Case study on cholelithiasis
•Descargar como PPTX, PDF•
215 recomendaciones•132,193 vistas

a case study on cholelithiasis

Recomendados
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (20)
Similar a Case study on cholelithiasis
Similar a Case study on cholelithiasis (20)
Más de education4227
Más de education4227 (20)
Último
Último (20)
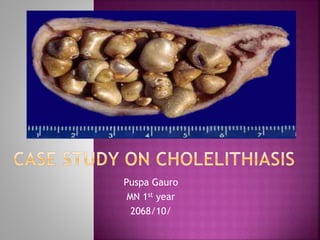
Case study on cholelithiasis
- 1. Puspa Gauro MN 1st year 2068/10/
- 2. To gain in-depth knowledge about the study subject/disease condition. To gain the confidence in handling such cases in future. To fulfill the partial course objective of M.N. curriculum. To share experience and knowledge to friends, juniors and seniors.
- 3. Cholelithiasis is one of the common problems encountered in Nepal. In the United States, about 20 million people (10-20% of adults) have gallstones. Every year 1-3% of people develop gallstones and about 1-3% of people become symptomatic. To provide holistic nursing care to the patient using the nursing process by Appling different nursing theories.
- 4. History taking and interviewing to the patient and his visitors. Observation and, physical examination to the patient Discussion with teachers, senior staffs and doctors Using various text books and references of Medicine and related internet search technology
- 5. Patient’s Name : Ms. Kalpana Pandit Age/ sex :-24yrs/female Marital status : - Married Education : - Literate Occupation : - house wife Religion : - Hindu Address :-Khaireni , Parsa-7, Chitwan Ward :- surgical ward Bed No. : - 28
- 6. Contd… IP No. :- 48870 Provisional Diagnosis :- cholelithiasis Date of admission :- 2068/07/29 Date of operation :2068/07/30 Interview date :- 2068/07/30 Date of discharge :- 2068/08/3 Final Diagnosis :- cholelithiasis Operative procedure : laproscopic cholesystectomy. Attending physician :- Dr Chandra Prakash Pandey Informants Obtained From :- Patient (self) & his husband
- 7. B.Chief complain Fever, vomiting, indigestion, diarrhea. Pain on the right side
- 8. C. Present Illness/ Health Status Ms. Kalpana Pandit had Fever, vomiting, indigestion, diarrhea was occurred before 15th of hospitalization and Pain on the right side was from about 2 months but pain was dull. Then she used to take pain killer from medical hall. Pain gradually increased. She came to the hospital when there was fever, vomiting and diarrhoea. She took the medical treatment from OPD of medical ward 15th before. She was advised to admit on 2068/7/29 for surgery.
- 9. Past health history No history of any childhood illness. No history of hospitalization No history of psychiatric problem. No history of past illness of any kind of Injuries and Accidents. Family history No history of Hypertension, Diabetes, TB or asthma. Socio economic history Middle class family. 9
- 10. Allergies:- no allergies to any food, Drugs and others Medication Taken at Home: she used to take medicine from medical hall in minor cases. Traditional Healer’s Prescription: she believes on traditional healer and obeys them but give emphasize to hospital also
- 11. Medical Practioner’s prescription:- if they get health problem they use to come to hospital and take the prescribed medicine. Self prescription: she use to take certain drugs like cetamol when suffering from fever.
- 12. Client’s Reaction to illness: she was worried about the pain that occur during surgery. Client’s Coping Pattern: she copes illness by expressing her feelings to her husband.
- 13. Client’s Value of Health: She things health is important. Client’s Perception of the Care Giver: She things that nurses are caring and giving health education effectively.
- 14. Family Relationship: Client’s Position in the Family: she use to help in the family. she is not head of the family. Person Living With Client (Support System) : her husband was caring her in hospital. Recent Family Crisis or Changes: there is family crisis, she is unable to care her son as he is of 5years and her child is with his grandmother.
- 15. Menstrual history Regular menstrual period Obstetric history: Antenatal checkup: done in hospital Postnatal checkup: done in hospital Place of Delivery: hospital Type of Delivery: Spontaneous Vaginal delivery Any complication: No
- 16. Personal history Smoking :-No smoking habit Alcohol : - No alcohol habit Food habit : - 3 times a day Food allergy : - Not known Drugs allergy : - Not known Bowel and bladder : - Regular bowl habit Sleeping Pattern : - 6-8 hrs. per day 16
- 17. Environmental history Type of family :- joint Family No. of family :- 5 members Type of house :- cement house NO. of rooms :- 4 Kitchen :- Separated Fuel used :- Firewood , Gas Drinking Water :- tap water Toilet :- pit latrin Drainage System :- open drainage 17
- 19. General Inspection: Gait : Normal Body Build : fat Consciousness : conscious and alert Facial expression : looking anxious Vital signs Temperature : 980 f Pulse :78 b/minute and regular Respiration : 18b /minute, regular Blood Pressure : 100/60 mm Hg in both arms (supine) Height : 5' 2" Weight : 65kg 19
- 20. Examination of head ,face and neck Inspection of head- Hair color and texture normal, clean hair no any injury Inspection of eyes- No discharge and redness of the eye Inspection of ears- No discharge and pain Nose- No discharge , bleeding and smelling problem. Mouth- Poor oral hygiene, no bleeding, Neck- No enlarged lymph node and thyroid gland normal neck mobility is present 20
- 21. Inspection; symmetrical shape, sternum is located at the midline, expansion of the chest , lateral diameter wider than anteriposterior diameter. Palpation : no tenderness, no lump or depression along the ribs, expansion of the chest on both sides Percussion : deep resonent sound over the lungs Auscultation : breath sounds are heared in all areas of lungs, no rales ronchi wheezing sounds. 21
- 22. Inspection: no enlargement of neck vein, Palpation - Non tender, no thrill Auscultation - clear and regular heart rate between 60-80 beats per minute. No murmur sound present. 22
- 23. Higher mental function normal Motor examination e.g. position of limbs normal no atrophy. No abnormal movement. Normal muscle tone. Normal power in all limbs. Deep tendon jerk (bicep, tricep, knee and ankle)normal 23
- 24. localized pain in the right upper quadrant, usually with rebound. Comfort sleep ,rest Slightly anxious about the operation.
- 25. In Books In patient 1. Selecting a mate She had selected mate for her life partner to form marital relationship. 2. Learning to live with a marriage partner She is married since 7 Yrs and live with her husband with happy life 3. Starting a family She has one children and stayed with joint family 4. Rearing children She is house wife. She was rearing her children very well and now she is unable to do due to illness.
- 26. In Books In Patient 5. Managing a home She was Establishing and maintaining a home and managing a time schedule. But now her physical and cognitive capacity is decreased due to illness. 6. Getting started in an occupation She has no other job, she manage home, caring and rearing her children as well as older parents. 7. Taking on civic responsibility She has housewife of the family and is taking care of all family members and also taking part in some social activities, e.g. in festivals, marriage etc. 8. Finding a friendly social group She has good relation in her neighborhoods and friendship group. She also involved in social activities.
- 27. Cholelithiasis is the medical term for gallstone disease. Gallstones are concretions that form in the biliary tract, usually in the gallbladder. Calculi, or gallstones, usually form in the gallbladder from the solid constituents of bile; they vary greatly in size, shape, and composition.
- 28. Cystic duct obstruction, if it persists for more than a few hours, may lead to acute gallbladder inflammation (acute cholecystitis). Common bile duct stone (choledocholithiasis)
- 29. In the United States, about 20 million people (10-20% of adults) have gallstones. Every year 1-3% of people develop gallstones and about 1-3% of people become symptomatic. Each year, in the United States, approximately 500,000 people develop symptoms or complications of gallstones requiring cholecystectomy Gallstones may be present at any age but are unusual before the third decade
- 30. The prevalence is two to three times higher in women than in men, although this difference is less marked in the sixth and seventh decade. At this age the prevalence ranges between 25% and 30%.
- 31. 1.Cholesterol gallstones: Liver cells secrete cholesterol into bile along with phospholipid (lecithin) in the form of small spherical membranous bubbles, termed unilamellar vesicles. Liver cells also secrete bile salts, which are powerful detergents required for digestion and absorption of dietary fats. Bile salts in bile dissolve the unilamellar vesicles to form soluble aggregates called mixed micelles. This happens mainly in the gallbladder, where bile is concentrated by reabsorption of electrolytes and water.
- 32. Compared with vesicles (which can hold up to 1 molecule of cholesterol for every molecule of lecithin). mixed micelles have a lower carrying capacity for cholesterol (about 1 molecule of cholesterol for every 3 molecules of lecithin). If bile contains a relatively high proportion of cholesterol to begin with, then as bile is concentrated, progressive dissolution of vesicles may lead to a state in which the cholesterol- carrying capacity of the micelles and residual vesicles is exceeded. At this point, bile is supersaturated with cholesterol, and cholesterol monohydrate crystals may form
- 33. Bilirubin, a yellow pigment derived from the breakdown of heme, is actively secreted into bile by liver cells. Most of the bilirubin in bile is in the form of glucuronide conjugates, which are quite water soluble and stable, but a small proportion consists of unconjugated bilirubin. Unconjugated bilirubin, like fatty acids, phosphate, carbonate tends to form insoluble precipitates with calcium. Calcium enters bile passively along with other electrolytes. In situations of high heme turnover, such as chronic hemolysis or cirrhosis, unconjugated bilirubin may be present in bile at higher than normal concentrations. Calcium bilirubinate may then crystallize from solution and eventually form stones.
- 34. Gallstone formation is multifactorial, and the factors involved are related to the type of gallstone . Risk factors for cholelithiasis: Obesity Women, especially those who have had multiple pregnancies . Frequent changes in weight
- 35. Rapid weight loss (leads to rapid development of gallstones and high risk of symptomatic disease) Treatment with high-dose estrogen. Low-dose estrogen therapy—a small increase in the risk of gallstones Cystic fibrosis Diabetes mellitus
- 36. Impaired gallbladder emptying Pregnancy Gallbladder stasis Fasting Total parenteral nutrition Spinal cord injury PATHOGENIC FACTORS LEADING TO THE PRODUCTION OF LITHOGENIC BILE Defective bile salt synthesis Excessive intestinal loss of bile salts Excessive cholesterol secretion Abnormal gallbladder function
- 37. According to book According to patient Gallstones may be silent, producing no pain and only mild gastrointestinal symptoms. Epigastric distress, such as fullness, abdominal distention The patient may have biliary colic with excruciating upper right abdominal pain that radiates to the back or right shoulder, is usually associated with nausea and vomiting, and is noticeable. several hours after a heavy meal. The patient develops a fever and may have a palpable abdominal mass. Pain on the right side of the abdomen. No abdominal distention. Vomiting, undigestion and diarrhea present. fever Not present
- 38. According to book According to patient Jaundice occurs in a few patients with gallbladder disease and usually occurs with obstruction of the common bile duct. . The excretion of the bile pigments by the kidneys gives the urine a very dark color. The feces, no longer colored with bile pigments, are grayish, like putty, and usually described as clay-colored Obstruction of bile flow also interferes with absorption of the fatsoluble vitamins A, D, E, and K. Therefore, the patient may exhibit deficiencies (eg, bleeding caused by vitamin K deficiency, Not present Urine normal colour Presence of diarrhea No any sign of bleeding
- 39. Choledocholithiasis Pancreatitis Fistulae between the gallbladder and duodenum or colon Pressure on/inflammation of the common bile duct by a gallstone in the cystic duct Cancer of the gallbladder
- 40. According to book According to my patient History taking Asymptomatic gallstones without causing symptoms or complications evidence to support a causal association between gallstones and chronic abdominal pain, heartburn, postprandial distress, bloating, flatulence, constipation, or diarrhea. Biliary colic pain resolves over 30 to 90 minutes as the gallbladder relaxes and the obstruction is relieved. indigestion, dyspepsia, belching, bloat, and fat intolerance Fever, vomiting, indigestion, diarrhea. Pain on the right side
- 41. physical examination: asymptomatic gallstones have no abnormal findings on physical examination. In acute cholecystitis localized pain in the right upper quadrant, usually with rebound and guarding. a positive Murphy sign (inspiratory arrest on deep palpation of the right upper quadrant during deep inspiration) Tachycardia and diaphoresis may be present as a complications of cholelithiasis consequence of pain In severe cases of acute cholecystitis, ascending cholangitis, or acute pancreatitis, bowel sounds are often absent or hypoactive. Choledocholithiasis with obstruction of the common bile duct produces cutaneous and scleral icterus. Acute gallstone pancreatitis is often characterized by epigastric tenderness Fever, vomiting, indigestion, diarrhea. Pain on the right side
- 42. According to book According to my patient Blood Studies complete blood cell (CBC) count with differential , liver function panel, and amylase and lipase. CBD) obstruction initially produces an acute increase in the level of liver transaminases (alanine and aspartate aminotransferases), followed within hours by a rising serum bilirubin level. •Liver function test done in my patient and values are normal. •alkaline phosphatase done in my patient and slight low value.
- 43. According to book According to my patient If obstruction persists, a progressive decline in the level of transaminases with rising alkaline phosphatase. . Prothrombin time may be elevated in patients with prolonged CBD obstruction, Concurrent obstruction of the pancreatic duct by a stone in the ampulla of Vater may be accompanied by increases in serum lipase and amylase levels. •Prothrombin time is done and it is normal. • Not done.
- 44. According to book According to my patient Abdominal Radiography Black pigment or mixed gallstones may contain sufficient calcium to appear radiopaque on plain films Ultrasonography useful investigation for the diagnosis of gallstone-related disease: (a) gallstones within the gall bladder, particularly when these are obstructing the gall bladder neck or cystic duct (b) focal tenderness over the underlying gall bladder (c) thickening of the gall bladder wall. Computed Tomography CT can be used in diagnostic challenges or to further characterize complications of gallbladder disease •Abdominal radiography not done in my patient. •Utrasonography done in my patient: Two calculi noted in the GB lumen, largest one measuring 10mm.
- 45. From St. Luke’s Health System Resource Library
- 46. According to book According to my patient •Magnetic Resonance Imaging Magnetic resonance imaging (MRI) with magnetic resonance cholangiopancreatography (MRCP) has emerged as an excellent imaging study for noninvasive identification of gallstones anywhere in the biliary tract, including the common bile duct •Endoscopic Retrograde Cholangiopancreatography •Not done in my patient •Not done in my patient
- 47. Date Test In Patient Reference Range 068/7/27 Haematological report WBC Neutrophil Lymphocytes Monocytes Eosinophil Basophil Hb Platelet Count PT( test) PT(control) 16,400 mm3 72% 26% 01% 01% 00% 10.7gm/dl 142000 mm3 16.3 sec 14sec 4000-11,000 mm3 40-70% 20-40% 2-10% 2-6% 0-1% M: 12-18 gm , F: 12- 16 gm/dl 150000- 400000 mm3 13-15sec
- 48. Date Test In Patient Reference Range 068/7/27 INR Bleeding time Clotting time Biochemistry SGOT/AST SGPT Bilirubin Total Bilirubin direct Blood sugar (R) Creatinine alkaline phosphate Blood group/Rh type HIV 1 &11 HbsAg Anti Hcv 1.20 2min 10min 34U/L 36u/L 0.61mg/dl 0.21mg/dl 110mg/dl 0.8 mg/dl 81.0 IU/L o+ve Non reactive Non reactive Non reactive 2-7min 6-12min M-<37 F <31 <40 0.4 - 1.4 0.1 – 0.4 70-120 0.4-1.4mg/dl ( M-64 -306 F: 84-306
- 49. Differentials diagnosis: Appendicitis Bile Duct Strictures Bile Duct Tumors Cholecystitis Gallbladder Cancer Gastritis and Peptic Ulcer Disease Gastroenteritis Pancreatic Cancer
- 50. Treatment of Asymptomatic Gallstones: Surgical treatment Surgical treatment of asymptomatic gallstones without medically complicating diseases is discouraged. cholecystectomy for asymptomatic gallstones may be indicated in the following patients: Patients with large gallstones greater than 2 cm in diameter
- 51. Patients with risk factors for complications of gallstones may be offered elective cholecystectomy.
- 52. Medical dissolution of gallstones Ursodeoxycholic acid (ursodiol) is a gallstone dissolution agent. In humans, long-term administration of ursodeoxycholic acid reduces cholesterol saturation of bile, both by reducing liver cholesterol secretion and by reducing the detergent effect of bile salts in the gallbladder (thereby preserving vesicles that have a high cholesterol carrying capacity). Desaturation of bile prevents crystals from forming and, in fact, may allow gradual extraction of cholesterol from existing stones.
- 53. In patients with established cholesterol gallstones, treatment with ursodeoxycholic acid at a dose of 8-10 mg/kg/d PO divided bid/tid may result in gradual gallstone dissolution. This intervention typically requires 6-18 months and is successful only with small, purely cholesterol stones. The recurrence rate is 50% within 5 years. Moreover, after discontinuation of treatment, most patients form new gallstones over the subsequent 5-10 years.
- 54. Cholecystectomy Removal of the gallbladder (cholecystectomy) is generally indicated in patients who have experienced symptoms or complications of gallstones Open versus laparoscopic cholecystectomy Currently, laparoscopic cholecystectomy is commonly performed in an outpatient setting. By reducing inpatient stay and time lost from work, the laparoscopic approach has also reduced the cost of cholecystectomy. Cholelithiasis patients whose laparoscopic cholecystectomy was uncomplicated may be sent home the same day if postoperative pain and nausea are well controlled
- 55. Stone Removal by Instrumentation. Several nonsurgical methods are used to remove stones that were not removed at the time of cholecystectomy or have become lodged in the common bile duct (Fig. 40-4A, B).
- 56. A catheter and instrument with a basket attached are threaded through the T-tube tract or fistula formed at the time of T-tube insertion; the basket is used to retrieve and remove the stones lodged in the common bile duct. A second procedure involves the use of the ERCP endoscope (see Fig. 40-4C).
- 57. After the endoscope is inserted, a cutting instrument is passed through the endoscope into the ampulla of Vater of the common bile duct. It may be used to cut the submucosal fibers, or papilla, of the sphincter of Oddi, enlarging the opening, which may allow the lodged stones to pass spontaneously into the duodenum. Another instrument with a small basket or balloon at its tip may be inserted through the endoscope to retrieve the stones (see Fig. 40-4D– F ).
- 58. Although complications after this procedure are rare, the patient must be observed closely for bleeding, perforation, and the development of pancreatitis or sepsis.
- 59. Surgical Trocar (both are often 5mm) Optical Trocar Retraction of gall bladder/liv er
- 60. Cystic Duct Cystic Artery Infundibulum of Gall Bladder
- 61. Extracorporeal Shock-Wave Lithotripsy. Extracorporeal shockwave therapy (lithotripsy or ESWL) has been used for nonsurgical fragmentation of gallstones. The word lithotripsy is derived from lithos, meaning stone, and tripsis, meaning rubbing or friction. After the stones are gradually broken up, the stone fragments pass from the gallbladder or common bile duct spontaneously, are removed by endoscopy, or are dissolved with oral bile acid or solvents.
- 63. Intracorporeal Lithotripsy Stones in the gallbladder or common bile duct may be fragmented by means of laser pulse technology. A laser pulse is directed under fluoroscopic guidance with the use of devices that can distinguish between stones and tissue.
- 64. Endoscopic sphincterotomy If surgical removal of common bile duct stones is not immediately feasible, endoscopic retrograde sphincterotomy can be used. In this procedure, the endoscopist cannulates the bile duct via the papilla of Vater. Using an electrocautery sphincterotome, the endoscopist makes an incision measuring approximately 1 cm through the sphincter of Oddi and the intraduodenal portion of the common bile duct, creating an opening through which stones can be extracted.
- 66. laparoscopic cholecystectomy 2068/7/30 Inj Cifran 200mg IV BD Inj Aciloc 50mg IV BD Inj tramadol 50mg IM SOS Inj phenargan 25mg IM SOS Tab Becto 500mg O BD Tab Rloc 150mg O BD Tab Nise 100mg O BD
- 67. The mortality rate for an elective cholecystectomy is 0.5% with less than 10% morbidity. The mortality rate for an emergent cholecystectomy is 3-5% with 30-50% morbidity. Following cholecystectomy, stones may recur in the bile duct.
- 69. Mrs. Kalpana Pandit was admitted for the first time She was anxious about outcome of disease as well as adjusting in new environment. She was fully conscious, alert and she can do care herself by minimal assistance. So, I applied Peplau’s Theory: Interpersonal Relationship with the mutual understanding of patient and family members while caring her.
- 70. Peplau’s Theory: Interpersonal Relationship According to Peplau, nursing is therapeutic in that it is a healing art, assisting in individual who is sick or in need of health care. Nursing can be viewed as an interpersonal process because it involves interaction between two or more individuals with a common goal. In nursing, this common goal provides the incentive for the therapeutic process in which the nurse and patient respect each other as individuals, both of them learning and growing as a result of the interaction.
- 71. Peplau identifies four sequential phases in interpersonal relationship: Orientation phase Identification phase Exploitation phase Resolution phase
- 72. Orientation phase: Nurse and patient come together as strangers; meeting initiated by patient who expresses felt need; work together to recognize, clarify and define facts related to need. It is also called problem defining phase. Identification phase: Interdependent goal setting, patient has feeling of belonging and selectively responds to those who can meet needs. Each patient responds differently in his phase. Selection of appropriate professional assistance.
- 73. Exploitation phase: Patient actively seeking and drawing on knowledge and expertise of those who can help, use of professional assistance for problem solving alternatives. Resolution phase: Occurs after other phases are successfully completed and have been met, leads to termination.
- 74. Asses health history: note history of smoking or prior respiratory problems. Asses respiratory status: note shallow respirations, persistent cough, or ineffective or adventious breath sounds Evaluate Nutritional status is evaluated through a dietary history and general examination performed at the time of preadmission testing Obtain laboratory results to obtain information about the patient’s nutritional status
- 75. Ask for pain in the in the operative site Regarding pain, discussion was made to assess the severity and the type and duration of pain.
- 76. Acute pain and discomfort related to surgical incision Impaired skin integrity related to altered biliary drainage after surgical intervention Imbalanced nutrition, less than body requirements, related to inadequate bile secretion Deficient knowledge about self-care activities related to incision care, dietary modifications (if needed), medications, reportable signs or symptoms (eg, fever, bleeding, vomiting)
- 77. The goals for the patient include: Relief of pain Adequate ventilation intact skin and improve biliary drainage Anxiety related to hospital admission optimal nutritional intake absence of complications understanding of self-care routines.
- 78. Postoperative: Place the patient in the low Fowler’s position. Provide Intravenous fluids. Provide water and other fluids and soft diet is started when bowel sounds return. Relieving pain: Administer analgesic agents as prescribed to relieve the pain Help the patient to turn, cough, breathe deeply, and ambulate as indicated. Use of a pillow or binder over the incision during these maneuvers.
- 79. Improving respiratory status Remind patients to take deep breaths and cough every hour to expand the lungs fully and prevent atelectasis. Promote early ambulation. Early ambulation prevents pulmonary complications as well Monitor elderly and obese patients must closely for respiratory problem. .
- 80. Promoting skin care and biliary drainage: observed for indications of infection, leakage of bile into the peritoneal cavity, and obstruction of bile drainage, clay colored stool and vital sign. note and report right upper quadrant abdominal, pain, nausea and vomiting, Observe for jaundice. changes frequently the outer dressings and protection of the skin from irritation. Maintain a careful record of fluid intake and output
- 81. Improving nutritional status Encourage the patient to eat a diet low in fats and high in carbohydrates and proteins immediately after surgery. At the time of hospital discharge, there are usually no special dietary instructions other than to maintain a nutritious diet and avoid excessive fats.
- 82. Monitoring and managing potential complications Closely monitor vital signs and inspects the surgical incisions and drains, if in place, for evidence of bleeding. Periodically assesses the patient for increased tenderness and rigidity of the abdomen and report to the surgeon. Instructs the patient and family to report to the surgeon any change in the color of stools because this may indicate complications.
- 83. Contd… After laparoscopic cholecystectomy, assesses the patient for loss of appetite, vomiting, pain, distention of the abdomen, and temperature elevation. These may indicate infection or disruption of the gastrointestinal tract and should be reported to the surgeon promptly. Instruct verbally and in writing about the importance of reporting these symptoms promptly after discharge.
- 84. Teaching Patients Self-Care Instruct the patient about the medications that are prescribed (vitamins, anticholinergics, and antispasmodics) and their actions. Inform the patient and family about symptoms that should be reported to the physician, including jaundice, dark urine, pale-colored stools, pruritus, or signs of inflammation and infection, such as pain or fever. Emphasize importance of keeping follow up appointments.
- 85. Asses the knowledge of patient and family of the therapeutic regimen. (medications, gradual return to normal activities) Emphasizes the importance of keeping follow-up appointments and reminds the patient and family of the importance of participating in health promotion activities and recommended health screening. Shower can be taken 48 hours after surgery. No restrictions to physical activities. Gradually increase activities at a comfortable and individual pace.
- 86. Postoperative: Placed the patient in the low Fowler’s position. Provided Intravenous fluids. Provided water and other fluids and soft diet is started when bowel sounds return. Relieving pain: Administerd analgesic agents as prescribed to relieve the pain Helped the patient to turn, cough, breathe deeply, and ambulate as indicated. Used of a pillow or binder over the incision during these maneuvers.
- 87. Improving respiratory status Remind patients to take deep breaths and cough every hour to expand the lungs fully and prevent atelectasis. Promoted early ambulation. Early ambulation prevents pulmonary complications as well Monitored elderly and obese patients must closely for respiratory problem. .
- 88. Promoting skin care and biliary drainage: observed for indications of infection, leakage of bile into the peritoneal cavity, and obstruction of bile drainage, clay colored stool and vital sign. noted and report right upper quadrant abdominal, pain, nausea and vomiting, Observed for jaundice. changed frequently the outer dressings and protection of the skin from irritation. Maintained a careful record of fluid intake and output
- 89. Improving nutritional status Encouraged the patient to eat a diet low in fats and high in carbohydrates and proteins immediately after surgery. At the time of hospital discharge, therewere usually no special dietary instructions other than to maintained a nutritious diet and avoid excessive fats.
- 90. Monitoring and managing potential complications Closely monitord vital signs and inspects the surgical incisions and drains, if in place, for evidence of bleeding. Periodically assessesd the patient for increased tenderness and rigidity of the abdomen and report to the surgeon. Instructed the patient and family to report to the surgeon any change in the color of stools because this may indicate complications
- 91. After laparoscopic cholecystectomy, assessed the patient for loss of appetite, vomiting, pain, distention of the abdomen, and temperature elevation. These may indicate infection or disruption of the gastrointestinal tract and should be reported to the surgeon promptly. Instructed verbally and in writing about the importance of reporting these symptoms promptly after discharge.
- 92. Teaching Patients Self-Care Instructed the patient about the medications that are prescribed (vitamins, anticholinergics, and antispasmodics) and their actions. Informed the patient and family about symptoms that should be reported to the physician, including jaundice, dark urine, pale-colored stools, pruritus, or signs of inflammation and infection, such as pain or fever. Emphasized importance of keeping follow up appointments.
- 93. Assesed the knowledge of patient and family of the therapeutic regimen. (medications, gradual return to normal activities) Emphasized the importance of keeping follow-up appointments and reminds the patient and family of the importance of participating in health promotion activities and recommended health screening. No restrictions to physical activities. Gradually increase activities at a comfortable and individual pace
- 94. Expected patient outcomes Expected patient outcomes may include: Reports decrease in pain Demonstrates appropriate respiratory function Exhibits normal skin integrity around biliary drainage site (if applicable) Obtains relief of dietary intolerance Absence of complications
- 96. Date: - 2068/7/29 Admission day A patient was admitted in surgical ward from opd for laproscopic laprotomy. On admission patient’s vitals sign were: B.P=100/60 mm of hg, R.R=20/min, Pulse=88/min, Temp. =98ºf, SPO2 98% according to nursing report. All investigation report were collected. Patients general condition was fair. Patient was kept NPO from 10pm.
- 97. Date: - 2068/7/ 30 1st day of admission She slept well but slightly anxious about the surgery. She is Alert and conscious History taking and physical examination done B/P- 110/70 mmof Hg, RR- 20/min, P- 92/min, T- 98 ºf, SPO2 99% Preoperative care was done: Send for bath. Psychological support given Consent was taken. Removed all ornaments. IV infusion was given. Gown was given to wear. Chart was completed.
- 98. Date: - 2068/8/1 2nd day of admission(1st post op day) B/P- 110/80 mmof hg, RR- 22/min, P- 80/min, T- 98.2 ºf, SPO2 98% Intake= 2100ml, output= 1450ml Patient GCS 15/15. Patient is self voiding. No soakage and bleeding from operation site. Inj NS Ipint and 5%dex IV pint was given. kept her in fowler position Slept well at night. Morning care was given. Caried out the prescribed medication. Coplain of pain so inj tramadol and inj phenargan was given and relieved after one hour. Patient was ambulated.
- 99. Date: 2068/8/2 3rd day of admission(2nd post op day) Slept well at night. B/P- 120/80 mmof hg, RR- 22/min, P- 78/min, T- 97.2 ºf, SPO2 98%. Patients GCS -15/15 Intake=1950ml, output=1350ml Cannula was removed. Patient transferred to surgical ward. No soakage and bleeding from wound site. Patient was ambulated. patient was given normal diet. Prescribed medication was given.
- 100. Date: 2068/8/3 4th day of admission(3rd post op day) Slept well at night Patients general condition was fair. B/P- 130/80 mmof hg, RR- 20/min, P- 88/min, T- 97.2 ºf, SPO2 98% No any complain. Normal voiding of urine and stool. Patient was discharged. Gave discharge teaching.
- 101. Adequate fluid intake Diet Personal hygiene Rest and sleep Exercise. Prevention of Infection Medication Follow up: after 5 days
- 102. Tab Nise 100mg “0” BD Cap Broclox 500mg 1cap QID 5days Follow Up after 5 days for removal of suture.
- 103. Diversional Therapy “is a client centered practice and recognizes that leisure and recreational experiences are the right of all individuals.” Activities are designed to support, challenge, and enhance the psychological, emotional and physical well being of individuals. These are often quite diverse and can range from: Games, outings, computers gentle exercise, music, arts and craft.
- 104. Gentle exercise. Deep breathing and coughing exercise Talking with other patient Listening music by mobile phone. Gossiping with her Allowing her husband to talk with her.
- 105. Sphygmomanometer Stethoscope X-ray machine Thermometer Pulse oxymeter BP instrument.
- 106. Fever, vomiting, indigestion, diarrhea. Pain on the right side Utrasonography done in my patient: Two calculi noted in the GB lumen, largest one measuring 10mm.
- 107. I learned many things from the case study which are as following: Identified the complete health need, development Task of Young adult and compared it with normal one. Provide comprehensive nursing care by using Nursing Theories to the Young adult patient. Assist in different type of diagnostic procedure for the patient. Analyze the concept and approach to nursing practice according to trend and technology.
- 108. Identified the factors influencing nursing practice. Identified the plan, implement and evaluate the educational need of the patient and patient family. Develop therapeutic relationship to the patient and family and understand their religion, culture, customs and health care belief and practices. Develop competency in handling various gadgets which were used to patient.
- 109. Chintamani, Lewis, Heitkemper, Dirksen, O’Brien and Bucher, (2011). Lewis’s Medical Surgical Nursing: Assessment and Management of Clinical Problems. 7th Ed Black J.M. & Hawks J.M. (2005). Medical –Surgical Nursing: Clinical management for positive outcomes. (7th Ed.). Brunner & Siddhartha's (2004).Medical- Surgical Nursing. (12th Ed.) . Mosby’s Nursing Drug Reference. (2010). 23rd Ed. Davidson’s principle and practice of medicine 20th edition Retrieved on 2068/10/20 from http://emedicine.medscape.com/article/175667- overview#showall. Retrieved on 2068/10/20 from http://www.nlm.nih.gov/medlineplus/ency/article/00 0273.ht
Notas del editor
- atient