
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Similar a introduction to Psycopharmacology
Similar a introduction to Psycopharmacology (20)
Más de ismail sadek
Más de ismail sadek (18)
Último
Último (20)
introduction to Psycopharmacology
- 2. + Preview Principles of Psychopharmacology Pharmacokinetics Pharmacodynamics Sites of Drug Action
- 3. + Introduction Psychopharmacology The study of the effects of drugs on the nervous system and behavior Drug effects – the changes a drug produces in an animal’s physiological processes and behavior Sites of action – the locations at which molecules of drug interact with molecules located on or in cells of the body, thus affecting some biochemical processes of
- 4. + Principles of Psychopharmacology Pharmacokinetics The process by which drugs are: absorbed, distributed within the body, metabolized, and excreted.
- 5. + Principles of Psychopharmacology Routes of Administration Oral Administration – administration of a substance into the mouth so that it is swallowed. Sublingual Administration – administration of a substance by placing it beneath the tongue.
- 6. +Routes of Drug Administration Oral Drug Administration Advantages: relatively safe, economical, convenient, practical Disadvantages: Blood levels are difficult to predict due to multiple factors that limit absorption. Some drugs are destroyed by stomach acids. Some drugs irritate the GI system.
- 7. + Principles of Psychopharmacology Routes of Administration Intravenous (IV) Injection – injection of a substance directly into a vein. Drug enters bloodstream immediately and reaches the brain in seconds
- 8. + Principles of Psychopharmacology Routes of Administration Intraperitoneal (IP) Injection – injection of a substance into the peritoneal cavity, the space that surrounds the stomach, intestines, liver, and other abdominal organs. Most common route for small laboratory animals
- 9. + Principles of Psychopharmacology Routes of Administration Intramuscular (IM) Injection – injection of a substance into a muscle.
- 10. + Principles of Psychopharmacology Routes of Administration Subcutaneous (SC) Injection – injection of a substance into the space beneath the skin.
- 11. + Principles of Psychopharmacology Routes of Administration Intrarectal Administration – administration of a substance into the rectum. Inhalation – administration of a vaporous substance into the lungs. Topical Administration – administration of a substance directly onto the skin or mucous membrane. Insufflation – sniffing drugs; contacts mucous membranes of the nasal
- 12. + Principles of Psychopharmacology Routes of Administration Intracerebral Administration – administration of a substance directly into the brain. Intracerebroventricular (ICV) Administration – administration of a substance into one of the cerebral ventricles.
- 13. + Routes of Drug AdministrationAdvantages of Injection Routes Absorption is more rapid than with oral administration. Rate of absorption depends on blood flow to particular tissue site (I.P. > I.M. > S.C.). Advantages specific to I.V. injection No absorption involved (inject directly into
- 14. + Routes of Drug Administration Disadvantages/Risks of Injection A rapid onset of action can be dangerous in overdosing occurs. If administered too fast, heart and respiratory function could collapse. Drugs insoluble in water or dissolved in oily liquids can not be given I.V. Sterile techniques are necessary to avoid the risk of infection.
- 15. + Principles of Psychopharmacology Distribution of Drugs Within the Body Lipid Solubility – ease with drug molecules are soluble in fat. Heroin more lipid soluble than morphine so gets to brain faster; more intense ”rush” Depot Binding – binding of a drug with various tissues of the body or with proteins in the blood. If drug bound to depot cannot reach site of action Albumin – a protein found in the blood; serves to transport free fatty acids and can bind with
- 16. + Depot Binding with Blood Albumin Protein
- 17. +Drug Distribution Cell Membranes Capillaries Drug affinities for plasma proteins Bound molecules can’t cross capillary walls Blood Brain Barrier Tight junctions in capillaries Less developed in infants Weaker in certain areas, e.g. area postrema in brain stem Cerebral trauma can decrease integrity Placenta Not a barrier to lipid soluble substances.
- 18. +Termination of Drug Action Biotransformation (metabolism) Liver microsomal enzymes in hepatocytes transform drug molecules into less lipid soluble by-products. Cytochrome P450 enzyme family
- 19. + Termination of Drug Action Elimination Two-stage kidney process (filter, absorption) Metabolites that are poorly reabsorbed by kidney are excreted in urine. Some drugs have active (lipid soluble) metabolites that are reabsorbed into circulation (e.g., pro-drugs) Other routes of elimination: lungs, bile, skin
- 20. + Termination of Drug Action Kidney Actions excretes products of body metabolism closely regulates body fluids and electrolytes The human adult kidney filters approx. 1 liter of plasma per minute, 99.9% of fluid is reabsorbed. Lipid soluble drugs are reabsorbed with the water.
- 21. + Termination of Drug Action Factors Influencing Biotransformation Genetic Environmental (e.g., diet, nutrition) Physiological differences (e.g., age, gender differences in microsomal enzyme systems) Drug Interactions Some drugs increase or decrease enzyme activity e.g., carbamazepine stimulates CYP-
- 23. + Pharmacodynamics Drug actions at receptor sites and the physiological/chemical/behavioral effects produced by these actions: Studies of drug mechanisms of action at the molecular level Provides basis for rational therapeutic uses and the design of new, superior therapeutic agents
- 24. + Definitions Efficacy Degree to which a drug is able to produce the desired response Potency Amount of drug required to produce 50% of the maximal response the drug is capable of inducing Used to compare compounds within classes of drugs
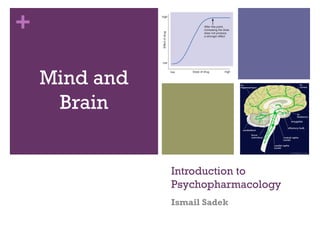
- 25. + Principles of Psychopharmacology Dose-Response Curve – a graph of the magnitude of an effect of a drug as a function of the amount of drug administered. Usually defined as mg of drug/Kg of body weight
- 26. + Definitions Effective dose 50% (ED50) Dose of the drug which induces a specified clinical effect in 50% of subjects Toxic Dose 50% (TD50) Dose of the drug which induces toxic effect in 50% of subjects
- 27. +Dose-Response Curves for Morphine
- 28. + Principles of Psychopharmacology Therapeutic Index – the ratio between the dose that produces the desired effect in 50% of the animals and the dose that produces toxic effects in 50% of the animals. If toxic dose is 5 times higher than the effective dose then the TI = 5 The lower the TI, the more care must be taken in prescribing the drug
- 29. + Principles of Psychopharmacology Effects of Repeated Administration Tolerance – a decrease in the effectiveness of a drug that is administered repeatedly. Withdrawal Symptom – the appearance of symptoms opposite to those produced by a drug when the drug is administered repeatedly and then suddenly no longer taken. Sensitization – an increase in the effectiveness of a drug that is administered repeatedly.
- 30. + Sites of Drug Action Most drugs that affect mental functions affect synaptic transmission
- 32. +Review of steps in synaptic transmission Neurotransmitters are synthesized and stored in synaptic vesicles Vesicles travel to presynaptic membrane and dock Axon fires and voltage-dependent calcium channels open allowing calcium ions to enter Calcium ions interact with docking proteins causing release of neurotransmitter into synaptic cleft Neurotransmitter binds to postsynaptic receptor, ion channels open, PSPs produced Effects of neurotransmitter kept brief by reuptake or enzymatic degradation
- 33. +Drug Affects on Synaptic Transmission
- 34. + Sites of Drug Action Act on Neurotransmitters Enzymes control the synthesis of a neurotransmitter from its precursors. Rate of synthesis and release can be increased by administering the precursor The precursor serves as an agonist (step 1 in Figure 4.5) If a drug inactivates the enzymes it prevents the neurotransmitter from being produced It serves as an antagonist (step 2 in Figure 4.5)
- 35. + Drug Affects on Synaptic Transmission
- 36. + Sites of Drug Action Effects on Storage and Release of Neurotransmitters Drugs may exert their agonistic or antagonistic effects by influencing the storage and release of neurotransmitters. Some drugs can prevent the storage of neurotransmitter in the vesicles – antagonists (step 3 in Figure 4.5) Some drugs can also prevent the release of neurotransmitters by deactivating proteins that cause synaptic vesicles to fuse with presynaptic membrane (step 5 in Figure 4.5) Other drugs act as agonists by triggering the release of neurotransmitter (step 4)
- 37. + Drug Affects on Synaptic Transmission
- 38. + Sites of Drug Action Effects on Receptors Drugs may exert their agonistic or antagonistic effects by influencing receptors. Direct Agonist – a drug that binds with and activates a receptor; mimics the effects of a neurotransmitter (step 6 in Figure 4.5). Direct Antagonist – a drug that binds with a receptor but does not activate it; prevents the natural ligand from binding with the receptor; also called receptor blocker (step 7 in Figure 4.5).
- 39. + Drug Affects on Synaptic Transmission
- 40. + Sites of Drug Action Noncompetitive Binding – binding of a drug to a site on a receptor; does not interfere with the binding site for the principal ligand. Indirect Antagonist – a drug that attaches to a binding site on a receptor and interferes with the action of the receptor; does not interfere with the binding site for the principal ligand. Indirect Agonist – a drug that attaches to a binding site on a receptor and facilitates the action of the receptor; does not interfere with the binding site for the principal ligand.
- 41. + Drug Actions at Binding Sites
- 42. + Sites of Drug Action Autoreceptors – regulate the amount of neurotransmitter released Drugs that activate these receptors serve as antagonists, decreasing the amount of neurotransmitter released (step 8 in Figure 4.5) Drugs that block the presynaptic autoreceptors increase the release of neurotransmitter (step 9 in Figure 4.5)
- 44. + Drug Affects on Synaptic Transmission
- 45. + Sites of Drug Action Some terminal buttons form axoaxonic synpases Presynaptic Heteroreceptor – a receptor located in the membrane of a terminal button that receives input from another terminal button by means of an axoaxonic synapse; binds with the neurotransmitter released by the presynaptic terminal button.
- 47. + Sites of Drug Action Effects on Reuptake or Destruction of Neurotransmitters Drugs can attach to transporter molecules responsible for reuptake and inactivate them Drugs can bind with the enzyme that normally destroys the neurotransmitter and prevent it from working Both types of drugs prolong the presence the neurotransmitter in the synaptic cleft – agonists (steps 10 and 11 in Figure 4.5).
- 48. + Drug Affects on Synaptic Transmission
- 49. + 49 Receptors Receptors are a target molecule that a drug molecule has to combine with to produce a specific effect Receptors must be compatible.
- 50. + Actions at Receptors Agonist: binds to receptors and produces pharmacological action. Antagonist: binds to receptors but produces no pharmacological action Partial agonists It is possible to produce signal transduction that is something more than an antagonist yet something less than a full agonist. Inverse agonists Inverse agonists are more than simple antagonists.These agents have an action that is thought to produce a conformational change in the G-protein linked receptor that stabilizes it in a totally inactive form. Binding or localization in the Brain
- 51. + Agonist and antagonist interactions with receptors
- 52. + A drug binds to a receptor…Then what? Intracellular action: promotes synthesis or release of an intracellular regulatory molecule - second messenger.
- 53. + Cell Nucleus
- 54. + A complex cascade of changes amplify the effects of the receptor within the neuron.
- 55. + 55 Types of receptors G-protein-couple receptors, seconds e.g. Muscarinic ACh receptors, adrenoceptors, histamine receptors Kinase linked receptors, hours e.g. Insulin, Growth factor Nuclear intracellullar receptors, hours e.g. steroid, thyroid hormone
- 56. + 56 Ion Channels Drugs act to affect cellular gating mechanism in cell wall Ligand-gated ion channels, milliseconds e.g GABA benzodiazepines, Nicotinic ACh Carrier molecules Drugs act on carrier transporters which allow molecules, not lipid soluble to cross cell membrane
- 57. + General Pharmacology strategies Indication: Establish a diagnosis and identify the target symptoms that will be used to monitor therapy response. Choice of agent and dosage: Select an agent with an acceptable side effect profile and use the lowest effective dose. Remember the delayed response for many psych meds and drug-drug interactions.
- 58. + Establish informed consent:The patient should understand the benefits and risks of the medication. Make sure to document this discussion including pt understanding and agreement. In fertile women make sure to document teratogenicity discussion. Implement a monitoring program:Track and document compliance, side effects, target symptom response, blood levels and blood tests as appropriate.
- 59. + Management: Adjust dosage for optimum benefit, safety and compliance. Use adjunctive and combination therapies if needed however always strive for the simplest regimen. Keep your therapeutic endpoint in mind.
Notas del editor
- Drugs are exogenous chemicals Drugs have effects and sites of action
- Oral – humans medicine; not good one for many animals
- Different routes of admin determine the rate drug enters the bloodstream
- Rapid but not as fast as IV
- Injection made into large muscle, upper arm, thigh or buttocks
- Useful for small amounts because large volume would be painful
- Intrarectal – rarely used in animals; used with drugs that can cause stomach upset
- Cover in chapter 5
- Drugs exert their effects only when they reach their sites of action...which for us is the CNS Different routes of admin determine the rate drug enters the bloodstream (except intracerebral and ICV)…but what happens next? Several factors determine rate drug in bloodstream reaches the brain. BBB only barrier for water soluble drugs.
- Depot binding can delay and prolong drug effects Take lipid-soluble drug orally…absorbed from stomach into bloodstream where it binds to albumin…little gets to the brain until albumin molecules can hold no more. Then gradually the albumin molecules release the drug as plasma levels of drug fall.
- The best way to measure drug effectiveness is to plot a dose-response curve
- Opiates such as morphine produce analgesia (reduced sensitivity to pain) but also depress activity of neurons in the medulla that control heart rate and respiration. Physician would want to administer a dose effective for pain relief but not cause respiratory failure. Most desirable drugs have large margin of safety.
- One measure of a drug’s margin of safety is its TI.
- When drugs are repeatedly administered the effects don’t remain constant Tolerance and withdrawal caused by body’s compensatory response to drug…restore equilibrium/balance/homeostasis
- Drugs can affect any one of these steps
- Transporter molecules in the membrane of the vesicle…similar to transporter molecules responsible for re-uptake
- Probably the most important, and certainly the most complex, site of drug action is on receptors (both presynaptic and postsynaptic).
- Some receptors have multiple binding sites
- Autoreceptors on dendrites of some neurons When neurons become active the dendrites, as well as terminal buttons, release NTS. When autoreceptors are stimulated they decrease firing by producing hyperpolarizations. This serves to prevent neurons from becoming too active.
- The last step in synaptic transmission is termination of the PSP…accomplished by re-uptake of NTS or degradation by enzymes..drugs can interfere with either of these two processes
- mq-fig-01-11-0.jpg
- G protein receptors work in seconds Kinase (enzyme) linked receptors can take hours.
- Some ion channels are gated by receptor (open only when receptor is occupied by an agonist) while other are voltage-gated-drugas affect the permage or flow of for example, potassioum, sodium or calcium in and out of the cell Drugs acting at ion channels include Benzodiazpeines that act at GABA (gamma amino butyric acid receptor) chloride channel return over excitable receptor to constitutive (normal) level of activation Calcium channel blockers prevent diffusion of calcium through cell membrane Nicorandil acts at potassium channels Carrier molecules allow transport of small organic molecules that are too polar-not sufficiently lipid soluble to penetrate cell membranes on their own. Eg. Glucose and amino acids Examples of drugs that act in this way include Loop diuretics which inhibit sodium, potassium and chlorine passage in the lop of Henle Another example Omeprazole inhibits proton pump in the gastric mucosa Tricyclics inhibit noradrenaline uptake