Choroidal coloboma
•Descargar como PPT, PDF•
125 recomendaciones•26,321 vistas

Choroidal coloboma

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Choroidal coloboma
Similar a Choroidal coloboma (20)
Más de Laxmi Eye Institute
Más de Laxmi Eye Institute (20)
Último
Último (20)
Choroidal coloboma
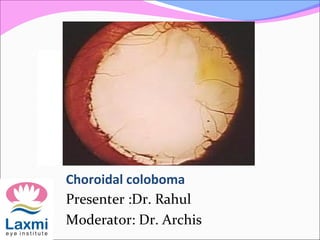
- 1. Choroidal coloboma Presenter :Dr. Rahul Moderator: Dr. Archis
- 2. Coloboma Coloboma (kolobomos :Greek for mutilation) Indicates “a condition where a portion of the structure of the eye is lacking”
- 3. Epidemiology Incidence is 5 per 1,00,000 newborns Prevalence is 1 in 10,000 60% are bilateral Molecular genetics deletion in gene which maps to chromosome 7q26. a mutation in the PAX6 g # Warburg M J Med Genet. 1993 Aug;30(8):664-9
- 4. Types According to site of genesis Typical Atypical As an isolated anomaly with or without microophthalmia Unilateral or Bilateral
- 5. Phenotypic classification It may help the clinician to give a systematic description of the anomalies Two major classes Total Partial
- 6. Aetiological classification • The aetiological classification consists of three classes: • Genetic • Prenatally acquired • Associations • The aetiological classification can be applied to other congenital birth defects and improves counselling of families # # Warburg M J Med Genet. 1993 Aug;30(8):664-9 Classification of microphthalmos and coloboma
- 7. Embryonic Origin The eye is derived from the neural tube (neuroectoderm), from which arise the retina proper The neural crest cells produce the corneoscleral and uveal tunics From the surface ectoderm, lens.
- 8. The earliest stage of eye development is the formation of the paired optic vesicles on either side of the forebrain.
- 9. These growing diverticula expand laterally into the mesoderm of the head and develop a stalk- like connection to the main portion of the rudimentary central nervous system
- 10. In humans, this process begins at about 22 days of development The vesicles continue to grow, their connection to the brain becomes progressively narrower and more stalk-like. This stalks will eventually become the rudiments of the optic nerves.
- 11. There is a seam at the bottom of each stalk, where blood vessels originally run. This seam is known as the optic fissure or choroidal fissure or embryonic fissure.
- 12. The closure starts roughly in the middle of the developing eye, and runs in both directions. This process is start at five week & finished by the seventh week of gestation. If, for some reason, the closure does not happen, a uveal coloboma is formed
- 13. Depending on where the closure did not happen, the baby can have an iris coloboma (front of the fissure) a chorio-retinal coloboma (back of the fissure) any combination of these.
- 14. Uveal coloboma can affect one eye (unilateral) or both eyes (bilateral)
- 15. A uveal coloboma may go from front to back continuous or have “skip lesions”. The fact that the seam runs at the bottom of the stalk is the reason why uveal coloboma is always located in the lower inside corner of the eye.
- 16. Pathophysiology Fusion or closure of the fissure begins in its central portion in the 11-mm embryo and proceeds anteriorly and posteriorly. Closure of the fissure is complete by the sixth week (13-mm stage).
- 17. Pathophysiology In the normal eye, optic fissure closes 33 to 40 days after conception. Failure of the embryonic fissure to close along the inferonasal aspect of the optic cup and stalk That causes Retinal neurosensory elements and RPE precursors fail to become confluent. Due to which underlying choroid fails to differentiate That results in bridge of bare sclera or a cyst formation
- 18. Pathophysiology Anteriorly defects in the neuroectodermally derived iris pigment epithelium produce iris coloboma Posteriorly The entire optic nerve head may be involved in a colobomatous malformation
- 19. Typical/atypical Colobomas are called typical if they are located inferonasally in the region of the fissure Typical colobomas can involve the iris, ciliary body, choroid, or any of the three, and also may involve the optic nerve Atypical colobomas are not related to closure of the fissure
- 20. Multi-system involvement A single-gene disorder with multisystem involvement Aicardi's syndrome Lenz microphthalmia syndrome Meckel's syndrome Warburg's syndrome
- 21. Aicardi's syndrome Absence of corpus callousm Consist of triad - Agenesis of the corpus callosum infantile spasms. morning glory syndrome
- 22. Multisystem disorder without known genetic cause CHARGE association of anomalies colobomatous Microphthalmos heart defects choanal atresia retarded growth genital anomalies ear anomalies or deafness (At least three of the features are necessary for the diagnosis)
- 23. Iris coloboma Total if they involve a whole sector of the iris up to the ciliary body“keyhole” defect Partial if they do not involve a whole sector of the iris may appear as a notch at the pupillary margin
- 24. Histological Complete coloboma involves the whole thickness of the iris Incomplete coloboma involves either the pigment epithelium or the stroma Bridge coloboma mesectodermal tissue forms a pupillary membrane that stretches across the defect
- 25. Lens coloboma Coloboma of the lens is not a true coloboma. No lens tissue is missing An absence of zonular fibers from an underlying colobomatous ciliary body Results in a lack of tension on the lens capsule in that region Notched equator/ Flattening of the inferior lens
- 26. Lens notches can occur wherever zonules are absent or deficient zonular rupture during early surgery
- 27. Ida Manns classification(1937)Ida Manns classification(1937) 1-above the optic disc 2-superior border of optic disc 3-seperated from the optic disc by normal narrow area of retina 4-inferior crescent below the disc 5- isolated gap in the line of fissure 6-area of pigmentary disturbance 7-extreme peripheral coloboma
- 28. 1)area of pigmentary disturbance 2) isolated gap in the line of fissure 3) above the optic disc
- 29. Retinal detachment in colobomaRetinal detachment in coloboma 40% develop RD , accounts for 0.5% of RD in young. May or may not be due to coloboma Vitreous traction cause breaks outside coloboma
- 30. RD due to coloboma is break along edge of coloboma It is difficult to visualise breaks because they are under edge or close to haemorrhage
- 31. Treatment modalitiesTreatment modalities Cryo to anterior margin and photocoagulation to posterior margin Radial buckles (Patnaik et al,1961)-may extend to disc if large.35-57% success rate
- 32. Management of RD with ColobomaManagement of RD with Coloboma Prophylactic laser delimitation of the coloboma margins If RD is due to peripheral coloboma-conventional scleral buckling surgery &Vitrectomy with endophotocoagualation with silicon oil injection
- 33. Management of RD with ColobomaManagement of RD with Coloboma Lensectomy may be required in cases of difficulty in visualizing inferior retina Breaks usually identified AFE easily done as sclera is concave Prolonged inferior tamponade needed-silicon oil gas.
- 35. SRNVM in retinochoroidal coloboma Pathology-absence of choroid with breach in bruch’s membrane leading to vessels entering sub-retinal space. Also RPE abnormalities stimulate budding of choriocapillaris endothelial cells. Laser photocoagulation is advised modality of treatment.
- 36. Cataract in colobomatous eyes Clinically significant cataract develops at a younger age compaired with age-related nuclear sclerotic cataract. Cataract more likely to be denser. Cuniform opacities are more likely to occur earlier. Increased no. of subluxated lens due to associated zonuler deficiency Michael L. Nordlund, Alan Sugar, Sayoko E. Moroi, J Cataract Refract Surg 2000; 26:1035-1040
- 37. Microophthalmos in colobomatous eyes Prevalence 21 per 100,000 82% at least >+7.00D of hypermetropia Coloboma is the second MC association after cataract (22% v/s 44%) Microophthalmos with coloboma may or may not be associated with microcornea Mark J etal Aetiology of severe visual impairment and blindness in Microophthalmia BJO 1994(78);332-334
- 38. Microophthalmos in colobomatous eyes A person with coloboma with microophthalmos with microcornea has a poorer visual prognosis than a person with coloboma with microophthalmos without microcornea Further a newborn with a corneal diameter<5mm has a very poor prognosis Mark J etal Aetiology of severe visual impairment and blindness in Microophthalmia BJO 1994(78);332-334
- 40. Microcornea in colobomatous eyes The term microcornea implies a corneal diameter of less than 10 mm. It thought to occur secondary to an arrest in corneal growth after the fifth month of fetal development. It often occurs with ocular abnormalities such as colobomata and microophthalmos may be present Microcornea accompanies anterior microphthalmos, with crowding of the anterior segment structures
- 41. Management Systemic evaluation Ocular examination. Investigations Axial length Keratometry IOL Master USG UBM
- 42. Management Clinically significant cataract develops at a younger age If a coloboma involves the macula Axial length will be varied so earlier refraction will be important or Axial length may be obtained by locating the preferred fixation point Coloboma with microophthalmos with microcornea – ECCE not a viable option The crystalline lens has been reported to be of normal or slightly larger than normal size #
- 43. Management The lens:eye volume ratio is greater (10 to 32 percent) in these eyes compared with emmetropic eyes (3 to 4 percent) So Phaco-emulsification / manual phaco (SICS) is a viable option Phaco-emulsification—e.g. Slit Nucleotomy, Wooden boot, Petalloid etc. Manual phaco (SICS) —e.g. Sandwich technique, Quarters technique, Phacotrisection etc. Michael L. Nordlund, Alan Sugar, Sayoko E. Moroi, J Cataract Refract Surg 2000; 26:1035- #
- 44. Management Minimal mydriasis or reactive miosis should be anticipated Iris retractors / multiple sphicterotomies CCC run-off or tear can occur Recommendations for CCC Eccentric capsulorhexis Increased magnification with dye assistance Oblique illumination Two stage CCC Good chamber maintainence with viscoelastic Nucleus sculpting / Nucleus cracking at opposite meridian + PCIOL@90° to tear Endothelial losses Shell technique can be used Michael L. Nordlund, Alan Sugar, Sayoko E. Moroi, J Cataract Refract Surg 2000; 26:1035- #
- 46. Management Anterior vitrectomy Vitreous loss – Prolapse through PC rent Prolapse through colobomatous area without PC rent Optimal centeration of the optic with the ectopic pupil to avoid post-op mono-ocular diplopia Puppiloplasty may be required Avoid silicon material IOLs As future VR surgery may entail the use of silicon oil # Michael L. Nordlund etal Phacoemulsification and intraocular lens placement in eyes with cataract and congenital coloboma: visual acuity and complications J Cataract Refract Surg 2000; 26:1035-1040
- 47. Prognosis The prognosis for vision depended on the phenotype of the better eye Microphthalmos with cyst has the worst prognosis Coloboma with microcornea and microphthalmos a poor prognosis Coloboma with only microcornea has an intermediate prognosis Simple coloboma has the best prognosis A corneal diameter <6 mm had a poor visual prognosis whereas a corneal diameter >10 mm had a good prognosis Time of surgery Type of surgery Hornby SJ, etal Ophthalmology. 2000 Mar;107(3):511-20 Visual acuity in children with coloboma Michael L. Nordlund, Alan Sugar, Sayoko E. Moroi, J Cataract Refract Surg 2000; 26:1035- 1040