02 vascular pathology
•Descargar como PPT, PDF•
1 recomendación•254 vistas

Are localized abnormal dilations of arteries. Result due to weakening of the vessel wall. Have the tendency to rupture. Law of Laplace: states that as the diameter of aneurysm increases the wall stress increases : further enlargement and rupture is inevitable. Aneurysms are classified by: Location ( e.g abdominal aortic aneurysm) Etiology (e.g. syphlitic aneurysm) Shape (e.g. fusiform , saccular)

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a 02 vascular pathology
Similar a 02 vascular pathology (20)
Más de med_students0
Más de med_students0 (20)
Último
Último (20)
02 vascular pathology
- 1. 1
- 2. 2 Aneurysms Are localized abnormal dilations of arteries. Result due to weakening of the vessel wall. Have the tendency to rupture. Law of Laplace: states that as the diameter of aneurysm increases the wall stress increases : further enlargement and rupture is inevitable. Aneurysms are classified by: Location ( e.g abdominal aortic aneurysm) Etiology (e.g. syphlitic aneurysm) Shape (e.g. fusiform , saccular)
- 3. 3
- 5. 5 Causes of aneurysm 1. Atherosclerosis: MCC causes arterial wall thinning due to destruction of media 2. Cystic medial degeneration 3. Syphilis 4. Trauma 5. Polyarteritis nodosa (PAN) 6. Congenital defects : EDS, MS 7. Infections (also called mycotic aneurysms).
- 6. 6 Aneurysm complications 1. Rupture 2. Impingement on adjacent structures 3. Occlusion of proximate vessel 4. Embolism from mural thrombosis
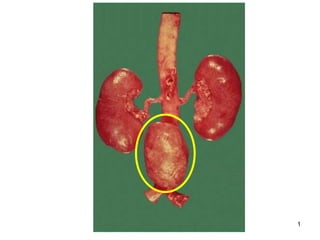
- 7. 7 Abdominal aortic aneurysms (AAA) Are complications of atherosclerosis MC type of aneurysm (MC in men>55 yrs) Usually located below the renal artery orifices proximal to bifurcation Pathogenesis: 1. Atherosclerosis weakens vessel wall: (no vasa vasorum below renal artery orifice). Lumen of aneurysm fills with atheromatous debris and blood clots. 2. Familial factors and structural defects in connective tissue
- 8. 8
- 10. 10 Abdominal aortic aneurysms Clinical findings: Majority are asymptomatic Symptomatic: a pulsatile mass can be palpated. Rupture: is the most common complication Abrupt onset of severe back pain is followed by hypotension from blood loss in retroperitoneum and shock. Diagnosis: Abdominal ultrasound is the gold standard test.
- 11. 11 Syphilitic aneurysm Cardiovascular manifestation of tertiary syphilis. Usually occurs in men 40-55 years of age. Is due to inflammation of aortic vasa vasorum.
- 12. 12 Syphilitic aneurysm: Pathogenesis T.pallidum infects the vasa vasorum of the ascending and transverse portions of aortic arch. Causing endarteritis obliterans (of the vasa vasorum). Characteristic plasma cell infiltrate in vessel wall. Ischemia focal necrosis and scarring of media Dilation of the aorta and aortic valve ring. Roughened intimal surface imparts a “tree bark” appearance.
- 14. 14 Syphilitic aneurysm Clinical findings: Aortic regurgitation with left ventricular hypertrophy. Bounding pulse: due to increased LVEDV Increased stroke volume. Brassy cough: left recurrent laryngeal nerve is stretched by the aneurysm. Respiratory difficulty: due to airway encroachment. Rupture leads to rapid death. Diagnosis: Aortography Calcification in the arch of aorta: highly predictive of syphilitic aneurysm.
- 15. 15 Syphilitic aneurysm "Tree-barking“ of aorta
- 16. 16 Mycotic aneurysm Result from weakening of the vessel wall due to a microbial infection. Causes: Septic embolism Bacteria: Bacteroides, Pseudomonas aeruginosa, Salmonella species Infective endocarditis Fungal vasculitis: Aspergillus, Mucor, Candida are vessel invaders) Clinical findings: thrombosis with or without infarction, rupture and hemorrhage.
- 17. 17 Berry aneurysm Are small spherical aneurysms most commonly located at the bifurcation of cerebral vessels. Increased intravascular pressure and weakness in arterial wall lead to their formation. They can rupture and lead to fatal Subarachnoid hemorrhage.
- 18. 18
- 19. 19 Berry aneurysm :Pathogenesis Arise due to defect in cerebral vessels: Vessels lack muscular layer at the point of bifurcation Pressure at the weak point Loss/degeneration of internal elastic membrane Berry aneurysm Associations: any cause of HT predisposes to berry aneurysms: Essential hypertension Adult polycystic kidney disease Rupture of a berry aneurysm blood into subarachnoid space
- 20. 20
- 21. 21
- 22. 22 Berry aneurysm Clinical findings: Subarachnoid hemorrhage: Sudden onset of severe occipital headache “worst headache I ever had”. Loss of consciousness. Nuchal rigidity from irritation of meninges. Complications: Death from bleeding Rebleed, neurological deficits. Diagnosis: CT scan as screen Angiography confirms the diagnosis.
- 23. 23 Aortic dissection Definition: blood from the vessel lumen enters an intimal tear and dissects a path along the length of the vessel. Usually involves the wall of the ascending aorta.
- 24. 24 Epidemiology Aortic dissection occurs in two groups: Most common group: Men (mean age of 40-60 years) with hypertension. Young patients with a connective tissue disorder: Marfan syndrome, Ehlers Danlos syndrome.
- 25. 25 Pathology and Pathogenesis The basis of dissecting aortic aneurysm is weakening of aortic media. Predisposing conditions: Cystic medial degeneration (CMD): is characterized by focal loss of elastic and muscle fibers in tunica media. Leads to cystic spaces filled with myxoid material. The cause is unknown. Seen in different conditions ….
- 27. 27 Pathology and Pathogenesis Risk factors for CMD: Increase in wall stress: Hypertension, pregnancy Defect in connective tissue: Marfan Syndrome : defect in elastic tissue (fibrillin) Ehlers Danlos syndrome : defect in collagen Aging, Copper deficiency
- 28. 28 Cause of dissection Intimal tear: Due to HT or underlying structural weakness in the media Usually occurs within 10 cm of aortic valve Column of blood dissects under arterial pressure through the areas of weakness Progresses proximally and or distally.
- 29. 29 Intimal tear
- 31. 31 Aortic dissection Types: Type A : involves ascending aorta Most common and worst type Type B: Begins below the subclavian artery Classification of dissection into types A and B.
- 32. 32 Aortic dissection Clinical findings: Acute onset of severe retrosternal pain radiating to the back. Pain described as tearing. AV regurgitation: due to aortic valve ring dilation; a radiograph or echocardiogram shows widening of the aortic valve root. Loss of upper extremity pulse: compression of the subclavian artery. Rupture: usually into the pericardial sac (tamponade most common cause of death), pleural cavity or peritoneal cavity. Diagnosis: Increased aortic diameter on chest X ray.