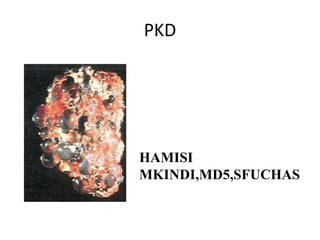
Polycystic Kidney disease
•Descargar como PPTX, PDF•
43 recomendaciones•24,464 vistas

Subset of renal cystic disorders in which cysts are distributed throughtout the cortex and medulla of both kidneys.

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Polycystic Kidney disease
Similar a Polycystic Kidney disease (20)
Más de Mkindi Mkindi
Más de Mkindi Mkindi (11)
Último
Último (20)
Polycystic Kidney disease
- 2. Epedemiology 12.5 million people in the world
- 3. Defn Subset of renal cystic disorders in which cysts are distributed throughtout the cortex and medulla of both kidneys. Numerous and are fluid-filled, resulting in massive enlargement of the kidneys.
- 4. Types There are two types of PKD: autosomal dominant polycystic kidney disease (ADPKD) and the less-common autosomal recessive polycystic kidney disease (ARPKD). The two major forms of polycystic kidney disease are distinguished by their patterns of inheritance. ADPKD(50:50 Chance) and ARPKD(1:4 Chance)
- 5. ADPKD vs ARPKD ADPKD ARPDK Most common Most severe Onset age >30 Infants and children Half get ESRD by 60 Infant renal failure Cerebral aneurysm Liver fibrosis,death
- 6. Pathophysiology The main feature of ADPKD is a bilateral progressive increase in the number of cysts, which may lead to ESRD. Hepatic cysts, cerebral aneurysms, and cardiac valvular abnormalities also may occur. Defect on PKD1 and 2. PKD1 and PKD2 are expressed in most organs and tissues of the human body. The proteins that are encoded by PKD1 and PKD2, polycystin 1 and polycystin 2, seem to function together to regulate the morphologic configuration of epithelial cells.
- 7. Pathophysiology A decrease in urine-concentrating ability is an early manifestation of ADPKD. The cause is not known. Plasma vasopressin levels are increased; this increase may represent the body's attempt to compensate for the reduced concentrating capacity of the kidneys and could contribute to the development of renal cysts, hypertension, and renal insufficiency
- 8. Pathophysiology-Hypertension Cyst-induced bilateral renal ischemia, with subsequent activation of the renin– angiotensin–aldosterone system, is an important factor in the initiation of hypertension in polycystic kidney disease.
- 9. Pathophysiology-Bleeding Renal cysts in ADPKD are associated with excessive angiogenesis evinced by fragile vessels stretched across their distended walls. When traumatized, these vessels may leak blood into the cyst, causing it to expand rapidly, resulting in excruciating pain. If bleeding continues, then the cyst may rupture into the collecting system, causing gross hematuria.
- 10. SIGNS AND SYMPTOMS Pain—in the abdomen, flank, or back—is the most common initial complaint, and it is almost universally present in patients with ADPKD. Dull aching and an uncomfortable sensation of heaviness may result from a large polycystic liver.
- 11. PRESENTATION The pain caused by : Enlargement of one or more cysts Bleeding: May be confined inside the cyst or lead to gross hematuria with passage of clots or a perinephric hematoma UTI (eg, acute pyelonephritis, infected cysts, perinephric abscess) Nephrolithiasis and renal colic Rarely, a coincidental hypernephroma
- 12. PRESENTATION Berry aneurysm Examination in patients with ADPKD may demonstrate the following: Hypertension: One of the most common early manifestations of ADPKD. Palpable, bilateral flank masses: In advanced ADPKD Nodular hepatomegaly: In severe polycystic liver disease Rarely, symptoms related to renal failure (eg, pallor, dry skin, edema)
- 13. TESTING Routine laboratory studies include the following: Serum chemistry profile, including calcium and phosphorus CBC count from cysts Urinalysis Urine culture Genetic testing may be performed, in which the major indication is for genetic screening in young adults with negative ultrasonographic findings who are being considered as potential kidney donors.
- 14. IMAGING Radiologic studies used in the evaluation of ADPKD include the following: Ultrasonography: Technique of choice for patients with ADPKD and for screening patients' family members; useful for exploring abdominal extrarenal features of ADPKD (eg, liver cysts, pancreatic cysts)
- 15. IMAGING CT scanning: Not routine; useful in doubtful pediatric cases or in complicated cases (eg, kidney stone, suspected tumor) MRI: Not routine; helpful in distinguishing renal cell carcinoma from simple cysts; criterion standard to help determine renal volume for clinical trials when testing drugs for ADPKD; best imaging tool to monitor kidney size after treatment to assess progress MRA: Not routine; preferred imaging technique for diagnosing intracranial aneurysms.
- 16. IMAGING-US Ultrasonographic diagnostic criteria for ADPKD1 are as follows: At least 2 cysts in 1 kidney or 1 cyst in each kidney in an at-risk patient younger than 30 years At least 2 cysts in each kidney in an at-risk patient aged 30-59 years At least 4 cysts in each kidney for an at-risk patient aged 60 years or older
- 17. IMAGING-US Ultrasonographic diagnostic criteria for ADPKD in patients with a family history but unknown genotype are as follows: Three or more (unilateral or bilateral) renal cysts in patients aged 15-39 years Two or more cysts in each kidney in patients aged 30-59 years
- 18. IMAGING Indications for MRA are as follows: Family history of stroke or intracranial aneurysms Development of symptoms suggesting an intracranial aneurysm Job or hobby in which a loss of consciousness may be lethal Past history of intracranial aneurysms
- 19. MANAGEMENT No specific medication is available for ADPKD. However, pharmacotherapy is necessary to accomplish the following: Control blood pressure: Drugs of choice are ACEIs or ARBs Control abnormalities related to renal failure Treat urinary tract infections Treat cyst infections: Gyrase inhibitors (eg, ciprofloxacin, chloramphenicol, clindamycin, levofloxacin); dihydrofolic acid inhibitors (TMX/SMP) Treat hematuria: Possibly analgesic plus copious oral hydration Reduce abdominal pain produced by enlarged kidneys Prevent cardiac valve infection in patients with intrinsic valve disease
- 20. Mx-SURGICAL OPTION Surgical intervention in ADPKD includes the following: Surgical drainage: Usually in conjunction with ultrasonographically guided puncture; in cases of infected renal/hepatic cysts not responding to conventional antibiotics Open-/fiberoptic-guided surgery: For excision/drainage of the outer walls of cysts to ablate symptoms Nephrectomy: Last resort for pain control in patients with inaccessible cysts in the renal medullae; bilateral nephrectomy in patients with severe hepatic involvement Partial hepatectomy: To manage massive hepatomegaly Liver transplantation: In cases of portal hypertension due to polycystic liver or hepatomegaly with nonresectable areas
- 21. MANAGEMENT • Patients with ADPKD who progress to end- stage renal disease may require the following procedures: Hemodialysis Peritoneal dialysis Renal transplantation
- 22. Summary • PCKD 12.5 mill people. • Two types: ADPKD and ARPKD • ADPKD most common,asymptomatic to >30 • Sx:Pain,hematuria,HTN,palpable kidneys with nodular surface,nodular hepatomegally, berry aneurysm and mitral valve prolapse can occur. • Dx:Family Hx,clinical findings and US exam. • No specific medication available.
- 23. REFERENCES • 1.http://emedicine.medscape.com/article/244 907-workup • 2.Davidson principle and practice 22nd edition • 3.Pathophysiology of polycystic kidney disease,experimental studies by Jeron Nauta