Cv junction
•Descargar como PPTX, PDF•
22 recomendaciones•3,598 vistas

radiology presentation of cv junction

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Similar a Cv junction
Similar a Cv junction (20)
Más de Dr Praveen kumar tripathi
Más de Dr Praveen kumar tripathi (17)
Último
Último (20)
Cv junction
- 1. DR PRAVEEN K TRIPATHI
- 2. The term ‘cv junction’ refers to the occipital bone that surrounds the foramen magnum and the atlas and the axis vertebrae. The C-V junction is a transition site between mobile cranium and relatively rigid spinal column. It is also the site of the medullo spinal junction. Accounts for approximately 25% of the vertical height of the entire cervical spine
- 3. Meckel , 1815 : manifestation of occipital Vertebrae Bell , 1830 : first described spontaneous Atlantoaxial dislocation 1886 – giacomini described the first case of congenital aad 1912Maurice Klippel and Andre Feil Chamberlain , 1937 : basilar invagination Carl List, in 1941, described the neurological syndromes accompanying developmental anomalies of the occipital bone, the atlas, and the axis vertebrae 1960 – wadia-congenital aads Greenberg , 1968 : classified atlantoaxial Anomalies Atul Goel 2014 . Goel's Classification of Atlantoaxial ‘facetal’ dislocation.
- 4. ● Notochord forms early axial skeleton ● During 4th week gestation, 42 somites formed o 4 occipital, 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, 8-10 coccygeal ● Each somite differentiates o outer dermatome o inner myotome o medial sclerotome - form vertebrae around notocord 4 occipital sclerotomes ● 4th Occipital Sclerotome - Proatlas - important for CVJ development
- 5. Develops from the 4 occipital and upper 2 cervical somites. The mesoderm caudal to neural plate condenses into four occipital somites, these are the precursors of occipital sclerotomes. First Two - Basiocciput Third - Jugular tubercles * Fourth occipital sclerotome Proatlas
- 8. Proatlas Hypocentrum Centrum Neural arch Anterior tubercle Apex of dens Ventral Dorsal of clivus & Apical ligament Rostral Caudal
- 9. First spinal sclerotome Atlas vertebra is primarily formed from this sclerotome. Sclerotome division Hypocentrum Centrum Neural Arch Anterior arch C1 Dens Inferior portion of (mid portion the posterior arch of the odontoid process and fused with axis)
- 10. Second spinal sclerotome Develops into axis vertebra Sclerotome division Hypocentrum Centrum Neural Arch Disappears Body of axis Facets & Posterior arch of axis
- 12. Constituents of CV junction Osseous components and their articulations Ligamento-muscular elements Neuro-vascular structures Characteristics of CV junction Mobility at the cost of stability Constantly changing structure and kinematics –even in the post natal period Vital neuro-vascular relations
- 13. Atlas * Named after the mythical giant who carried the earth on his shoulder. * Thin Anterior and posterior arches •Sturdy Lateral masses – made up of a column of superior and inferior articular facets placed in a vertical line •No body
- 14. Axis: Forms the axis of rotation Dens is the divorced body of C1 Bifid spinous process Inferior facet more posterior than superior facet
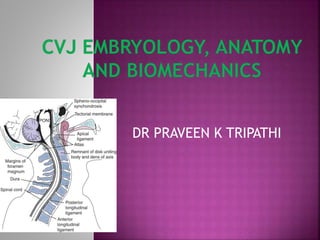
- 18. POSTERIOR - POSTERIOR ATLANTOOCCIPITAL MEMBRANE: EXTENDS FROM OCCIPITAL BONE TO POSTERIOR ARCH OF ATLAS. IT IS SHARP & THIN & IN DIRECT CONTACT WITH ANTERIOR CORTEX OF POSTERIOR ARCH OF ATLAS
- 19. Anterior Longitudinal Ligament : Extending from lower border of anterior arch of C1 to body of Axis Anterior Atlanto-occipital Membrane : Extends from anterior edge of Foramen Magnum to anterior arch of C1
- 20. TECTORIAL MEMBRANE Cephalic extension of PLL inserted into processus basilaris 1-2cm above basion
- 21. OCCIPITOTRANSVERSE LIGAMENT: TO BASION INFERIOR LOGITUDINAL BAND: TO AXIS BODY TRUE TRANSVERSE LIGAMENT
- 22. STRONG HORIZONTAL PORTION MAINTAINS THE POSITION OF DENS IN SAGITTAL & CRANIOCAUDAL DIRECTION ARTICULATES WITH ODONTOID FACET INSERTED LATERALLY IN BONY PROMINENCE IN INNER ASPECT OF CONDYLES IT IS 8mm IN HEIGHT AND 2-3 MM THICK IN MIDLINE
- 23. BARKOWS LIGAMENT- FROM TIP OF DENS TO ANTEROLATERAL FM RIM APICAL LIGAMENT- TIP OF DENS TO MIDDLE PART OF FM RIM GRUBERS LIGAMENT- TRANSVERSE LIG TO TIP OF DENS
- 24. ALAR LIGAMENT- VERY STRONG LIGAMENT 6 – 8 mm DENS TIP TO LATERAL PART OF RIM OF FM
- 25. VERTEBRAL ARTERIES - Anterior and Posterior ascending arteries. CAROTID ARTERY : Anterior ascending artery. Forms an apical arterial arcade in the region of alar ligament and sends perforators VENOUS DRAINAGE : Periodontal venous plexus and suboccipital venous sinuses drain to pharyngovertebral veins
- 26. LYMPHATIC DRAINAGE : CV JUNCTION DRAINS TO RETROPHARYNGEAL LYMPH NODES & THEN TO THE UPPER DEEP CERVICAL CHAIN RETROGRADE INFECTION OF CV JUNCTION FROM PHARYNX , SINUSES & RETROPHARYNGEAL AREAS : GRISEL’S SYNDROME
- 27. MOVEMENTS : FLEXION EXTENSION SLIDING MOVEMENT LATERAL FLEXION ROTATION
- 28. FLEXION & EXTENSION : JOINTS INVOLVED : OCCIPITOATLANTAL & ATLANTOAXIAL AVERAGE RANGE AT OCCIPITOATLANTAL JT. : 13 – 15 DEGREES ATLANTOAXIAL JT. : 10 DEGREES FLEXION IS LIMITED BY : TECTORIAL MEMBRANE DENS BASION CONTACT EXTENSION LIMITED BY : STRETCHING OF TEC. M OPISTHION POST. ARCH OF ATLAS CONTACT
- 29. ANTERO-POSTERIOR TRANSLOCATION BETWEEN DENS & ANT. RING OF ATLAS : ADULTS : 3mm YOUNG CHILDREN : 5mm ADULTS UPTO 5 mm : RUPTURE OF CRUCIATE LIG. > 5 mm : RUPTURE OF BOTH CRUCIATE & ALAR LIG.
- 30. JOINT INVOLVED : ATLANTOAXIAL JOINT MAXIMUM RANGE : 37 – 42 DEGREES > ROTATION LEADS FACET JT. INTERLOCKING ROTATION > 32 – 35 DEG. : ANGULATION OF CONTR. VERT. ARTERY > 45 DEG. : IPSILATERAL VA OCCLUSION
- 31. LATERAL ROTATION : 90 DEG. JT. INVOLVED : ATLANTOAXIAL & LOWER C-SPINE LATERAL FLEXION : SMALL AMPLITUDE 5 – 10 DEG.
- 32. SLIDING MOVEMENT : FORWARD OR BACKWARD MOVEMENT OF HEAD WITHOUT FLEXION OR EXTENSION OF NECK FORWARD SLIDE : AXIS INCLINES FORWARD POST. DISPLACEMENT OF AXIS ANT. ARCH OF ATLAS SLIDES UP ATLANTOODONTOID SPACE GAP OCCIPITOODONTOID SPACE GAP N : 3 – 6 mm DOUBLE IN FORWARD SLIDE BACKWARD SLIDE :ANT. ARCH OF ATLAS SLIDES DOWN POST. ATLANTOOCCIPITAL SPACE
- 34. Menezes classified CV junction anomalies into two broad categories Congenital (Primary) Developmental and Acquired (Secondary) CV junction anomalies and AAD classifications overlap
- 37. Abnormalities of Foramen magnum DEFORMITIES OF FORAMEN MAGNUM N : AP DIAMETER – 30-40 mm STENOSIS : < 30 mm ENLARGEMENT : > 40 mm -MENINGIOMA - EPIDERMOID - CYSTIC MALFORMATION -ACM
- 38. AAD is not a disease per se , rather it’s a manifestation of a spectrum of pathological states. This is a condition in which the atlas(C1) slips over the axis(C2) in the antero-posterior direction resulting in neural structure compression between the two vertebrae. A distance of >3mm in an adult & >4.5mm in a child between posterior surface of anterior Arch of C1 & anterior surface of dens is thought to be due to incompetence of Transverse Ligament with associated instability.
- 39. Greenberg’s Classification of AAD I Incompetence of odontoid process II Incompetence of Transverse Atlantal ligament I Incompetence of odontoid process A. Congenital 1. Type I Separate odontoid: OS odontoideum 2. Type II Free apical segment: Ossiculum Terminale 3. Type III Agenesis of odontoid base 4. Type IV Agenesis of Apical segment 5. Type V Agenesis of odontoid process totally
- 41. B. Traumatic 1. Acute 2. Chronic C. Infectious e.g Tuberculosis D. Tumors 1. Primary 2. Metastatic
- 42. II Incompetence of Transverse Atlantal ligament A. Congenital: 1. Idiopathic 2. Mongolism B. Traumatic 1. Acute - Rupture of TAL 2. Chronic - Assimilation of atlas - Block vertebrae C2 & C3 C. Hyperaemic 1.Infection–Bacterial/viral(Grisel’s syndrome)/granulomatous 2.Rheumatoid arthritis
- 43. Wadia proposed the following classification Group I: AAD with * Occipitalization of atlas * Fusion of C2, C3 vertebrae * Odontoid process dislocated posteriorly Group II: AAD with * No occipitalization of atlas * No Fusion of vertebrae * Odontoid process dislocated because of its maldevelopment Group III: AAD with * No occipitalization * No fusion of vertebrae * Odontoid is normal in shape and size to body of the axis. I & II are usually developmental and III is acquired
- 44. Biomechanical Translatory Rotary Radiological Mobile Fixed Clinical Reducible Irreducible
- 46. The term Basilar Invagination was used by Chamberlain in 1939 . This is a primary defect implying prolapse of the vertebral column into the skull at the base.
- 47. Two types of Basilar invagination A. Ventral: There is shortening of the basiocciput so that clivus is short & horizontally oriented thus displacing the plane of the FM in an upward direction compared with spinal column. B.Paramesial : Condylar hypoplasia may be present so that clivus become dorsally displaced into posterior fossa but may be of normal length.
- 48. BI is commonly associated with an abnormal odontoid process invaginating into posterior fossa. Axis becomes elongated and the true odontoid process is small. There is abnormal clivus-odontoid articulation. The resultant abnormal clivus-canal angle produces an indentation on the pons, medulla or cervicomedullary junctionin a ventral manner. Chiari Malformation is associated with BI in 25 – 30%cases.
- 49. PSEUDOBASILAR INVAGINATION OCCIPITALIZATION OF POSTERIOR ARCH OF C1 HYPERTROPHY OF ODONTOID PROCESS ASSOCIATED FEATURES : ACM BILATERAL AGENESIS OF VA
- 50. OS Odontoideum Definition – An independent bone cranial to the axis, in the place of dens. It is not an isolated dens but exists apart from a small hypoplastic dens. Two types : (Fielding & Griffin) A. Orthotopic variety: OS lies in the position of dens and moves with atlas and axis. B. Dystopic variety: OS lies near the inferior end of clivus & fuses with the occipital bone and moves in unison with clivus. Congenital Os Odontoideum Traumatic Os Odontoideum 1. H/o Trauma - often present Always present 2. Location - Usually between base of dens and usually between the base body of the axis (below superior and apical segment of the dens facet of axis ) (above superior facet of axis) 3. Line of separation - Always smooth Acutely irregular and not corticated and corticated 4. Associated congenital anomaly - Absent often present
- 51. Failure of fusion of the terminal ossicle to remainder of the odontoid process Fusion by 12 years of age Confused with a type 1 odontoid fracture (avulsion of the terminal ossicle) Differentiation between traumatic or congenital -difficult stable when isolated odontoid process is usually normal in height.
- 52. The most interesting feature of the clinical presentation is the diversity.This is due to compression of the lower brainstem, cervical spinal cord, cranial nerves, cervical nerve roots, & vascular supply. Presentation may be insidious, or as false localizing sign, infrequently a rapid neurological progression followed by death.
- 53. The most common symptom is neck pain originating in suboccipital region with radiation to cranial vertex region -85%. False localising signs: Usually motor monoparesis, paraparesis, & quadripresis.
- 54. GENERAL EXAM : Abnormal general physical apperance. KLIPPEL- FEIL SYNDROME :Triad of Low hairline, short neck and a webbed neck with limitation of neck movements. OTHER DYSPLASTIC FEATURES: high arch palate poly/syndactyly pes cavus scoliosis sprengel shoulder,
- 55. Motor deficits- legs more involved Cruciate paralysis Posterior tract symptoms- Lhermitte sign Central cord syndrome Neck pain/ cough headache Lower cranial nerve paresis Hearing loss(most common)-25% Hypoglossal paralysis (Klaus 1969)
- 56. Sleep apnea and dysphagia Nystagmus Gait ataxia Syncope Vertigo Episodic paresis Transient visual loss. Due to vertebro basilar insufficiency Present in 15 – 25% of cases.
- 57. Importants Points to remember 1. Short neck, low hairline, restricted neck movements are frequently seen in KF anomaly, Occipitalization, and basilar invagination 2. Transient Attacks of VB insufficiency are usually encountered in Pts. With A-A dislocation. 3. Several bony and soft tissue anomalies often co-exist 4. Neurological deficit is usually produced by A-A dislocation, Basilar Invagination, ACM and Syringomyelia / Syringobulbia
- 58. Conventional antero-posterior and lateral views will reveal the presence and type of cranio-vertebral anomaly. It will show whether the odontoid is present or absent and also the integrity of the rings of atlas and axis. Block vertebrae and occipitalisation of atlas are also visualised. The open mouth view shows hypoplastic odontoid, os odontoideum or ossiculum terminale with clarity.
- 59. determine basilar invagination, which is an upward movement of the base of the skull in the region of the foramen magnum. It is measured by the intracranial extension of the tip of the odontoid process.
- 60. Chamberlain's line (1939) is drawn from the posterior lip of the foramen magnum to the dorsal margin of the hard palate. Intracranial projection of up to one third of the length of the odontoid is normal. McGregor's line (1948) is drawn from the upper surface of the posterior edge of the hard palate to the most caudal point of the occipital curve of the skull. The tip of the odontoid normally does not extend more than 4.5 mm above this line. McRae's line (1953) defines the opening of the foramen magnum.
- 62. These are the lateral views of the cervical spine in flexion and extension. These are absolutely essential to determine the presence of atlanto-axial instability and cord compression. The atlanto-dens interval (ADI) is the space between the anterior aspect of the dens and the posterior aspect of the anterior arch of atlas. This is measured by the distance from the posterior aspect of the odontoid or axis to the nearest posterior structure. (Posterior ring of atlas or foramen magnum). in patients with atlantooccipital fusion, those with less than 19mm of available space behind the odontoid or atlas were symptomatic.
- 63. CHAMBERLAIN’S LINE MCRAE’S LINE Posterior margin of hard palate to opisthion( ) Normal- tip of dens less than 5mm below this line Abnormal- in basilar invagination Line from basion to opisthion ( ) Normal – tip of dens below this line Abnormal-in basilar invagination
- 64. MCGREGOR’S LINE WACKENHEIM’S LINE Posterior margin of hard palate to lowest part of occipital bone Normal- tip of dens less than 7mm below this line Abnormal- in basilar invagination Line extrapolated along dorsal surface of clivus Normal – dens should be tangential or anterior to this line Abnormal-in basilar invagination
- 65. DIGASTRIC LINE BIMASTOID LINE Line between incisurae mastoidae ( ) Normal- 10mm above atlanto- occipital joint Line between tips of mastoid processes ( ) Normal – intersects atlanto- occipital joint
- 66. WELCHER BASAL ANGLE CLIVUS CANAL ANGLE Angle at junction of nasion- tuberculum and tuberculum- basion lines Normal- 132-140 degree Abnormal->143 degree in platybasia Angle at junction of Wackenheim’s line and posterior vertebral body line Normal – 150-180degree Abnormal-<150 degree in platybasia
- 67. ATLANTOOCCIPITAL JOINT AXIS ANGLE KLAUS INDEX Angle formed at junction of lines along atlanto-occipital joints ( ) Normal -124-127 degree Obtuse in condyle hypoplasia Distance between dens and tuberculum cruciate line ( ) Normal-40-41mm Basilar invagination-<30mm
- 68. Skull base flattening Primary and secondary Bow string deformity Increased basal angle Decreased clivus canal angle ( ) Association – basilar invagination 32 year old gentleman with decreased clivus canal angle( ) , violation of Chamberlain’s line( , ) acute angulation, compression of cervicomedullary juncion ( ) PLATYBASIA
- 69. Abnormally high vertebral column Prolapse into skull base Secondary- basilar impression Chamberlain’s line Mc Gregor’s line Digastric line 24 year old gentleman with violation of Chamberlain’s line( ) and digastric line( ), atlantoaxial dislocation(atlantodens interval-3.8mm) BASILAR INVAGINATION
- 70. Anterior and posterior arch anomalies Total or partial aplasia Isolated anterior arch anomalies –rare Split atlas CT axial section showing posterior atlas arch rachischisis CT axial section showing partial anterior arch rachischisis( ) and os odontoideum( ) Hypertrophic anterior arch( ); corticated margins Jefferson’s fracture Irregular margins ; normal anterior arch CONGENITALANOMALIES-ATLAS
- 71. OS ODONTOIDEUM OSSICULUM TERMINALE Separate odontoid process Failure of fusion of base with body of axis Bergmann ossicle Failure of fusion of apical segment with base of dens CONGENITALANOMALIES-AXIS T1W MRI sagittal section showing os odnotoideum( CT sagittal section showing os odnotoideum( ) with ossiculum terminale( )
- 72. KLIPPEL FIEL SYNDROME CHIARI MALFORMATION Complex entity causing cervicovertebral fusion Associations- occipito-atlantoid fusion Low lying tonsils Associations- basiocciput hypoplasia, atlanto-occipital assimilation, platybasia CONGENITAL SYNDROMES 16 year old lady with herniated tonsils( ) Acute clivocanal angle( ),short clivus( ) and cervical cord compression CT sagittal section showing violation of Chamberlain’s line ( ), atlantooccipital fusion( ), atlantodens interval of 3.9mm( ),fused C5-C8( )
- 73. Congenital Acquired Traumatic Atlantodens interval 3mm - adults 5mm - children ATLANTOAXIAL DISLOCATION 20 year old man with type 2 dens fracture(irregular margins( ) and atlantoaxial dislocation( ) 47 year old lady with rheumatoid arthritis with basilar impression, sclerosis of atlantoaxial joint( ) and atlantoaxial dislocation( ) 18 year old lady with TB, retropharyngeal collection( ), lytic area in dens( ) and atlantoaxial dislocation( ) 38 year old lady with increased atlantodens interval( ) SPONTANEOUS INFECTIVERHEUMATOID ARTHRITISTRAUMA
- 74. Lines and angles used in radiologic diagnosis of C.V anomalies. Parameter Normal range limits A. PLATYBASIA B. BASILAR INVAGINATION C. ATLANTO-AXIAL DISLOCATION * • Basal angle < 150 degree • Boogard’s angle (Angle between the clivus line and McRae's line)< 136 degree • Bull’s angle (Line drawn between the posterior and anterior arch of C1. Bull's angle is the angle between this line and the hard palate plane. < 13 degree • Chamberlain’s line < one third of odontoid above this line • Mcgregor’s line < 5 mm • Mcrae line odontoid lies below this • Klaus height index > 35 mm • Atlanto-temporo > 22mm. mandibular index • Atlanto-odontoid space upto 3 mm in adults upto 5 mm in children • EDFM > 19mm * May be reducible, partially reducible or irreducible
- 75. THANK YOU
Notas del editor
- Formation of the human craniovertebral junction. Sclerotomal primordia and their vertebral phenotypes are colour-matched. During resegmentation, the caudal half of the fourth somite (fourth occipital somite) and rostral half of the fifth somite combine to form the proatlas sclerotome (PA). Derived from the proatlas are: the axial zones (Ad and Al) which become the basion (B) of the basioccipital or clivus (CL) and the apical segment of the dens (AD); the lateral dense zone (Ld) becomes the exoccipital comprising the occipital condyle (OC), and lateral rim and opisthion (OT) of the foramen magnum; the proatlas’ hypochordal bow (HBp) forms the ventral clival tubercle (CT). The C1 resegmented sclerotome (C1) comes from adjacent halves of the fifth and sixth somites. Derived from the C1 sclerotome are: the axial zones form the basal segment of the dens (BD); the lateral zone forms the posterior atlantal arch (C1P); the hypochordal bow (HBc) forms the anterior atlantal arch (C1A). The C2 resegmented sclerotome (C2) comes from the sixth and seventh somites. From the C2 sclerotome: the axial zone forms the C2 vertebral body (AB); the lateral zone forms the neural arch of C2 vertebra. The intervertebral boundary zone (IBZ) between the proatlas and C1 sclerotome forms the upper dental synchondrosis (US) and the IBZ between the C1 and C2 sclerotomes forms the lower dental synchondrosis (LS)
- The three developmental phases of the axis (C2) and the three waves of ossification. The primordia for the dens components are assembled during the membranous phase. Upper and lower dental synchondroses are shown as dense lines. First wave of ossification at fourth foetal month consists of bilateral centres for the neural arches and a single centre for the centrum. Second wave at sixth foetal month At birth, the basal dental centres should have integrated in the midline and begun to be fused to the centrum. Third wave of C2 ossification occurs from 3 to 5 years post-natal life at the apical dental segment, which does not become fused to the basal dens till the 6–9th year, and fully formed during adolescence.
- Irreg cortic margins Sag view ant arch
- Cervical cord compression
- Boogard’s angle (Angle between the clivus line and McRae's line) < 136 degree Bull’s angle (Line drawn between the posterior and anterior arch of C1. Bull's angle is the angle between this line and the hard palate