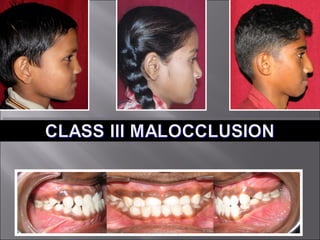
Class iii malocclusion /certified fixed orthodontic courses by Indian dental academy
•
38 recomendaciones•20,803 vistas

The Indian Dental Academy is the Leader in continuing dental education , training dentists in all aspects of dentistry and offering a wide range of dental certified courses in different formats. Indian dental academy provides dental crown & Bridge,rotary endodontics,fixed orthodontics, Dental implants courses.for details pls visit www.indiandentalacademy.com ,or call 0091-9248678078

Recomendados
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Class iii malocclusion /certified fixed orthodontic courses by Indian dental academy
Similar a Class iii malocclusion /certified fixed orthodontic courses by Indian dental academy (20)
Más de Indian dental academy
Más de Indian dental academy (20)
Último
Último (20)
Class iii malocclusion /certified fixed orthodontic courses by Indian dental academy
- 2. INDIAN DENTAL ACADEMY Leader in continuing dental education www.indiandentalacademy.com www.indiandentalacademy.com VT’s
- 4. VT’s Orthodontic treatment not only involves establishment of physiologically and anatomically functional occlusion but also includes correction of the relationship of the maxilla and mandible to each other and to the rest of the craniofacial complex. www.indiandentalacademy.com
- 5. VT’s According to Angle (1899): Class III malocclusion occurred when the lower teeth occluded mesial to their normal relationship by the width of one premolar or even more in extreme cases. (mesioocclusion) Class III malocclusion can be defined as skeletofacial deformity characterized by a forward mandibular position with respect to the cranial base and maxilla. The facial dysphasia can be classified into mandibular prognathism, maxillary retrognathism or combination of both depending variation of the anteroposterior jaw relation www.indiandentalacademy.com
- 6. VT’s It is generally agreed by orthodontists that skeletal Class III malocclusions are difficult to treat by orthodontic means alone. A skeletal class III discrepancy may be the result of a large mandible, a small maxilla, a distally positioned maxilla, or any combination of the three. Most often the patients are advised to wait until the termination of active facial growth so that maxillofacial surgery can be performed www.indiandentalacademy.com
- 7. VT’s Generally of 2 types: Dentoalveolar Skeletal TWEED (1966) CLASS III MALOCCLUSION PSEUDO CLASS III SKELETAL CLASS III Normal Mandible Large Mandible Underdeveloped Maxilla Underdeveloped or Normal Maxilla www.indiandentalacademy.com
- 8. VT’s MOYERS ACCORDING TO THE CAUSE Osseous Muscular Dental www.indiandentalacademy.com
- 9. FREQUENCY OF CLASS III MALOCCLUSION VT’s 1) Caucasians 1 to 4 % Swedish population: 2) African – Americans 7 to 13 Years - 4.2% 14 to 18 Years - 9.4% 5 to 8% 3) Asian Maxillary deficiency Japanese: 4 % younger / 14 % older Chinese: 3 % younger / 13 % older Indians: 1.3% (J Ind. Ped & Prev Dent: 1998 – Uteraja et al) Iranian: 2.1% (East Mediters Health J: 2006: Danaie et al) www.indiandentalacademy.com
- 10. VT’s McGuigan (1966) – Inheritance of class III malocclusion in Hapsburg Family, having the distinct characteristics of prognathic lower jaw. Litton et al (1970) – Dental characteristics of class III are related to genetic inheritance. Rakosi & Schilli (1981) Functional factors: Anteriorly positioned tongue believed to be a local epigenetic factor. Also associated with syndromes like Apert and Cruzons. www.indiandentalacademy.com
- 11. VT’s Mental diseases – Compulsive habits of protruding the mandible. Enlarged tonsils and naso-respiratory diseases – Results in anterior tongue posturing. Premature loss of decidious molars – Results in anterior mandibular displacement. Tongue thrusting habit – Prevents eruption of buccal segments, thus causing auto-rotation of mandible into excessive intra occlusal space. www.indiandentalacademy.com
- 12. The posterior ‘squeezing out’ effect of molar crowding: due to crowding in the molar regions, which can contribute to an anterior open-bite malocclusion in a mandible with poor vertical growth in the ramus area . Alternatively, good ramus growth can lead to a Class III malocclusion. This concept is not well understood, and has not been fully investigated VT’s
- 13. Guyer et al (1986) 13-15 years- 57% - Normal to prognathic Mand. with Retrusive Max. www.indiandentalacademy.com Ngan P et al: AJODO : 1996 VT’s
- 14. Ellis & Mc Namara 1996: 243 possible types of Class III VT’s Wu, Lin 1986: 75 % of all Chinese Class III have max. retrusion and increased lower facial heights. COMPONENTS OF CLASS III MALOCCLUSION Vertical components : •Vertical Deficient •Vertical Normal •Vertically excess Anterio-Posterior components : • Maxillary Deficient • Mandibular excess • Combined Maxillary deficient and mandibular excess www.indiandentalacademy.com
- 16. DENTAL ASSESSMENT FOR DIAGNOSIS OF CLASS III MALOCCLUSION (molar relation and over jet) VT’s www.indiandentalacademy.com Ngan P et al: Pediat Dent : 1997
- 17. 1) Cranial Base Angle – More Acute Middle Cranial Fossa Posterio-Superior Alignment 2) Maxilla Decreased horizontal maxillary growth when compared with the patients with class I malocclusion. 3) Mandible Gonial Angle Obtuse Anteriorly placed 4) Dentoalveolar compensation Proclination of upper incisors, Retroclination of lower incisors. www.indiandentalacademy.com VT’s
- 18. VT’s In 1970 Dietrich reported that Class III skeletal discrepancies change with age. DENTAL AGE MAXILLARY ANTEROPOSTERIOR DEFICIENCY Stage I Primary 23% 26% Stage II Mixed 30% 44% Stage III Permanent NEGATIVE ANB ANGLE 34% 37%. These all results indicates that the abnormal skeletal characteristics can become move pronounced with time. www.indiandentalacademy.com
- 19. VT’s Growth prediction can be used to define Class III tendency and identify specific skeletal morphologic pattern. Certain cephalometric measurements such as cranial flexure, Porion location and ramus position have been used predict normal or abnormal growth. Mito and Co-workers suggested that accuracy of prediction is around 70-80% by use of cervical vertebral to predicted mandibular growthpotential. www.indiandentalacademy.com
- 20. VT’s GTRV analysis is performed in early permanent dentition. This helps clinicians to decide whether the malocclusion can be camouflaged by orthodontic or by surgical intervention once the growth is completed. GTRV =Horizontal growth changes of maxilla Horizontal growth changes of mandible GRTV ratio normal individual 0.77 mm at 8-16 year.
- 21. VT’s In case of Class III patient have GTRV Ratio 0.33-0.38 mm maxillary deficiency and can be successfully treated by with camouflage Class III patient with excessive mandibular growth with GTRV<0.38 mm then it indicated Orthognathic surgery. www.indiandentalacademy.com
- 22. VT’s The craniofacial skeletal pattern of children with Class III malocclusion is evident in the early deciduous dentition. A sample of 69 Class III subjects were compared with 60 subjects exhibiting normal occlusion. They showed both maxillary retrusion and mandibular protrusion with additional other skeletal characteristics are short anterior cranial base length, larger mandibular ramus height and corpus length. www.indiandentalacademy.com
- 23. Class III skeletal imbalance shows either edge to edge incisor relationship or an anterior crossbite in deciduous dentition. The skeletal components of the class III malocclusion tend to worsen along with subsequent growth. MEAN ANNUAL GROWTH INCREMENT EARLY MIXED DENTITION LATE MIXED DENTITION MAXILLA 0.8mm / 1.1 mm 1.1 mm / 1.4 mm MANDIBLE 4.5mm / 2.6 mm 4.4 mm / 2.8 mm Class III Normal growers www.indiandentalacademy.com VT’s
- 24. VT’s Early signs of true progressive mandibular prognathism occasionally can occur in infancy. In the first months of life a sequential development of the class III condition may be observed as: Eruption of the maxillary central incisors in a lingual relationship and the mandibular incisors in a forward position with no overjet. Development of an incisal crossbite during the eruption of the lateral incisors into a normal relationship. www.indiandentalacademy.com GPR
- 25. Full incisor cross bites develops some weeks later. Flattening of the tongue as it drops away from the palatal, contact and postures forward, pressing against the lower incisors Habitual protraction of the mandible by the child into the protruded functional and morphologic relationship VT’s GPR
- 26. VT’s The configuration and form of the forehead and nose in relation to the lower face are significant for esthetic evaluation and prognosis. A well formed Naso labial angle is important for esthetic improvement. Acute: the premaxilla segment can be retracted Obtuse; the segment must be protracted to improve facial esthetics. The soft tissue of the chin can compensate for or accentuate a skeletal class III relationship depending on its thickness. Gingival recession or dehiscence can often be seen in early class III malocclusion. This damage is irreversible and is an indication for early treatment www.indiandentalacademy.com GPR
- 27. The next step is Examination Of The Dentition, including the morphology and number of teeth. Congenital absence (e.g., in the maxilla: missing canine or first premolar teeth) makes treatment more difficult. When evaluating the axial inclination of the teeth, certain disadvantageous irregularities such as labial tipping of the upper incisors and lingual tipping of the lower incisors still in anterior cross bite should be noted. A concavity of the lingual alveolar structure in the mandible also is a clue to future difficulties in the correction of Class III malocclusion. GPR www.indiandentalacademy.com VT’s
- 28. Crowding of maxillary teeth also enhances treatment problems; treatment may require extraction of the counterpart teeth in the lower arch, leading to great difficulty in closing spaces and maintaining proper incisor axial inclination. To make treatment easier if extractions are required, the clinician should perform extractions in the mandible before proceeding to those in the maxilla. Depending on the state of development, enucleation or germectomy may be feasible for the lower first premolars. The molar occlusal relationship is usually Class III, but the plane of occlusion also should be evaluated because its GPR www.indiandentalacademy.com correction may be necessary before surgery VT’s
- 29. VT’s The Path Of Closure: from the postural rest position to occlusion must be carefully studied. The mandible may slide anteriorly into a forced protrusion because of premature contact and tooth guidance when the jaw closes into full occlusion. Such anterior displacements have more favorable prognosis. In contrast, patients with problems caused by an anterior rest position with respect to habitual occlusion are difficult to treat and usually require orthognathic surgery. www.indiandentalacademy.com GPR
- 30. VT’s In addition, a Skeletal Class III with a dental compensation arising from labial tipping of the upper incisors on a deficient maxillary base and lingual tipping of the lower incisors on an excessively long mandible. Orthodontic pre surgical treatment must decompensate these malpositions before surgical procedures can be performed. www.indiandentalacademy.com GPR
- 31. VT’s If the condyle occupies the most posterior position in the temporal fossa the likelihood of its riding over the posterior periphery of the articular disk is increased with concomitant clicking and lateral crepitus,. Abnormal tongue function, size and posture must be considered. The tongue may be postured low in the mouth and be flat and elongated, especially in cases of mouth breathing. In cases of Macroglossia the tongue is not contained within the dentition and the scalloping effect of the tooth www.indiandentalacademy.com contact may be visible on the periphery.
- 32. VT’s A short hypotonic retrusive upper lip is often seen in combination with a heavy, redundant, everted lower lip. A closed lip position will produce the appearance of a long lower lip, as the lip elongates to close over the class III incisor relationship. The closed lip length is misleading and should not be used for treatment planning. Relaxed lip appearance is deceiving due to hypotonicity of lower lip --this causes elevation and apparent www.indiandentalacademy.com
- 33. VT’s The lower lip length should be verified with the lower incisor tip to soft tissue menton which is not influenced by posture Maxillary retrusion is associated with upper lip retrusion and a straight maxillary sulcus curve. Upper lip retrusion is treated with labial crown torque. www.indiandentalacademy.com
- 34. VT’s 1. 2. 3. 4. 5. 6. An increased gonial angle Antegonial notching Backward direction of condylar growth Thin mandibular symphysis Compensation in position of upper and lower incisors in response to disproportionate jaw growth. Mandibular incisors are retroclined as child becomes older there roots tend to press against the labial plate producing a WASH BOARD EFFECT. Maxillary incisors are usually flared anteriorly. GPR www.indiandentalacademy.com
- 35. Several studies have been done in an attempt to compare Class III malocclusion with Class I controls relative to the morphology of the maxilla, the mandible, and the cranial base. These differences include the following: 1. The SNA angle is significantly lower in the Class III samples, indicating a greater degree of maxillary retrusion. 2. Mandibular protrusion is greater in the Class III samples. 3. The mean ANB angle in the Class III samples is negative. www.indiandentalacademy.com VT’s
- 36. VT’s 4. The gonial angle is more obtuse in the Class III samples. 5. The mandibular plane angle is steeper than normal in the Class III samples. 6. Lower anterior face height is significantly greater in the Class III samples. 7. The sella angle and articular angle were smaller in class III samples. 8. Anterior position of the mandible is seen. www.indiandentalacademy.com
- 37. CEPHALOMETRIC CLASSIFICATION Dentoalveolar Class III: No apparent sagittal skeletal discrepancy (normal ANB angle) Tipping of incisors : upper- lingual and lower -labial Skeletal Class III: Max retrusion Mand prognathism Combination Negative to 00 ANB angle and Wits appraisal Increased mand length and more obtuse gonial angle Tipping of incisors: upper- labial & lower lingual (compensation) Pseudo Class III (Kwong & Lin 1987) Ceph values intermediate to class I & III. Except for functional positioning of Mand in a more protrusive position probably due to premature contacts (CO-CR discrepancy ) or Habits. www.indiandentalacademy.com VT’s
- 38. VT’s EARLY TREATMENT IN GROWING CHILDREN FUNCTIONAL AND ORTHOPEDIC APPLIANCES LATE TREATMENT IN LATE ADOLOSENCE AND NON GROWING ADULTS ORTHODONTICS + SURGERY www.indiandentalacademy.com NAGN et al 2001
- 39. VT’s Class III malocclusion is established early in life and is not a self correcting disharmony. Cephalometric and morphometric gives treatment of Class III malocclusion. It is carried out more efficiently during early mixed dentition than late mixed dentition. At post pubertal observation (Cs5 and Cs6) when active growth of the skeleton is completed. Class III subjects treated with rapid maxillary expander and facial mask well before the growth (CS1) present and there will be peak mandibular growth at Cs3 stage. Early orthodontic treatment: J Daniel Subtenly www.indiandentalacademy.com
- 40. VT’s To prevent irreversible soft tissue or on bony changes. Often associated with anterior crossbite leads to abnormal wear of lower incisor. Dental decomposition of mandibular incisors leads to tinning of alveolar place and gingival recession. To improve skeletal discrepancies. Early orthopedic treatment using facemask or chin cup therapy improve skeletal relations which minimize excessive dental decompensation i.e. over closure of mandible and retroclination of mandibular incisor. Early treatment eliminate the functional shift, CRCO discrepancies and prevents severe Orthognathic surgeries . AJODO 2006 www.indiandentalacademy.com Early treatment provides pleasing profile thus Apr Suppl
- 41. EARLY CORRECTION OF MANDIBULAR DISPLACEMENTS These should be identified at dental age 8 or 9, soon after the permanent incisors erupt. This incisor relationship has the potential to restrict maxillary development and encourage mandibular growth, thereby worsening the Class III problem. (This is similar to the effect of a functional appliance in Class II treatment.) Normally, such displacements can be corrected by simple tooth movements, and it is important for treatment to be provided at an early age. Subsequently, unrestricted maxillary development can resume, and if the condyles are centered in the fossae, this will AJODO 2006 www.indiandentalacademy.com eliminate the potential ‘functional Apr Suppl VT’s
- 42. MAXILLARY RETROGNATHISM VT’s Growing patients who present with maxillary retrognathism should be considered for early expansion and development of the maxilla. Use of rapid maxillary expansion and a reverse headgear. Subsequently, a palatal bar can be used to stabilize the skeletal change, and then full fixed appliance treatment can be commenced at approximately 12 years of age. BORDERLINE SURGICAL CASES In some cases with mandibular excess, the diagnosis will suggest that mandibular surgery may be needed. It is helpful to delay orthodontic treatment for such cases, if possible. This will allow assessment of growth patterns, using regular cephalometric radiographs, so that a more informed www.indiandentalacademy.com AJODO surgical/non-surgical decision can be reached. 2006 Apr Suppl
- 43. VT’s CLASS III SURGICAL CASES Some cases are clearly Class III surgical cases from the outset, and SHOULD NOT BE TREATED UNTIL ALL GROWTH HAS CEASED. Timing will be beyond the age of 20 years in males and a little earlier in females. www.indiandentalacademy.com AJODO 2006 Apr Suppl
- 44. Rickets (AJO 2000) has summarized the main objectives of early treatment lying in five concepts 1. Obtaining a skeletal change (structural) 2. Providing the opportunity of a functional change in the environment 3. Utilization of the individual growth towards the correction. 4. Elimination of the detrimental habits (breathing etc) 5. Taking advantage of the forces of the occlusal development towards the correction. www.indiandentalacademy.com VT’s AJODO 2000
- 45. Turpin has developed a list of positive and negative factors to aid in deciding when to interrupt a developing class III malocclusion POSITIVE FACTORS 1. Good facial esthetics 2. Mild skeletal disharmony 3. No familial prognathism 4. Antero posterior functional shift 5. Convergent facial type 6. Symmetric condylar growth 7. Growing patients with expected good cooperation. 8. If the above factors are not present in the patient , they are listed as negative and treatment can be www.indiandentalacademy.com delayed until growth is completed. AJODO 2006 Apr Suppl VT’s
- 46. Joondeph, after Turpin’s thesis, also pointed out the goals of early intervention: 1. Reduce the skeletal discrepancy and provide a more favorable environment for normal growth. 2. Achieve as much relative maxillary advancement as possible. 3. Improve occlusal relationships. 4. Improve facial esthetics for more psychosocial development. 5. Reduce or simplify, phase II or surgical treatment. www.indiandentalacademy.com VT’s AJODO 2006 Apr Suppl
- 47. VT’s Extraction therapy may have limited applicability in Class III treatment. For example, we would not want to limit extractions to the lower arch because many times the incisors are generally inclined lingually and extraction treatment tends to increase this inclination, possibly beyond the limits of the lingual plate of bone. Also, extractions may be contraindicated when orthodontic treatment must be combined with surgical treatment. www.indiandentalacademy.com
- 48. Another consideration is that many of the forces in conventional orthodontics carry risks because of the unfavorable growth pattern in patients with Class III malocclusions. VT’s For example, many patients with Class III malocclusions have an increased vertical face height, particularly of the lower anterior part of the face, with an open-bite. In these patients, Class III elastics and second-order bends in the posterior regions cannot be used conveniently because the extrusive force components on posterior teeth can open the bite and increase the vertical dimension further. Particular attention must be paid to the use of Class III elastics because they can also extrude the mandibular incisors, and there is frequently excessive vertical dentoalveolar development in the incisor region. Since many of the conventional treatment procedures have limitations, we should consider the use of extra oral traction because appropriate force systems can be placed with fewer deleterious www.indiandentalacademy.com
- 49. There are three important diagnostic principles which merits attention. First Principle: it is particularly important to determine whether the mandible, on closure, is in centric relation or in a "convenient" anterior position. The practical implication is that a Class I problem can appear to be a Class III malocclusion (Pseudo-Class III malocclusion) when the mandible is forced anteriorly . Even a true Class III malocclusion can appear much more serious if there is an anterior path of closure of the mandible www.indiandentalacademy.com VT’s
- 50. VT’s Type Pseudo-Class III Anterior position of mandible Present Centric relation and centric occlusion Significance Not coincident Problem is less difficult than it appears ( in a Class I) actually. True Class III Present Not coincident Not coincident Problem is less difficult than it appears True Class III Absent Coincident Problem is as difficult as it appears
- 51. Second Principle: is that the nature of the skeletal discrepancy must be defined because treatment, to a large extent, is based on this differential diagnosis. Class III malocclusions can be classified as An under developed maxilla---TYPE A An over developed mandible--TYPE B A combination of TYPE A and TYPE B www.indiandentalacademy.com VT’s
- 52. Third Principle: a malocclusion reflects the interplay of many conditions that may be impossible to evaluate singularly. One important variable is the potential growth and development of a patient with a Class III malocclusion. In this context, at least two factors may be detrimental and aggravate Class III malocclusions with time. One is the differential growth of the jaws, carrying the mandible more anteriorly relative to the maxilla. Also, local conditions (such as low tongue posture) may adversely influence the growth pattern. Since the amount and the timing of growth of the mandible cannot be assessed accurately, we cannot consider a Class III malocclusion fully resolved until facial growth has ended. www.indiandentalacademy.com VT’s
- 53. VT’s 1. 2. Characteristic of this type in which the maxilla appears retrognathic is a concave profile which represents underdevelopment of the middle part of the face, rather than prominence of the mandible. Treatment should be started early, (as early as 4 years of age) for two fundamental reasons. Extraoral traction which pulls the maxilla anteriorly functions in the same direction as the direction of development. Unlike posterior movement of the mandibular arch, anterior movement of the maxillary arch appears to have a greater chance of remaining stable. www.indiandentalacademy.com
- 54. RESULTS ACHIEVED: VT’s An orthopedic protraction of the maxilla with a strong force (500 to 1,000 Gm per side). This change appears to be limited especially if treatment is started after 6 years of age, An increase in the inclination of the maxillary incisors to obtain a sufficient overjet, associated more or less with Bodily movement of all the teeth in an anterior direction, advancing point A. RESULT: Both an improvement in function and a more esthetic profile. www.indiandentalacademy.com
- 55. The use of Protraction Headgear - > 100 years ago Early orthopedic intervention - non surgical alternative in the treatment of Class III malocclusion with maxillary retrusion. Protraction headgear – FORCE -directed forwards in the same direction of growth of the maxilla An EXTRA ORAL FORCE of 300 gm or more per side, when applied, can cause significant changes in the circum maxillary sutures and in the maxillary tuberosity. Tension produced within the sutures was believed to cause an increase in vascularity and a concomitant differentiation of the cellular tissues resulting in increased osteoblastic activity. www.indiandentalacademy.com VT’s
- 56. RESULTS PRODUCED : In an animal study with tantalum implants and oxytetracycline dyes, heavy intermittent maxillary protraction was found to produce forward displacement of the mid face, anterior relocation of the inferior border of the orbit, and gross osseous alterations extending superiorly to the area of the fronto maxillary suture. The study also found that post treatment skeletal rebound was minimal and was observed only during the first month after discontinuation of mechanical forces. Clinically, the maxilla can be advanced 2 to 4 mm over a 12 to 15-month period of headgear treatment. The use of protraction headgear has been shown to be most effective in the full deciduous or early transitional dentition, with less skeletal changes after 9 years of age. But, a recent longitudinal study suggested that orthopedic effects of protraction headgear on dentofacial structure was possible in young girls as late as during the acceleration phase of pubertal growth spurt. www.indiandentalacademy.com VT’s
- 57. APPLIANCE DESIGN: The orthopedic facial mask consists of three basic components. FACIAL MASK BONDED/ BANDED MAXILLARY SPLINT ELASTICS The facial mask : an extra oral device composed of a fore head pad a chin pad that are connected with a heavy steel support rod. To this support rod is connected a cross bow to which are attached rubber bands to produce a forward and downward elastic traction of the maxilla. The position of the pads and the cross bow can be adjusted simply bywww.indiandentalacademy.comand tightening set loosening VT’s
- 58. VT’s The major modification in the appliance is the addition of facial mask hooks in the upper first deciduous molar. In patients in whom treatment is started before the eruption of the upper first molars, the appliance is designed to incorporate the first and second deciduous molars as well as deciduous canines www.indiandentalacademy.com
- 61. The splint is activated once per day until the desired increase in transverse width has been achieved. In patient in whom no increase in transverse dimension is desired, the appliance still activated for 8-10 days to disrupt the maxillary sutural system and to promote maxillary protraction (HASS 1965) After the patient has been accustomed to wearing the maxillary splint, the facial mask treatment is initiated. The current version of the petit facial mask is one universal size and can be adjusted to fit the facial contours of most patients. www.indiandentalacademy.com VT’s
- 62. SEQUENCE OF ELASTICS: At the time of delivery After 2 weeks Increased to a max. of 3/8” 1/2” 5/16” 8 oz 14 oz 14 oz 2 weeks Timing of wear: Young patients (4 - 9 years) should wear the mask on a full time basis except during meals. In older patients, it is worn at all times except during school Duration is 4-6 months. Retained: with only night time wear or with a maintenance plate, chin cup, FR III or a modified utility arch with Class III elastics. www.indiandentalacademy.com VT’s
- 63. SKELETAL EFFECTS OF MAXILLARY PROTRACTION ( sutures involved): The maxilla articulates with nine other bones of the craniofacial complex: frontal, nasal, lacrimal, ethmoid, palatine, vomer, zygoma, inferior nasal concha, opposite maxilla, and occasionally sphenoid. Palatal expansion had been shown to produce a forward and downward movement of the maxilla by affecting the intermaxillary and circummaxillary sutures. The disruption of these sutures may help initiating cellular response in the sutures, allowing a more positive reaction to protraction www.indiandentalacademy.com VT’s
- 65. Kambara found changes at the circummaxillary sutures and at the maxillary tuberosity attributable to posteroanterior traction, including the opening of sutures, stretching of sutural connective-tissue fibers, new bone deposition along the stretched fibers, and apparent tissue homeostasis that maintained the sutural width. Nanda and Hickory showed how the histologic modifications in the zygomatico maxillary suture after maxillary protraction varied according to the orientation of the force system applied. VT’s www.indiandentalacademy.com
- 66. BIOMECHANICS: VT’s The centre of resistance of the maxilla is located at the distal contacts of the maxillary first molars, one half the distance from the functional occlusal plane to the inferior border of the orbit.( Lee AJO 1997) Protraction of maxilla below the Centre of resistance produces counter clock wise rotation of the maxilla. Also Hata et al (AJO 1987) found using human skulls that protraction forces at the level of the maxillary arch produces forward but counter clock wise rotation unless a heavy downward vector of force was applied. www.indiandentalacademy.com
- 68. VT’s A heavy force at 300 -450 gms on either side at about 300 to the functional occlusal plane in both primary and mixed dentition is recommended by most authors producing 10 degree of counter clock wise rotation being acceptable . Direction of force: Downwards and forwards Point of Application: 5 mm above the palatal plane in the canine region. Hata et al suggested that an effective forward displacement of the maxilla can be obtained with this point of application www.indiandentalacademy.com
- 69. EFFECTS OF THE FACE MASK VT’s 1. 2. 3. 4. 5. The maxillary incisors moved in the anterior direction, whereas the mandibular incisors moved posteriorly. After maxillary protraction, the maxilla was displaced anteriorly, whereas the mandible rotated posteriorly. The mandibular plane angle and anterior lower and total face heights increased. There is no change in SN-palatal plane angle during growth period. These changes were reflected in the profile, whereby the skeletal profile convexity increased and soft tissue facial angle and facial convexity increased; and the Class III concave profile became more balanced, with the upper lip area www.indiandentalacademy.com
- 70. 6. 7. 8. 9. 10. Position of the posterior nasal spine remained stable Over bite was improved by eruption of maxillary and mandibular molars. Anchorage loss was observed during maxillary protraction with mesial movement of the maxillary molars. An average of 5.68 mm anterior movement of the upper incisors resulted in a significant amount of upper lip protraction. The ratio of upper lip protraction to upper incisor protraction relative to the vertical reference line was 1:1.26 A significant decrease in upper lip thickness to vermilion was caused by the fact that during the treatment period, total anterior movement of the upper incisors was approximately 1 mm more than that of the upper lip. www.indiandentalacademy.com VT’s
- 71. 11. 12. 13. 14. 15. A significant decrease in the upper lip sulcus depth can be evaluated as another favorable effect of the appliance on the soft tissue profile. The lower lip moved posteriorly to lie behind the Steiner S line After the correction of the crossbite in Class III cases, the lower lip most often contacts both lower and upper incisors and would therefore be influenced not only by the retraction of the lower incisors but by protraction of the upper incisors as well. Backward repositioning of the pog’, and slight inhibition of anterior migration of the lower lip was seen. Upward and Forward Rotation of the maxilla occurs when protraction force on molars is applied parallel to the occlusal plane. This type of maxillary rotation can be minimized when the force is applied in the www.indiandentalacademy.com canine area, 20° to 30° below the occlusal plane. VT’s
- 73. Rapid maxillary expansion is the corner stone of increasing the transverse dimension in growing individual. In general there are three types of expansions are there to increase the transverse dimension 1.ORTHODONTIC EXPANSION 2.PASSIVE EXPANSION 3.ORTHOPEDIC EXPANSION www.indiandentalacademy.com VT’s
- 74. # Indications for RME VT’s Patients who have LATERAL DISCREPANCIES resulting in either unilateral or bilateral posterior crossbites ANTERO-POSTERIOR DISCREPANCIES Cleft lip and palate patients with collapsed maxillae . Procedure to gain arch length in patients who have moderate maxillary crowding. www.indiandentalacademy.com
- 75. # Contraindications for RME Non cooperate patients Patients who have a single tooth in crossbite Patients who have anterior open bites, steep mandibular planes, and convex profiles Patients who have gross skeletal asymmetry of the maxilla or mandible Adults with severe anteroposterior and vertical skeletal discrepancies www.indiandentalacademy.com VT’s
- 76. VT’s Does RME enhance the efficiency of maxillary protraction with face mask in developing Class III malocclusion? Results: Face mask therapy effective in early Class III MO The need for palatal expansion in the absence of a transverse discrepancy or a skeletal/ dental cross bite is not supported. Correction due to combined skeletal and dental change. www.indiandentalacademy.com AJO DO 2005 128; 299-309
- 77. VT’s The skeletal change following protraction is significant. But has no correlation with expansion. www.indiandentalacademy.com Kalha A S: EBD 2006:7,16-17
- 78. VT’s A modified protraction headgear design and the biomechanical considerations of its clinical use are presented by Nanda (1980 AJO). The clinical results show that a modified protraction headgear with a chin cup helps in the correction of moderately severe Class III malocclusions by the anterior displacement of the maxilla and maxillary dentition, and possibly restricting or changing the direction of the growth of the mandible. This headgear can also be used to correct axial inclinations and or mesial displacement of posterior teeth www.indiandentalacademy.com
- 79. VT’s This functions to produce anterior movement to the maxilla and to redirect the anterior movement of the mandible. This appliance can be used when strong forces are not necessary. Under these conditions, however, the orthopedic effect may be limited. www.indiandentalacademy.com
- 80. VT’s Use of removable appliances which are placed in the deciduous dentition stage of development or in the mixed-dentition stage when certain teeth have exfoliated or are carious. If retention of the removable appliance is adequate, we can apply up to 500 Gm. per side. Some of the mild class III can be treated with bite planes in the anterior region (Nanda 2006) www.indiandentalacademy.com
- 81. VT’s Characteristic of this type of malocclusion is the overdevelopment of the mandible, especially in relation to the maxilla. The treatment of choice would be to inhibit or redirect the growth of the mandible. For this purpose, a few appliances are available. www.indiandentalacademy.com
- 82. VT’s Orthopedic force with the chincup or mental anchorage - serves to redirect mandibular growth Appliances resembling chin cups have been in use since the early 1800's. Thilander treated sixty patients with chin cups for 1 to 6 years. A significant percentage of patients did not improve. The patients who showed improvement were comparatively young and showed favorable dental changes. The force generated by the chin cup in his study was only 150 to 200 Gm. www.indiandentalacademy.com
- 83. Types of chincup VT’s VERTICAL PULL CHIN CUP www.indiandentalacademy.com
- 84. VT’s According to Graber, the early attempts with the chin cup were not successful because of incomplete knowledge of mandibular and facial growth, its use on non growing patients, and an inadequate understanding of the forces generated by the chin cup. Armstrong applied 500 Gm. of force via chin cups on 100 adolescent patients with mandibular prognathism. He reported that half of his patients showed improvement in the Class III profile, whereas none of the control / non treated patients showed any favorable change. www.indiandentalacademy.com
- 85. VT’s Graber, Chung, and Aoba reported results in patients treated with chin cups for 12 to 14 hours each day with a force of 1.5 to 2 pounds on each side. They showed that mandibular growth could be redirected with a chin cup. They asserted that continuous use of the appliance for a long period or through active growth was necessary to achieve stable results. Graber treated 35 Class III malocclusions in children between the ages of 5 and 8 years with chin cup therapy for 3 years. He found that the therapy was particularly effective in patients with increased vertical growth of the face. www.indiandentalacademy.com
- 86. VT’s Chin cup therapy primarily works on the hypothesis that “A force directed through the condyles will inhibit as well as redirect the condylar growth.” However, this therapy alone may not be indicated for a fair percentage of patients in skeletal Class III who show a small midfacial bone or a retropositioned maxilla with relatively normal mandibular dimensions. Jacobson et al studied 149 Class III patients and noted that in approximately one fourth of the sample the problem was due to maxillary deficiency. Several clinical studies in the past have noted that treatment of patients in skeletal Class III www.indiandentalacademy.com
- 87. As the neck of the condyle reverts back toward its former position post treatment, as it usually does (De Vincenzo 1991), one of four post treatment reactions must occur; 1. The molar relation must revert back toward Class III occlusion, 2. The lower molars must move forward on the mandible, 3. There must be a change in the temporal mandibular joint, or 4. There must be a dual bite. VT’s The authors of the Class III study speak of “shrinkage” of the condylion- pogonion distance, but this is a misnomer. The distance does not become smaller, it only fails to increase in proportion to the growth of the condyle, because of the reduction of the gonion angle. The backward bending of the neck of the condyle www.indiandentalacademy.com followed
- 88. VT’s This generally requires a combination type of therapy to produce anterior movement of the maxilla and posterior movement of the mandible. This is chosen when the malocclusion reflects underdevelopment of the maxilla associated with hyper development of the mandible. It can also be done when, during treatment, to accept a compromise result between relationships of the mandible and maxilla. Maxillary protraction and mandibular retraction can be achieved by using, in successive treatment periods, two types of extraoral traction. For example, initially, a facial mask may be used to gain space for the maxillary teeth and to protract the maxillary arch. In a subsequent treatment period, an extraoral appliance can be used to move the mandibular arch distally or, at least, to control the incisor region and possibly influence mandibular growth and www.indiandentalacademy.com development
- 89. VT’s The activator was introduced by Andresen and has been long served for correction of skeletal Class II malocclusions. Rakosi suggested modification of the activator for use in Class III treatment. The appliance consists of wire and acrylic parts. The wire components are 4 stop-loops located mesial to all first molars to prevent mesial tipping of the molars and to stabilize the appliance, lower labial bow to stabilize the appliance, upper labial pads to remove the force of the upper lip and create periosteal pull to induce bone formation, and Tongue Crib to correct anterior tongue thrusting habit. Somchai Satravaha: AJODO 1999 www.indiandentalacademy.com
- 90. VT’s The construction bite is taken by retruding the lower jaw. www.indiandentalacademy.com
- 91. Post treatment Changes ANB angle as well as the Wits value remained quite stable. The SNA, SNB, SN-Pog, and NA-Pog became larger. The articular angle was increased The gonial angle exhibited a compensatory decline resulting in decreasing of the sum angle VT’s Long-term Results The Class III activator produced a more posterior position of the mandible and changed direction of the mandibular growth. Both alterations remained through the post activator period. The maxilla and the mandible grew with an increase in maxillo mandibular differential; the maxilla remained in a more forward position There was significant difference in the degree of change of angle OP/Go-Gn during the treatment but disappeared in www.indiandentalacademy.com the post activator period due to compensatory reduction of
- 93. VT’s The Two-Piece Corrector was designed by Gerald R. Eganhouse to apply biological forces that will counteract any Class III developmental vectors, whether skeletal or dentoalveolar, and correct or minimize their effects on the patient . It is a removable acrylic appliance that simultaneously applies an anterior force to the maxilla and an equal posterior force to the mandible. The flat, sliding surfaces of the two pieces create almost no friction as the dentition is disoccluded during movement, but provide both lateral and anteroposterior stability www.indiandentalacademy.com JCO 1997
- 94. Appliance construction: VT’s A construction bite of 4-6 mm thick is taken using an “Exacto Bite” registration jig. This gives an accurate centric relation, since the mandibular incisors can be positioned precisely. In the laboratory, a slide is created on the articulator, with the male (guide) portion in the maxillary acrylic plate and the female (groove) potion in the mandibular plate. The male portion is extended about 15 mm distal to allow for anteroposterior sliding and to ensure lateral stability as correction progresses. The anterior portion of the two pieces will flush when the appliance is inserted, but the maxillary piece will gradually slide forward on the mandibular piece Elastics provide the force between two parts of the appliance – one hook on each side of the maxillary plate on the disto buccal aspect of the maxillary first molar, two located in the maxillary first bicuspid – canine area, and the fourth placed between the mandibular canine and lateral incisor www.indiandentalacademy.com
- 96. The shorter elastics (1/8 ” 6oz ) are attached from the mandibular hook to the most anterior hook on the maxilla. As treatment progresses, it is moved to the posterior hook. The longer elastic on each side stretched from the mandibular hook to the molar hook can be (¼”, or 3/16” – 6oz) depending on the comfort. DURATION: 12 hours a day in conjugation with face mask. 11 months of treatment time and 18 -24 months of retention INDICATION: Mild skeletal class III where future surgery would not be indicated. And used during preadolescent and adolescent growth periods www.indiandentalacademy.com VT’s
- 97. VT’s CLASS III BIONATOR BALTERS BIONATOR III can be used in patients with skeletal Class III malocclusion. The use of this appliance causes some skeletal changes through neuromuscular modifications. Garatinni et al AJODO 1998 www.indiandentalacademy.com
- 98. VT’s • Upper lip pads • Lower labial bow • Protrusion bow in the upper arch www.indiandentalacademy.com
- 99. VT’s MODIFICATIONS • WITH UPPER LIP PADS • WITH REPELLING MAGNETS MODE OF ACTION www.indiandentalacademy.com
- 102. VT’s www.indiandentalacademy.com JCO 2005 & AO 2006
- 103. VT’s www.indiandentalacademy.com Liou et al JCO 2005
- 107. VT’s TREATMENT OF CLASS III MALOCCLUSIONS IN ADULT OR NONGROWING INDIVIDUALS www.indiandentalacademy.com
- 108. VT’s When a patient is diagnosed as a Class III malocclusion in the permanent dentition and if there is a strong skeletal component to the Class III malocclusion then treatment options are less. Such treatment usually includes comprehensive orthodontic therapy, either combined with extraction or orthognathic surgery. www.indiandentalacademy.com
- 109. The Orthognathic surgical procedure is designed to address the imbalance of the skeletal component (Eg: mandibular set back in patient with mandibular prognathism and Le-Fort I advancement in maxillary skeletal retrusion.) In patients who are expected to have excessive skeletal growth in the future, the surgical procedure is usually deferred until the end of active growth period. In the diagnosis and treatment planning of patients who present with a Class III malocclusion in the late deciduous or in the mixed dentition, several treatment options are available. www.indiandentalacademy.com VT’s
- 110. VT’s Inter-maxillary Class III elastics are most helpful in orthodontic (non-surgical) correction of Class III cases. They tend to produce lower incisor retroclination, upper incisor proclination, and A/P correction of the molar relationship. All components of the Class III elastic force can therefore be helpful in reaching treatment goals in average or low angle
- 111. Lower first premolar extractions are most favorable in assisting lower incisor distal movement, or Extraction of lower 2nd molars and Distalization of the 1st molar to achieve a class I molar relation (AO 2006) . If the lower arch is managed on a nonextraction basis, Class III mechanics can be used to produce some retraction and retroclination of the lower incisors. This can produce distal tipping of the lower premolars and molars, which in turn reduces the available space for the lower third molars . www.indiandentalacademy.com VT’s
- 112. Early removal of lower 3rd molars can be considered in some cases. A non-extraction approach to Class III treatment may not achieve sufficient lower incisor movement for the needs of the case. Correction of the malocclusion may be possible, but not over-correction. Thus, there is no provision in the result for any late growth changes, which occur relatively frequently in Class III cases, especially among male patients. VT’s www.indiandentalacademy.com
- 113. VT’s As with Class III treatment, it is important to recognize those Class III cases which have a major skeletal disproportion, either at the time of assessment, or where there is a probability of unfavorable growth. For such individuals, it will be necessary to consider a surgical / orthodontic solution. www.indiandentalacademy.com
- 114. Treatment on the basis of orthodontics alone should be delayed, or discarded as : This will involve proclination of upper incisors and retroclination of lower incisors. Good patient cooperation with Class III elastics and/or a face mask will normally be needed in this type of treatment. This should lead to an acceptable dental and facial outcome without the need for orthognathic surgery. www.indiandentalacademy.com VT’s
- 115. VT’s The incisors will need to be decompensated by orthodontics before surgery, if there is to be an optimal facial benefit from the surgery: REVERSE ORTHODONTICS The treatment of Class III malocclusions is relatively easy when the problem is confined to the alveolar bone, but when the deformity is in the basal bone such as in a deficient maxilla or overgrowth of the mandible, and then the malocclusion does not respond readily to treatment and tends to recur after treatment. www.indiandentalacademy.com
- 116. SITUATION A – A SURGICAL/ ORTHODONTIC CORRECTION TO AN IDEAL RESULT Determined that mandibular surgery will be required, then the surgeon will normally wait until all growth has finished, which may be as late as 22 years of age in males. The surgeon will then require the orthodontist to decompensate the incisors. Correction will be achieved by A/P realignment of the mandible and/or maxilla, with transverse correction of the maxilla if necessary. This should lead to an optimal facial and dental result. A 6-mm mandibular set-back will result in measurements to true vertical line (TVL) which are within 1 SD of the ideal. VT’s
- 117. SITUATION B – ORTHODONTIC MASKING OF A MILD CLASS III SKELETAL CASE. As an alternative to ‘A’ above, if the underlying skeletal discrepancy is mild, it may be decided to follow a treatment plan based on orthodontics alone. This will allow correction to be commenced much earlier, and the patient will be informed of the possibility of late mandibular growth. The orthodontist will then solve the problem by ‘masking’ the underlying Class III discrepancy by dental compensation- CAMOFLAGUE In this theoretical representation, the upper incisors were proclined 2° and the lowers were retroclined 8°. VT’s
- 118. SITUATION C – LATE MANDIBULAR GROWTH: After orthodontic masking of a mild Class III malocclusion, late mandibular growth can occur, especially in males. This is a difficult situation to manage! Sometimes the patient will find the late change in dental and facial outcome acceptable, and seek no further treatment. However, if mandibular surgery is deemed necessary, there is limited scope for facial improvement from the surgery, because of the dentally compensated teeth. In some cases, late mandibular growth occurs after the type of treatment shown in ‘B’ above. This is difficult to manage. VT’s
- 119. VT’s Early surgery is possible in maxillary deficient but surgical intervention in young child may further adversely affect the growth of maxilla. Patients with true mandibular prognathism may continue to grow for several years beyond the puberty so that two lateral cephalograms are taken at least 1 year apart demonstrate no significant growth occurring over that period. www.indiandentalacademy.com
- 120. VT’s The current surgical methods for correcting skeletal Class III problems include: Setting back prognathic mandible. Mandibular inferior border osteotomy to reduce chin height or prominence. LeFort I osteotomy to advance a deficient maxilla. www.indiandentalacademy.com
- 121. VT’s Skeletal discrepancies can not be resolved during mixed dentition by growth modification may require comprehensive appliance therapy or surgical correction. Some patients treated in early childhood may recur malocclusion during adolescence. Treatment in adolescence is indicated to alleviate the potential psychosocial problems and reduce the need for surgery. Malocclusion with mild mandibular prognathism www.indiandentalacademy.com and moderate overbite can be corrected by
- 122. Class III elastics with or without extraction of teeth are used to camouflaged the skeletal discrepancy, resulting in acceptable facial profile. As early as 1907 Edward Angle suggested that the only way to correct severe Class III malocclusion in adult was to combine surgery and orthodontic treatment. Before 1970s must thought that Class III malocclusion were primarily caused by excessive anteroposterior growth of the mandible and most were corrected by www.indiandentalacademy.com VT’s
- 123. However later studies indicated 20-25% of mandibular protrusion, but also around 75% of maxilla deficient cases also leads to Class III malocclusion so that clinician should analyse where the fault, whether in maxilla or mandible or combination. Maxillary growth may be completed at age 14 15 years were as mandibular growth may continue until early 20 years. After this surgical procedure can be carried out. www.indiandentalacademy.com VT’s
- 124. VT’s Chung, Kim, et al : AO 2006 www.indiandentalacademy.com
- 125. VT’s Eliminate anterior and posterior dental compensation with guideline from orthodontic visual treatment objectives (VTO). Establish appropriate anteroposterior and vertical incisor position. Achieve compatible arch forms and inter canine widths, which are essential to make dental midlines compatible at surgery. Correct tooth size discrepancy www.indiandentalacademy.com
- 126. Class III mechanics, molar tie backs are not used when leveling & teeth are allowed to level forward. The orthodontic VTO should be referred to confirm the extent of incisor decompensation required. On the completion of leveling, Class II elastics may be used to advance the mandibular buccal segment and further to procline the mandibular incisors. When decompensating the mandibular incisors, clinician should keep in mind, patient with mandibular antero posterior excess often have a very thin bony symphysis and a small area of attached gingiva in the incisor region www.indiandentalacademy.com VT’s
- 127. Bilateral sagittal split osteotomy (BSSO) is the procedure of choice, Although (TOVRO) trans-oral vertical ramus osteotomy may be indicated in large setback procedures. NOTE: Correct positioning of condyle is important. The surgeon should carefully free the medial pterygoid an a stylomandibular ligament from the medial side of the ramus. Otherwise proximal segment will be pushed back by distal segment & with return of muscle function, the patient will tend to position mandible forward again. www.indiandentalacademy.com VT’s
- 128. VT’s The incidence of neuro-sensory morbidity with trans-oral Vertical ramus osteotomy is less associated with bilateral sagittal split ramus osteotomy. A genioplasty is often indicated to place the chin in most esthetic antero posterior, vertical and midsagittal position. www.indiandentalacademy.com
- 129. VT’s The clinician should design the retention plan according to original malocclusion and its possible relapse tendency. If tendency to relapse is noticed, light (2.5 3.5 oz) Class III elastics should be placed immediately. A rectangular arch wire should be placed in maxilla to prevent the molar extrusion. www.indiandentalacademy.com
- 131. VT’s BSSO for Class III – 30% likelihood to relapse For isolated mand set back (1.49mm = 22.6%) the most important factor responsible for relapse is its magnitude. In bimax surgeries (set back = 5.44 mm & relapse = 3.33 mm – 61.2 %) : counterclockwise rotation of the proximal segment Rigid internal fixation did not guarantee more stability.(9.8 – 66%) Int’l J www.indiandentalacademy.com of adult ortho & orthga surgery: 2001
- 132. VT’s Maxillary anteroposterior deficiency often misdiagnosed as mandibular anteroposterior excess. So the clinician must carefully distinguish between the two deformities. www.indiandentalacademy.com
- 133. Cases of maxillary deficiency often involve crowding in the maxilla and retraction of incisor is indicated. This will require extractions. 1.If maximum retraction is necessary or significant crowding is present - extn of 1st premolar is indicated 2.If little retraction is necessary or crowding is slight – 2nd premolar is indicated. 3. Advancement of mandibular incisors from an upright or lingually tipped position may be limited by lack of attached gingiva or thin alveolar bone and symphysis. Extn of mandibular 2nd premolar is necessary to provide required space towww.indiandentalacademy.comcrowding. manage VT’s
- 134. Orthodontic Mechanics: Pre surgically:- the maxillary incisors should be placed in good angulation in the central trough of bone. To achieve best esthetic results. Surgical treatment:-The maxilla is advanced by means of Le-fort I Osteotomy. So surgeon can correct discrepancies in the Vertical, Transverse and Sagittal planes. www.indiandentalacademy.com VT’s
- 135. Undesirable soft tissue changes may occur, including widening of &/or tipping up of the nose and increased nasolabial angle. So that patient should be informed about expected soft tissue changes. Post surgical orthodontics: Surgical splint is given only in multipiece LeFort-I maxillary osteotomy or in bi-jaw surgery. Once the splint is removed immediately the orthodontist should place orthodontic palatal bar and continuous arch wire to maintain achieved results. www.indiandentalacademy.com VT’s
- 137. VT’s In as study done by Chen et al in 2007 compared the short and long term effects of bimaxillary surgery and mandibular setback on the narrowing of airway and concluded that bimaxillary surgery prevent narrowing of the airway space, which may lead to obstructive sleep apnea. AJODO 2007 www.indiandentalacademy.com
- 141. VT’s Tooth borne anchorage devices like TPA and Expansion Screws may lead to Dentoalveolar compensatory changes like lose of arch length, forward movement of molars, proclination of max. incisors, etc. Solution: Hydroxylapatite coated Osseointegrated palatal onplant www.indiandentalacademy.com
- 142. VT’s Class III malocclusion worsens with the continuing mandibular growth. Relapse from continuing mandibular growth is likely to occur and such growth is extremely difficult to control. Applying a restraining force to the mandible using a chin cap is not effective in controlling growth in a class III patient. In mild class III problems a functional appliance or a positioner may be enough to maintain the occlusal relationship during post treatment growth. www.indiandentalacademy.com
- 143. Wilford et al in their literature review attributed few identifiable & unavoidable factors to relapse in class III individuals: Unstable presurgurgical orthodontics Condyle being forces posteriorly into the fossa Occlusal splints that open the bite and create an upward and forward rotation of the mandible on splint removal Failure to remove the bony interferences from proximal segment that do not allow the segments to fit passively Macroglosia Untreated active condylar hyperplasia. www.indiandentalacademy.com VT’s
- 144. VT’s To improve skeletal discrepancy and provide a more favorable environment for future growth. But this may prove detrimental for long term stability of the case. Early orthopedic treatment using face mask or chin cup therapy improve skeletal relations which in turn minimizes excessive dental decompensation. Early treatment provides more pleasing facial profile, thus improves psycho-social development of child. It eliminates Orthognathic surgery maximizing growth potential of maxilla may minimize the extent of surgical procedures in cases of severe Class III malocclusion. “Correct diagnosis and proper treatment planning holds the key to successful outcome of the case.” www.indiandentalacademy.com
- 145. VT’s Contemporary orthodontics: William R. Proffit Early orthodontic treatment: J Daniel Subtenly Orthodontics current principles and techniques: T.M Graber, Vanarsdal, Vig Biomechanics and esthetic strategies in Clinical Orthodontics: Ravindra Nanda Text of orthodontics: Samier Bishara Graber Petrovic Rakosi Seminar in orthodontics 2005 – EARLY TREATMENT AJODO 2006 Apr Suppl. Int’l J of adult ortho & orthga surgery: 2001 Ngan P et al: AJODO : 1996 Ngan P et al: Pediat Dent : 1997 AJO DO 2005 128; 299-309 Kalha A S: EBD 2006:7,16-17 JCO 1997 – 2 PIECE CORRECTOR FOR CLASS III Garatinni et al AJODO 1998 J Ind. Ped & Prev Dent: 1998 – Uteraja et al East Mediters Health J: 2006: www.indiandentalacademy.com Danaie et al
- 146. VT’s www.indiandentalacademy.com Leader in continuing dental education www.indiandentalacademy.com