Goals of patient care introduction
•Descargar como PPTX, PDF•
3 recomendaciones•1,643 vistas

Goals of patient care

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Goals of patient care introduction
Similar a Goals of patient care introduction (20)
Más de SCGH ED CME
Más de SCGH ED CME (20)
Último
Último (20)
Goals of patient care introduction
- 1. Goals of Patient Care “It’s everyone’s responsibility”
- 2. Outline • Brief background about Goals of patient care (GOPC) • Some tools • Patient identification • Communication • The new form structure • Timelines • Resources
- 3. Background • The GOPC form is still in it’s trial state •14 sites across WA now using the GOPC trial form instead of a Not For Resuscitation Form (blue form) • Previous pilot of the trial form in 2017 • Wards G53, G63, C17 (SCGH) • Ward 4 (OPH)
- 4. Current situation 2/3rd of MET calls are after hours – Where difficult decisions are made quickly by clinicians who do not know the patient & without patient / surrogate decision maker input. Of MET calls are repeatMET calls
- 5. Synergies •Fits in with Choosing Wisely initiatives •Part of Sustainable Health care is providing appropriate the goal of care to patients •Links in with advanced health care directives
- 6. Considerations • Estimated 70% of patient deaths are now expected. • In WA, an average of 8 admissions in last year of life • Over half of all deaths occur in hospital • Many decisions to limit treatment occur in crisis situations, especially during MET calls
- 7. Pathways to death -- Multiple co- morbidities, each hosp adm leads to poorer new baseline -- Frail – not expected to survive even single organ failure MOST ADMITTED PATIENTS AND THOSE SEEN FREQUENTLY IN OUTPATEINTS FALL INTO THE ABOVE CATEGORIES!
- 8. GOPC rationale • A medical decision making based on determining the patient’s goals of care. • Assigned according to realistic assessment of probable outcomes •Not the same as Advance Health Directive – which is made by the person in their own voice and utilised when capacity is lost •Conversation is shared with the patient or their surrogate decision maker
- 9. GOPC – patient identification tools Does your patient have two or more of the following? 1. Reducing function 2. Two or more hospital admissions in 6 months 3. Weight loss of 5-10% 4. Refractory symptoms 5. Dependent on others for care needs
- 10. The surprise question Would you be surprised if this person died in the next 6 – 12 months?
- 11. The SPICT Tool 2 part tool: 6 General indicators Patient requires 2 or more indicators from this section
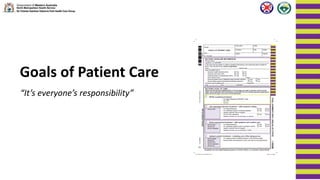
- 13. Change in forms 4 main sections (1)Baseline information (2)Goal of care - All life sustaining tx - Life extending tx - Active ward based mx - Comfort care (3)Goal of care summary discussion (4)Extended use of form
- 14. Section 1 – intern & above
- 15. Section 2 – Registrar or Consultant LHS – what is NOT being done RHS – tailoring what IS to be done
- 16. All life sustaining treatment • Aim is cure • Is there reasonable chance the patient will leave hospital with a similar life span? • Probably the quickest discussion / decision. • No limitations on interventions / treatments FOR CPR MET calls ICU
- 17. Life extending treatment • With probable treatment ceiling • Aim is for prolonged disease remission or restoration of pre episode health status. • Returning to previous level of function • For life sustaining treatments as needed. • May require ICU review / consult Not for CPR
- 18. Active Ward based care Consider in patients who may have: • Incurable and progressive disease • Advancing disease: anticipating death • Life expectancy months, possibly years Remember the “surprise question” • Aim of treatment: • Length of survival not sole determinant • Comfort, quality and dignity • Treatment underlying disease still appropriate Not for CPR Symptom / comfort care
- 19. Optimal comfort treatment •Including care of the dying person •Death imminent •Would you be surprised if they died during this admission. •Should be on Care Plan for the Dying Person Aim is comfort, quality of life and dignity
- 20. NOTE! To make the form valid P.T.O None of what’s been completed in section 2 is valid unless section 3 is signed overleaf.
- 21. Section 3 = Most crucial section The Goal of patient care summary of discussion Area to be signed to make the form valid
- 22. Section 4 = Extended use of form This section can be completed in outpatients and valid if the patient is then subsequently admitted to hospital for example If signed, then the form is valid for 12 months* * Team are working with HIMS on how a valid form can be pulled from the medical record in to the medical notes
- 23. GOPC narrative • It’s all about communication • It’s also a clinical decision tool • Understand what’s important to the patient • Understand what lifestyle limitations / treatments would be unacceptable to them
- 24. • Do you want us to do everything? • Resuscitation is futile • The medical team have decided •There is nothing more we can do Importance of use of languageWe might say
- 25. • Do you want us to do everything? • Resuscitation is futile • The medical team have decided •There is nothing more we can do What the patient/family hears…. • Do you want us to try? • Your loved one is worthless •We don’t care what you think… we’ll decide for you •We are going to abandon treatment and care
- 26. • Do you want us to do everything? • Resuscitation is futile • The medical team have decided •There is nothing more we can do Reframing the discussion • Do you want us to try? • Your loved one is worthless •We don’t care what you think… we’ll decide for you •We are going to abandon treatment and care • We want to work out what is the right thing to do…. •Treatment that is ineffective and distressing •The treatment is not working • We will do everything possible to ensure comfort and dignity…
- 27. GOPC narrative 2 x videos
- 28. Video 1 = NFR CPR decision – first step Done just before death Emphasis is on what “won’t be done” Sub-optimal care Misses patient preferences Treating team perform Emphases what “will be done” Consensus care Seeks patients preferences Breaks the ICE Video2 = “Goals of care”
- 29. Ask Tell Ask Framework • Ask For opinions and thoughts – open questions / Fears • Tell “To make sure we are on the same page, can you tell me what is your understanding of your illness?” • Ask Can we talk about what we should do if things don’t go as well as we hope? • If your illness gets worse, what things would be most important to you? • Who are you going to tell about this conversation?
- 31. On change over day Patients who have a current “blue” form will require the details of the form updated on to the GOPC form and the “blue” form to be cancelled.
- 32. Next steps • Feedback from all areas of use will shape how the final from will look like • We will be formalising dates for focus groups in due course
- 33. Overall aim • One form across the whole of WA • Linked form with the community
- 34. GOPC resources • GOPC.SCGH@Health.Wa.Gov.Au SCGH: • Annie Brinkworth – MET Co-Ordinator • Anil Tandon – Palliative Care Physician OPH • Brendan Foo – Rehab and Aged Care https://ww2.health.wa.gov.au/Articles/F_I/Goals-of- patient-care http://www.spict.org.uk/using-spict/
- 35. Any Questions?
- 36. Take home messages •Consider for all admitted patients •End of life = last 12 months •You are NOT saving time by avoiding these conversations but may be increasing suffering. •Communication is key! •Make a home team decision