APM Welcome, APM North West Network Conference, Synergies Across Sectors
Blood Administration
1. Blood Administration
Reference: http://rnbob.tripod.com/blood.htm
1. Only two units per filter.
2. Verify units.
3. Use within four hours after removal from blood bank.
4. Use 20 ga. or larger catheter.
5. Obtain Informed consent.
6. PRBC replaces RBCs only.
7. If more than 6-8 units of PRBC are given then give FFP with every other unit.
8. Give platelets one for every unit of PRBC after eight units.
ESSENTIAL INFORMATION:
1. Clinical Pathology and Transfusion Medicine Guide
2. Nursing Department Policy: Infusion of Blood and Blood Components.
3. Department of Transfusion Medicine (DTM) Procedure: Infusion of Non-cryopreserved Cellular
Components.
4. Circular of Information For the Use of Human Blood and Blood Components, American Association of
Blood Banks. July 1998 (Distributed by DTM)
EQUIPMENT:
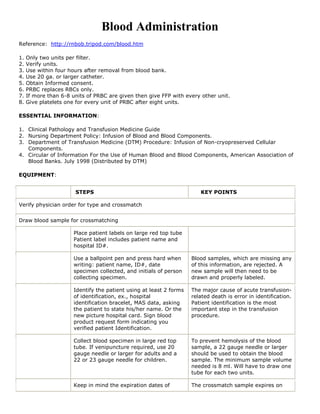
STEPS KEY POINTS
Verify physician order for type and crossmatch
Draw blood sample for crossmatching
Place patient labels on large red top tube
Patient label includes patient name and
hospital ID#.
Use a ballpoint pen and press hard when Blood samples, which are missing any
writing: patient name, ID#, date of this information, are rejected. A
specimen collected, and initials of person new sample will then need to be
collecting specimen. drawn and properly labeled.
Identify the patient using at least 2 forms The major cause of acute transfusion-
of identification, ex., hospital related death is error in identification.
identification bracelet, MAS data, asking Patient identification is the most
the patient to state his/her name. Or the important step in the transfusion
new picture hospital card. Sign blood procedure.
product request form indicating you
verified patient Identification.
Collect blood specimen in large red top To prevent hemolysis of the blood
tube. If venipuncture required, use 20 sample, a 22 gauge needle or larger
gauge needle or larger for adults and a should be used to obtain the blood
22 or 23 gauge needle for children. sample. The minimum sample volume
needed is 8 ml. Will have to draw one
tube for each two units.
Keep in mind the expiration dates of The crossmatch sample expires on
2. crosmatches for most hospitals. 11:59 p.m. on the third day after the
day it is drawn, i.e. a sample drawn
anytime Tuesday the 23rd, will expire
at 11:59 p.m. on Friday the 26th.
Blood Transfusion Preparation – Verify Order for Blood Product, Identification & Consent
Check physician’s order to determine: Allow 30 – 60 minutes for oral
a. product to be administered medications, 10 minutes for IV
b. number of units or volume to be medications to become effective.
administered
c. date to be administered
d. special processing
e. duration of infusion
f. pre-medication orders, if indicated
For whole blood, red blood cells or
granulocytes, verify in the computer or
with the blood bank.results of:
a. blood grouping
b. Rh type
c. number of units crossmatched
d. number of units set up
Verify informed consent has been Consent required for ALL blood
obtained and signed in the past year, products.
except for emergency transfusions.
Ensure the inpatient is wearing hospital Required for ALL blood products.
ID bracelet. Ask lucid patients to state full
name and date of birth. If not lucid, ask
responsible visitor.
Establish Line & Check Client’s VS
Establish or verify patency of peripheral When infusion pump is used, 20
or central venous access device. gauge needle or larger is
recommended to prevent lysis of red
blood cells. 23-gauge needle can be
used for transfusing pediatric
patients.
Obtain and record patient’s baseline Febrile patients destroy cells
vital signs. Conduct patient teaching and rapidly. If febrile, notify physician to
alert staff to the following symptoms: decide if transfusion can wait or if
• Chest pain. patient should receive acetaminophen
• Flushing. as a pre- medication.
• Shivering.
• Abdominal discomfort.
• Rashes.
• Shortness of breath.
• Pain in the loins or extremities.
• Blood in urine.
• A feeling of restlessness or anxiety.
• Feeling generally unwell
Pick up Blood from Blood Bank
3. When the patient is ready to be There should be a four hour time
transfused, take pick up slip to blood lapse between completing infusion of
bank to obtain blood. Amphotericin and beginning
transfusion of granulocytes or vice
versa. It is advisable that all other
blood products be separated from
Amphotericin by two hours. Blood
products must be hung within 30
minutes of leaving the Blood Bank
refrigerator. The Blood Bank will
usually only release one blood
product at a time. However, with
physician phone call multiple units
may be issued during an emergency.
Blood products MUST NEVER be
placed in the refrigerator on the
patient care unit.
Check the appearance of unit for If appearance is suspicious, return it
presence of clots, brown discoloration, to Blood Bank, as it may not be
clumps or abnormal cloudiness, and appropriate for infusion.
integrity of seals.
Warming is not normally necessary
and blood components should never
be put in a bowl of warm water, on a
radiator or in a microwave oven: this
is dangerous, as it will damage the
cells.
Two qualified health professionals trained All three records must correspond
in blood administration procedures exactly.
compare: All identification attached to the
a. Blood product received on the unit container must remain attached until
to product requested in the the transfusion has been terminated.
medical order.
b. Blood type and Rh type recorded
in computer with the container
bag and container label ensuring
that they are either identical or
compatible.
c. The blood product number on the
blood container with the product
number on the blood container
tag.
d. Compare the expiration date and
time, if present, on the blood
container label to the current date
and time.
Immediately before the transfusion, The major cause of acute transfusion-
in the presence of the recipient, two related death is error in identification.
qualified health professionals identify the Proper patient and unit identification
patient using at least 2 forms of is one of the most important steps in
identification: the transfusion process. If any
a. Verify the patient’s name and discrepancy is noted, notify Blood
medical record number on the Bank at once and return the blood
blood unit with the information on product until the discrepancy is
4. the recipient’s identification resolved.
bracelet and the information
recorded in the patient record. Identify patients with patient hospital
b. Ask the patient to state his/her ID band or hospital label and ask the
name. patient to state their name. Correlate
c. Verify the information on the this information with blood
patient wristband and blood unit. component’s tag.
Start the Infusion Set
Prime the administration set with the Use of other IV solutions damages
blood product or 0.9% Sodium Chloride. blood components.
a. Add a three-way stopcock onto the During a reaction, 0.9% Sodium
end of the blood administration Chloride may be administered
set. Have 0.9% Sodium Chloride through the stopcock without infusing
solution and IV tubing unopened the additional blood product in the
and available in room for tubing
emergency use or attached to Leukocyte depletion filter may be
stopcock. used to prevent repeat febrile
b. If a leukocyte-depletion filter is reactions, decrease the risk of CMV
indicated, follow the transmission, and decrease the risk
manufacturer’s and blood Bank of alloimmunization. Do not flush
instructions for set up. filter with saline. Leukocyte
depletion filters are not to be
used when administering
granulocytes.
Connect the blood administration set to During a blood transfusion, it is
the IV extension set either directly or recommended that no intravenous
through the intermittent infusion cap via drugs are added to the same cannula
needleless system. or giving set, because of the risk of
interactions
Adjust the rate of flow for first few .
minutes A volumetric infusion pump may be
For adults: used to administer blood products.
• Platelets or plasma - 2-5 Symptoms of an immediate adverse
cc/min for 5 minutes reaction are usually manifested
• Whole blood, RBC or during infusion of the initial 50 cc. If
granulocytes - 2cc/min for 15 an incompatible transfusion is
minutes terminated early, acute renal necrosis
Patient should be observed closely for the and death may be prevented.
first 15 minutes.
For pediatric patients, volume of
For pediatric patients: blood products (excluding
• transfuse 5% of the total volume granulocytes) to be transfused should
ordered in the first five minutes be ordered based on the child’s
of platelet or plasma infusion weight, i.e. 10 - 15 ml/kg.
• first 15 minutes of whole blood,
RBC’s or granulocyte infusion.
Remain with the patient for the first 15
minutes after the start of the infusion.
Monitoring for Adverse Reaction
At the end of the first 15 minutes, The desirable rate of infusion
5. obtain and record TPR and BP. If vital depends upon patient’s blood volume,
signs are within normal range and the cardiac status, and hemodynamic
patient has no signs/symptoms of an condition. Suggested rates for adults
adverse reaction, change the rate to are:
infuse the unit within the time period PRBCs: 100-230 cc/hr
specified in the physician’s order. Granulocytes: 75-100 cc/hr
Plasma/platelets: 200 – 300 cc/hr
The volume of a plateletpheresis bag
varies from 120 cc to 400 cc. The
entire platelet product should be
given within one hour, if possible.
Continue to monitor the patient for signs .
and symptoms of adverse reaction during Adverse transfusion reactions can
transfusion and 1 hour post- transfusion. occur anytime during or after the
If patient experiences a transfusion transfusion.
reaction while transfusion is in progress, For treatment of adverse transfusion
immediately stop the transfusion. reactions: see Clinical Pathology and
Maintain patency of line with normal Transfusion Medicine Guide quot;Adverse
saline and notify MD. Reactions to Transfusionsquot;.
Complete transfusion as ordered not to Increased possibility of contamination
exceed four hours. and decreased viability of cells if
prolonged.
Tubing sets can be used for second
unit of blood if used within four hours. As there is a possibility of delayed
transfusion reactions, some hospitals
require empty transfusion packs to be
kept to enable testing if required.
Packs should only be stored for the
required time as they are a source of
infection in themselves if left for
extended periods.
At the conclusion of a blood product Do not flush leukocyte filters with
transfusion in which no adverse reaction saline.
occurred:
a. Obtain 10 - 60 minute post
transfusion CBC for post-count as
indicated.
b. Flush the blood administration set
with 0.9% Sodium Chloride until
the tubing is clear.
c. Obtain and record vital signs.
d. Disconnect and discard the empty
blood product container in a
contamination red bag.
Adverse Reactions
Pyrexia A temperature of more than 38 C might be due to:
• n Pyrogens resulting from bacterial contamination.
• n Reaction to white cells or platelets which can
• also be accompanied by chills or rigors.
• n Haemolytic blood reaction (see below).
The appropriate action is to stop the transfusion and to seek medical advice.
6. Allergic reaction Allergic reactions can present as an urticarial rash or a mild pyrexia. This can also
develop into oedema around the eyes or larynx and cause dyspnoea. Full anaphylaxis is uncommon. The
appropriate action is to stop the
transfusion and to seek medical advice. (Subsequent transfusions might require pre-medication with a
prescription for an antihistamine and paracetamol.)
Infection Although donated blood is screened for major viruses and bacteria (including HIV, hepatitis B,
hepatitis C and syphilis), infections, although very rare, do occasionally occur. Much more common,
however, is local phlebitis which
occurs if a cannula remains in situ for too long: the most commonly isolated bacteria are staphylococci
or corynebacteria. Platelets are stored at room temperature and so can act as an ideal medium for
bacterial growth. The appropriate action is to check cannula insertion sites regularly for inflammation and
infection, and to change the insertion site routinely every 72 hours. When using platelets, bags should be
checked for discolouration, which may indicate the presence of bacteria.
Haemolytic reaction A haemolytic reaction is caused by destruction of the donor red blood cells by
antibodies in the recipient’s plasma. It can occur after only a few millilitres of blood are transfused,
although a delayed reaction can occur up to two hours later. Haemolytic reactions can be fatal and as
such, a suspected haemolytic reaction must always be responded to as a medical emergency. A
haemolytic reaction is indicated by:
• Breathlessness.
• Collapse.
• Tachycardia.
• Hypertension followed by hypotension.
• Chest or loin pain.
• Subsequently, the patient might develop:
• Disseminated intravascular coagulation (DIC).
• Circulatory and respiratory failure.
• Renal failure.
The appropriate actions are:
1. stop the transfusion
2. disconnect the pack and giving set
3. maintain the intravenous line with normal saline
4. seek urgent medical advice.
This is an emergency, life-threatening situation. Haemolytic reaction is most likely to be due to a patient
receiving the wrong blood from one or more errors in the chain of events from taking a cross-match
sample, the laboratory processes, the collection of blood for transfusion and administration into the
recipient. All blood must be returned to the blood bank and an investigation must be carried out to
ascertain the source(s) of the error.
Circulatory overload Circulatory overload causes less of a problem now that concentrated red cells are
used more frequently than whole blood. Problems can occur with older people, neonates or patients with
megaloblastic anaemia.
The action to take is to give diuretic therapy as prescribed, slow the rate of transfusion and observe
closely for pulmonary and peripheral oedema.
Iron overload Patients who receive multiple transfusions have an increased serum ferritin. At a level
greater than 1,000mg per litre, the iron infiltrates organs such as the liver, heart and kidneys, which can
lead to organ failure or even
be fatal. In patients on multiple transfusion programmes, an iron chelater such as desferrioxamine can be
prescribed to regulate the level of serum ferritin.