Congenital ptosis
•Descargar como PPTX, PDF•
53 recomendaciones•13,784 vistas

Complete information about congenital ptosis.

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Congenital ptosis
Similar a Congenital ptosis (20)
Último
Último (20)
Congenital ptosis
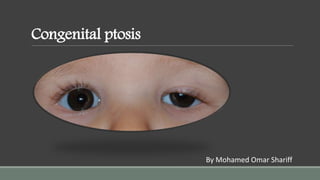
- 1. Congenital ptosis By Mohamed Omar Shariff
- 2. PTOSIS Ptosis is a Greek word which means: act of falling Abnormal drooping of the upper eyelid is called ptosis. Normally, upper lid covers about upper one-sixth of the cornea i.e., about 2 mm. In ptosis it covers more than 2 mm. Normal Eyelids Bilateral Congenital Ptosis
- 3. Congenital ptosis Types and etiology It is associated with congenital weakness (maldevelopment) of the levator palpebrae superioris (LPS). It may occur in the following forms: 1. Simple congenital ptosis (not associated with any other anomaly) 2. Congenital ptosis with associated weakness of superior rectus muscle. 3. As a part of blepharophimosis syndrome, which comprises congenital ptosis, blepharophimosis,telecanthus and epicanthus inversus. 4. Congenital synkinetic ptosis (Marcus Gunn jawwinking ptosis). In this condition there occurs retraction of the ptotic lid with jaw movements i.e., with stimulation of ipsilateral pterygoid muscle.
- 4. Simple congenital ptosis 1.Pathogenesis: Probably failure of neuronal migration or development with muscular sequelae; a minority are hereditary. 2.Signs •Unilateral or bilateral ptosis of variable severity. •Absent upper lid crease and poor levator function. •In downgaze the ptotic lid is higher than the normal because of poor relaxation of the levator muscle. This is in contrast to acquired ptosis in which the affected lid is either level with or lower than the normal lid on downgaze. •Following surgical correction the lid lag in downgaze may worsen.
- 5. 3.Associations: •Superior rectus weakness may be present because of its close embryological association with the levator. •Compensatory chin elevation in severe bilateral cases. •Refractive errors are common and more frequently responsible for amblyopia than the ptosis itself. 4.Treatment should be carried out during the preschool years once accurate measurements can be obtained, although it may be considered earlier in severe cases to prevent amblyopia. Most cases require levator resection (see below).
- 7. Blepharophimosis syndrome (Blepharophimosis ptosis and epicanthusinversus syndrome) 1.Inheritance is usually AD. BPES 1 (with premature ovarian failure) and BPES 2 (without premature ovarian failure) are caused by type 1 mutations in FOXL2 gene on chromosome 3. 2. Signs •Moderate to severe symmetrical ptosis with poor levator function. •Telecanthus and epicanthus inversus •Poorly developed nasal bridge and hypoplasia of the superior orbital rims. 3. Treatment initially involves correction of epicanthus and telecanthus, followed a few months later by bilateral frontalis suspension. It is also important to treat amblyopia, which is present in about 50% of cases.
- 9. Marcus Gunn jaw-winking syndrome About 5% of all cases of congenital ptosis manifest the Marcus Gunn jaw-winking phenomenon. The vast majority are unilateral. Although the exact aetiology is unclear, it has been postulated that a branch of the mandibular division of the 5th cranial nerve is misdirected to the levator muscle. 1.Signs •Retraction of the ptotic lid in conjunction with stimulation of the ipsilateral pterygoid muscles by chewing, sucking, opening the mouth or contralateral jaw movement. •Less common stimuli to winking include jaw protrusion, smiling, swallowing and clenching of teeth. •Jaw-winking does not improve with age, although patients may learn to mask it.
- 10. 2.Surgery should be considered if jaw-winking or ptosis represents a significant functional or cosmetic problem. Although no surgical treatment is entirely satisfactory possible approaches include: a.Unilateral levator resection for mild cases with levator function 5 mm or better. b.Unilateral levator disinsertion and part resection with ipsilateral brow (frontalis) suspension for more severe cases. c.Bilateral levator disinsertion and part resection with bilateral brow suspension to produce a symmetrical result.
- 12. Clinical evaluation Following scheme may be adopted for work up of a ptosis patient: I. History. It should include age of onset, family history, history of trauma, eye surgery and variability in degree of the ptosis. II. Examination 1. Exclude pseudoptosis (simulated ptosis) on inspection. Its common causes are: microphthalmos, anophthalmos, enophthalmos and phthisis bulbi. 2. Observe the following points in each case: i. Whether ptosis is unilateral or bilateral. ii. Function of orbicularis oculi muscle. iii. Eyelid crease is present or absent. iv. Jaw-winking phenomenon is present or not. v. Associated weakness of any extraocular muscle. vi. Bell’s phenomenon (up and outrolling of the eyeball during forceful closure) is present or absent.
- 13. 3. Measurement of amount (degree) of ptosis. In unilateral cases, difference between the vertical height of the palpebral fissures of the two sides indicates the degree of ptosis (Fig. 14.33). In bilateral cases it can be determined by measuring the amount of cornea covered by the upper lid and then subtracting 2 mm. Depending upon its amount the ptosis is graded as Mild 2 mm Moderate 3 mm Severe 4 mm 4.Margin–reflex distance is the distance between the upper lid margin and the corneal reflection of a pen torch held by the examiner, at which the patient is directly looking ; normal is 4–4.5 mm.
- 15. 5.Levator function (upper lid excursion) is measured by placing a thumb firmly against the patient’s brow to negate the action of the frontalis muscle, with the eyes in downgaze (Fig. 1.51A). The patient then looks up as far as possible and the amount of excursion is measured with a rule (Fig. 1.51B). Levator function is graded as normal (15 mm or more), good (12–14 mm), fair (5–11 mm) and poor (4 mm or less).
- 17. 6. Photographic record of the patient should be maintained for comparison. Photographs should be taken in primary position as well as in up and down gazes. Anatomy of the Eyelid 1.The levator aponeurosis fuses with the orbital septum about 4 mm above the superior border of the tarsus (Fig. 1.57). Its posterior fibres insert into the lower third of the anterior surface of the tarsus. The medial and lateral horns are expansions that act as check ligaments. Surgically, the aponeurosis can be approached through the skin or conjunctiva.
- 18. 2.Müller muscle is inserted into the upper border of the tarsus and can be approached transconjunctivally. 3.The inferior tarsal aponeurosis consists of the capsulopalpebral expansion of the inferior rectus muscle and is analogous to the levator aponeurosis. 4.The inferior tarsal muscle is analogous to Müller muscle.
- 20. Treatment I. Congenital ptosis. It almost always needs surgical correction. In severe ptosis, surgery should be performed at the earliest to prevent stimulus deprivation amblyopia. However, in mild and moderate ptosis, surgery should be delayed until the age of 3-4 years, when accurate measurements are possible. Congenital ptosis can be treated by any of the following operations: 1. Conjunctiva–Müller resection Indications include mild ptosis with levator function of at least 10 mm. This includes most cases of Horner syndrome and very mild congenital ptosis. The maximal lift is 2–3 mm. Technique. Müller muscle and overlying conjunctiva are excised (Fig. 1.58A) and the resected edges reattached (Fig. 1.58B).
- 22. Levator resection 1.Indications are ptosis of any cause provided levator function is at least 5 mm. The extent of resection is determined by the amount of levator function and the severity of the ptosis. 2.Technique involves shortening of the levator complex through either an anterior (skin – Fig. 1.59) or posterior (conjunctival) approach.
- 23. SKIN INCISION DISSECTION AND RESECTION OF LEVATOR APONEUROSIS
- 24. LEVATOR REATTACHMENT TO TARSAL PLATE
- 25. Brow suspension 1.Indications •Severe ptosis (>4 mm) with very poor levator function (<4 mm). •Marcus Gunn jaw-winking syndrome. •Ptosis associated with aberrant regeneration of the 3rd nerve. •Blepharophimosis syndrome. •Ptosis associated with 3rd nerve palsy. •Unsatisfactory result from previous levator resection. 2.Technique involves suspension of the tarsus from the frontalis muscle with a sling consisting of autologous fascia lata (Fig. 1.60) or non-absorbable material such as prolene or silicone.
- 26. SITE OF INCISIONS MARKED THREADING OF FASCIA LATA STRIPS
- 27. TIGHTENING AND TYING OF STRIPS