
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Similar a Breast Atypical Lesions
Similar a Breast Atypical Lesions (20)
Breast Atypical Lesions
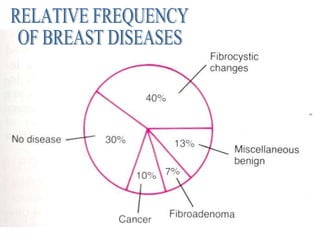
- 1. RELATIVE FREQUENCY OF BREAST DISEASES
- 2. BENIGN TUMORS -Fibroadenoma. -Adenomas. -Papilloma.
- 4. INNOCENT CHANGES IN FIBROADENOMA 1.Fibrohyaline stromal changes. 2.Reactive multinucleated giant cells. 3.Calcification & osteocartilagenous metaplasia. 4.Lactational changes: Plumpy vaculated epithelium with lumenal secretion. 5.Apocrine metaplasia: 15% of fibroadenomas
- 5. ATYPICAL CHANGES IN FIBROADENOMA 1.Myxoid stroma: May be confused with phyloides tumor. Moreover, multiple myxoid fibroadenomas may be associated with endocrinopathies, heart myxoma & cutaneous pigmentation. 2.Hemorrhagic infarct: Occurs in pregnant females, with a bulging red cutsection. The reactive degenerative cellular changes may be confused with a neoplastic condition. 3.Fibroadenoma with an illdefined margin: This occurs due to occurance of fibroadenosis around the tumor, and has been designated as fibroadenomatosis or fibroadenomatoid hyperplasia.
- 6. ATYPICAL CHANGES IN FIBROADENOMA 4.Pronounced stromal element (Fibroadenoma with stromal cellularity). 5.Pronounced epithelial element (Fibroadenoma with atypical epithelial hyperplasia). 6.Squamous metaplasia: If an abundant amount of sq. metaplasia is encountered, this favors the diagnosis of phylloides tumor than fibroadenoma, particularly in old age.
- 7. ATYPICAL CHANGES IN FIBROADENOMA 7.Giant fibroadenoma: Tends to occur in adolescence, more common in black, sometimes bilateral & the tumor exceeds 10cms In diameter. This type is highly cellular, thus also known as fetal fibroadenoma. 8.Complex pattern: A mixture of different patterns (Papillary, apocrine changes, calcification, cystic changes, etc….). Commonly, there is sclerosis, producing architectural distortion & a pseudoinvasive pattern.
- 8. ATYPICAL CHANGES IN FIBROADENOMA 9.Progressive fibroadenoma: Fibroadenoma with a rapid progression in size has been described in immuno diffecient patients & etiologically relate to EBV. 10.Malignant transformation: Less than 0.1%, and may in either epithelial (Focus of CIS) or stromal (Sarcomatous nodule). In the former, the surrounding breast tissue shows CIS in 21% of patients.
- 10. ADENOMA TUBULAR ADENOMA occurs in young age as a well-circuscribed small nodule, characterized by uniform, small tubules, lined by a single layer of epithelium, rimmed by an attenuated myoepithelium in a sparse stroma. COMPLEX ADENOMA is characterised by being cellular with pronounced myoepithelial & stromal element. LACTETIONAL ADENOMA occurs during pregnancy or puerpurium show epithelial secretory activity & some necrosis. APOCRINE ADENOMA is exclusively composed of apocrine cells.
- 11. A B (A) Breast adenoma with a well defined margin (B) Lactational adenoma, with secretary changes
- 12. INTRADUCT PAPILLOMA O ccurs at the age of 48ys, presenting by bleeding per nipple & a small a subareolar mass, not exceeding 3cm. Multiple in 10% of cases & is bilateral in 25% of patients. Its well known by its complex, cellular papillomatous pattern.
- 14. ATYPICAL CHANGES IN INTRADUCT PAPILLOMA 1.Cystic changes: intracystic papilloma, particularly with degenerative changes gives the impression of intracystic papillary carcinoma at the level of cytology. 2.Hemorrhagic infarct 3.Squamous metaplasia 3.Sebacious metaplasia
- 15. ATYPICAL CHANGES IN INTRADUCT PAPILLOMA 4.Pseudoinvasive pattren: This occurs due to stromal sclerosis 2ry to hemorrhage & produces marked architectural distortion & pseudoinfiltrative pattern. But, the double cell layer is preserved. Moreover, the lesion shows areas of hemosiderin deposits & cholestrol clefts. 5.Atypical intraduct papilloma: IHC for myoepithelium highlights the absence of this component in malignancy
- 16. NIPPLE ADENOMA Occurs in the 4 th or 5 th decades as a retroareolar mass & characterised by a complex pattern of florid papillomatosis, adenosis & a distortive, densly sclerotic, stromal componant. A comedo-like patten may be present. Aqanthomatous changes may be observed Moreover, the tumor may erode the nipple, thus confused with paget’s diseases. However the tumor is distinguish from low grade malignancy by: Preservrd myoepithelium -Oval nuclei -Streaming pattern* -Absent atypia -The formation of peripheral clefts* -Absent cribriform pattern
- 17. Absent May be present 5. Apocrine metaplasia More abundant Scanty 10.MITOSIS Prominent, with multiple nucleoli Inconspicuous 9.Nucleolus Hyperchromatic, unevenly distributed Normochromatic, evenly distributed 8.CHROMATIN May be present Absent 11. ِ ABNORMAL MITOSIS Oval-Cigar shaped Oval 7.Nuclei Constant Variable 6.Distance between nuclei Absent Present 4.IHC FOR MYOEPTHELIUM: (SMA, calponin,p63, s100, CK ) Absent (Monotonus) Present 3.TWO CELL TYPES Sparse, delicate without sclerosis A dense, well formed with sclerosis 2.STROMAL STALK Commonly, > 3cm. < 3cm. 1.SIZE PAPILLARY CARCINOMA DUCT PAPILLOMA
- 18. Papillary adencarcinoma, with a delicate core, cigar shaped nuclei, a degree of hyperchromasia, prominent Nuclei & cellular monotony
- 19. BREAST FNAC
- 20. THE ADVANTAGES OF FNAC IN BREAST PATHOLOGY 1.Rapid accurate diagnosis 2.Coast-effective role in the management of breast mass 3.DD. Cystic lesion from solid mass, & has a therapeutic value in the former. 4.Involving the patient in the decision making process when malignancy is encountered 5.Helps to relief patient’s anxiety in benign lesions. 6.Evaluation of associated lymphadenopathy 7.Evaluation of chest wall recurrence 8. Offers fresh material for ancillary studies (FCM, EM, PCR & other cytogenetics & oncogenes studies). 9.Provides a sample for culture and senstivity in inflammatory conditions.
- 21. THE GOLDEN RULE FOR CYTOLOGIC DIAGNOSIS OF ATYPICA BREAST LESIONS 1.Never diagnosis malignancy in the absence of separate malignant cells. 2.Never diagnose malignancy in the presence marked inflammation. 3.Never diagnose malignancy if the aspirate consists of small cells only. 4.If the diagnosis of malignancy is confirmed, it is not possible to differentiate between insitu & invasive tumors. 6.All papillary lesions should be excised for histopathology. 6.Re-evalute your smears & evenly do anther FNAC if your diagnosis is not supported by the clinical & mammographic findings. ٍ Sudha R. KINI, 1999
- 22. BREAST MASS CLINICALLY BENIGN CLINICALLY SUSPECIOUS 2-stage procedure As inpatient +/- FS confirmation EXCISIONAL BIOPSY 1-step procedure As inpatient +/- FS confirmation NO BIOPSY FNAC + FNAC - FNAC + FNAC - Lannin et.al., 1986 COST-EFFECTIVENESS OF BREAST FNAC
- 23. CYTOPATHOLOGY OF ATYPICAL FIBROADENOMA False positive results in few cases of fibroadenomas due to the relatively cellular smears, with epithelial cells showing a degree of atypia & prominent nucleoli. However, these cells are arranged in monolayer, cohesive sheets with a charcteristic branching border (Stag-horn), the presence of the bipolar nacked nuclei (Myoepithelial) & , fibromyxoid stromal fragments are conclusive. But, if the cytological atypia is prominent, it is better to use the term “Atypical or cellular fibroadenoma for complete excision”
- 24. A B A. Branching sheets of FA. B. FA sheets are monolayer. Notice the mild degree of nuc. atypia.
- 25. BENIGN EPITHELIAL TUMORS, FNAC Conventional adenoma is identical to fibroadenoma, with the absenence of the stromal elements. But, the presence of bipolar naked nuclei supports the diagnosis of a benign neoplasm. However, adenomas acquiring papillary patter are very difficult to distinguish from low grade papillary carcinoma. Therefore, excision of the lesion is always recommended. In case of lactetional adenoma, FNAC is the procedure of choice, sparing both the mother & the fetus the problems of surgery & anathesia. Lactetional adeoma smear are usualy cellular, showing dipearsed foamy epithelial cells with a minor degree of reactive nuclear dysplasia (Large nuclei & prominent nucleoli) in a dirty background.
- 26. The flow cytometery can be of a benefit in distinguishing between atypical FA & carcinoma. The FNAC is the ideal procedure for obtaining Fresh samples for the FCM. Cancer is mostly aneuploid ,
- 27. INTRADUCT PROLIFERATIVE LESIONS -UDH -FLAT EPITHELIAL ATYPIA -ADH -DCIS
- 28. UDH WITH INSIGNIFICENT ARCHITECTURAL ATYPIA -SCLEROSING ADENOSIS -MICROGLADULAR ADENOSIS -TUBULAR ADENOSIS -APOCRINE ADENOSIS
- 29. ATYPICAL PATTERNS OF UDH SCLEROSING ADENOSIS: Occurs at the age of 30, presenting with a disk-like, multinodular lump & is characterized by a profound myoepithelial participation. A very low power examination of the lesion will reveal the tendency for architectural respect. The nodule retains a rounded or oval lobular configuration, and is more cellular centrally. During pregnancy this lesion becomes florid with the presence of apocrine metaplasia & a degree of cellular dysplastic changes (Nuclear & nuclear enlargement). Moreover, perineural permeation may occasionally occur.
- 30. A B C (A) High power of sclerosing adenosis, showing irregular glands & dense stroma. (B) Perineural permeation by small Glands in sclerosing adenosis. C. The glands are by BM, positive for collagen IV.
- 31. ATYPICAL PATTERNS OF UDH MICROGLANDULAR ADENOSIS: This is the only benign epithelial lesion, lacking myoepithelial cells & differs from tubular carcinoma by having rounded non-angulated glands & the stromal componant is minimal.
- 32. Microglandular adenosis with minimal stroma & small glands Present in the fat. However, They are wrapped by BM. COLLAGEN-IV
- 33. ATYPICAL PATTERNS OF UDH APOCRINE ADENOSIS: This is a varient of microglandular adenosis, but the glands are larger & lined by an apocrine epithelium. Sometimes a degree of cellular dysplastic changes are present in the form of nuclear atypia & prominence of the nucleoli (ATYPICAL APOCRINE METAPLASIA).
- 34. Apocrine metaplasia, with decapitation secretion & a mild degree of atypia.
- 35. ATYPICAL PATTERNS OF UDH TUBULAR ADENOSIS: Another varient of microglandular adenosis, but with a myoepithelial componant, that helps to distinguish it from tubular carcinoma.
- 36. A case of tubular adenosis, wrapped by A myoepithelial layer, showing +reaction For smooth muscle actin, a feature absent In tubular carcinoma
- 37. ATYPICAL PATTERNS OF UDH EPITHELIOSIS & PAPILLOMATOSIS Azzopardi had found a significance in reporting the degree of epitheliosis in fibrocystic disease: A.MILD: 3-4cells in thickness B.MODERATE TO FLORID: More profound, but still respecting the benign morphology* C.ATYPICAL EPITHELIOSIS: Sharing Some features with ADH*
- 38. FEATURES OF BENIGN EPITHELIOSIS 1.Oval nuclei 2.Normochromatic, with evenly distributed chromatin 3.Slight overlap 4.Small, single, indistinct nuclei 5.Acidophilic, granular cytoplasm, rather than being pale & homogenous. 6.Indistenct cell boundaries (Pseudosyncytial)
- 39. FEATURES OF BENIGN EPITHELIOSIS 7.Streaming effect (Parallel oval nuclei) versus the vertically oriented nuclei in malignancy. 8.Tufts projecting into the lumen. 9.Peripheral clefts (Glomeruloid appearance) 10.The lumens of the cell mass are irregular in size & shape, tending to be elongated rather than rounded, with peripheral location. 11.Bridgies within the cell mass are irregular & the cells within have an oval nuclei, arranged parallel to the longitudinal axis of the bridge. While in malignancy, the nuclei are perpendicular to the long. Axis of the bridge. (Roman arch).
- 40. FEATURES OF BENIGN EPITHELIOSIS 12.Apocrine changes with luminal cytoplasmic blebbing (Decapitation secretion). 13.Myoepithelium is constantly present, on the other hand it is rarely present in intraduct carcinoma. 14.Intralumenal foamy histiocytes, admixed with the epithelial cells. 15.Frequent luminal stromal calcification but not in the form of spherules or psammoma bodies. 16.Absent necrosis.
- 41. FEATURES OF BENIGN EPITHELIOSIS 17.Collagenous spherulosis: Collagenous deposit within the space between the epithelial & myoepithelial cells may be seen, but are less likely to occur with cancer. They may be confused with adenoid cystic carcinoma. 18.Cystic changes are more commonly observed in benign conditions. 19.Positive for HMWK, that is negative in 90% of ADH. 20.EM evidence of intranuclear, electron-dense core inclusions with a corona of radiating filaments (Heloid inclusions).
- 43. Collagenous spherulosis, resembling Adenoid cystic carcinoma
- 44. CLASSIFICATION OF INTRADUCT PROLIFERATIVE LESIONS PBD TRADITIONAL TERMINOLOGY RISK DIN-TERMINOLOGY UDH (usual ductal hyperplasia) 1.5 fold UDH Flat epithelial atypia* DIN 1A ADH 4-5 fold DIN 1B DCIS 8-10 fold -G1 DIN 1C -G2 DIN 2 -G3 DIN 3 * No available data for risk estimation
- 45. FLAT EPITHELIAL ATYPIA Intraduct hyperplastic lesion characterized by replacement of the native epithelium by a 1-5 layers of mildly atypical epithelium, having a monotonous apperance. The proliferating cells are cuboidal-columnar. Luminal secretory content is also encountered. This lesion is also know as columar Cell hyperplasia
- 47. ADH Intraduct hyperplastic lesion characterized, having the following distinctive features from UDH: -Mild to moderate degree of cytological atypia. -Evenly distributed, monomorphic cells. -Micropapillae & tufts formations. -Typical Roman bridges. -Solid & cribriform patterns. -Microcalcification. -A bacground of flat atypia. -Negative for HMWCK in 90% of cases. Thus, several authors consider ADH & low grade DCIS are the same disease entity. However, others tend to separate them.
- 48. ADH VERSUS DCIS Slightly higher Intermediate between UDH & DCIS 5.PI Common Rare 6.ERBB2 overexpression Rounded Ovoid to rounded 4.Nuclear shape Present Absent 3.Nuclear equidistance Slight increase Normal 2.N/C ratio Psmmomatous Non-psammomatous 1.Microcalcification DCIS ADH
- 49. ADH ADH DCIS DCIS
- 50. LOBULAR BREAST LESIONS Distended Normal 5.ACINAR SIZE Obliterated Residual 4.LUMEN Absent Present 3.MYOEPITHELIUM Discohesive Cohesive 2.COHESION Monomorphic Pleomorphic 1.CELL MORPHOLOGY LCIS LOBULAR HYPERPLASIA
- 51. LCIS
- 52. ATYPICAL HPERPLASTIC BREAST CONDITIONS, FNAC These conditions lies in the mid zone grey area between normal fibrocystic disease & true malignancy. Thus, the diagnosis of atypical hyperplastic requires the full knowledge about the diagnostic criteria of both lesions. In fibrocystic disease the cell yeild is low-moderate, with cohesive large monolayer epithelial sheets, having a characteristic honey-comb pattern. Separate, bipolar, naked nuclei are abundant & some of which are attached to the epithelial sheets. There is associated foamy histiocytes & apocrine cells. The nuclei is less than 16 microns with no significant variability in size or shape & is normochromatic with even distribution. The background is clean, free of necrotic debris. Peterse JK. et al, 1989
- 53. ATYPICAL HPERPLASTIC BREAST CONDITIONS, FNAC In malignancy, the smear is highly cellular & the cells are dyscohesive (Dissociated), forming small clusters, with separate malignant cells. The nucleus is larger than 16 micron, with macronucleoli. There is hyperchromasia, with uneven chromatin distribution. There is marked variability in nuclear size & shape with irregular nuclear membrane. The background is necrotic. In atypical proliferative lesions, there is increased cellularity & the ductal epithelial cells are arranged in groups, with mild loss of polarity & slight nuclear overlapping. The nuclei may show marked variability in size & shape, with an enlarged nucleoli. The nucleus is enlarged, but still less than 16 microns. The benign nature of these lesions should be considered by the presence of diverse cell types, including apocrine cells, some mature ductal cells, histiocytes & especially bipolar nuclei Peterse JK. et al, 1989
- 54. Breast cancer with highly cellular smear A B C A B Breast cancer with macronucleol C Breast cancer with overlapping
- 55. ADH (upper Lt.), showing a cellular smear & a mild degree of atypia. However, in another field (Upper Rt.) apocrine cells are encountered, excluding the possibility of malignancy
- 56. ATYPICAL SCLEROSING DUCTAL LESIONS RADIAL SCAR: By mammography & gross examination, it appears small (Less than 1cm.), stellate shaped lesion with a central fibrous core. Thus has great resemblance to IDC. At the microscopic level, it resemble tubular carcinoma. The lesion is characterized by a central dense collagenous core. Ductal formations radiating from the center are composed of two cell types. Characteristically, These glandular structures are larger at the periphery & tend to get smaller as they approach the centre.
- 57. Both sections from a case of a radial scar, notice the stellate outline of the lesion, architectural distortion & the central collagenosis. Glands near the center are small, while those at the periphery are large, & some are cystic.
- 58. SPINDLE CELL LESIONS OF THE BREAST - - - + - - Spindle cell melanoma + - - - - - Myofibroblastic lesions - + - - - + Smooth muscle tumors - - + - - - Sarcomatoid carc. - - + + + + Myoepithelioma CD34 Desmin CK5,6 s100 Calponin SMA TUMOR
- 59. BENIGN VERSUS MALIGNANT PHYLOIDES TUMOR Stromal predominance EQUAL TWO CELL ELEMENTS Heterologous Homologous STROMAL ELEMENTS Infiltrative Pushing MARGIN Simple mast. WE TTT >10/10HPF <10/10HPF MITOSIS Present Absent ANAPLASIA High, haphazardly arranged Low, periductal CELLULARITY >50ys <50ys AGE MALIGNANT BENIGN TUMOR
- 60. ATYPICAL LACTATIONAL CHANGES A rare histological lactational abnormality, termed “Clear cell change”, where the cytoplasm is not vaculated or foamy. The main DD here is lobular carcinoma insitu. But, the later has a larger nuclei. Moreover, These clear cells may show intracytoplasmic Lumina having secretory droplet. Other tumors with clear cell morphology include: Glycogen rich carcinoma, secretory carcinoma, 1ry or metastatic clear cell carcinoma.
- 61. FAT NECROSIS Fat necrosis is most likely to be confused with carcinoma at the clinical, mammography & gross levels of examination. This is due to its clinical hard consistency & the mammographic ominous features including the branching margin & microcalcification. However, at the microscopic level it has a characteristic pattern composed of a granulomatous reaction, rich in foamy histiocytes & closely related to ruptured fat cells. Ancient lesions undergo cavitation, fibrosis, hemosedrin deposition & calcification.
- 62. A.Mammographic picture of breast fat necrosis with branching appearance & marginal micro-calcification. B.Breast carcinoma tends to be more localized A B
- 63. (A) Lipid-laden signet ring histiocytes found in the axillay LN of a woman had a previous procedure that disrupted mammary adipose tissues. Notice the resemblance to metastatic signet ring carcinoma. But, these cells are CK- & CD68+. (B) Chronic mastitis with concentric arrangment of lymphocytes, mimicking lobular carcinoma. But, these cells are CK- & LCA+. A B
- 64. MUCOCELE_LIKE LESION: Mucinous cyst showing pools of extracellular mucin & flattened epith. Lining. However, its cystic gross pattern is helpful for exclusion of mucinous carcinoma.
- 65. RADIO/CHEMO EFFECT VERSUS RESIDUAL CRCINOMA: Therapy induced atypia in the form of cytomegally nucleomegally & multinucleation, as well as, lobular fibrosis. But, the absence of necrosis & the presence of myoepithelium support the diagnosis of therapy effect.
- 66. PSEUDOLYMPHOMA (ALEL): High power examination will reveal the heterogeneous Cellular population & mature plasma cells. In problematic Cases, clonality has to be done.
- 67. THANK YOU
- 68. THANK YOU