post-bullhorn Injury Abdominal Wall Hernia: Role of Laparoscopic Tissue Repair Dr Kaushal Deep Singh, Dr Vikas Singh Uttar Pradesh University of Medical Sciences, Saifai, Etawah