Respiration upload4
•Descargar como PPTX, PDF•
2 recomendaciones•2,059 vistas

The document summarizes various topics related to respiratory physiology including: 1. The respiratory response to high altitude includes hyperventilation, respiratory alkalosis, and increased renal bicarbonate excretion to resolve alkalosis. 2. Acute mountain sickness symptoms are caused by hypoxia and alkalosis, while prevention involves acclimatization. 3. Periodic breathing involves deep then shallow breathing in cycles, like Cheyne-Stokes respiration occurring every 40-60 seconds. 4. Hypoxemia can result from problems in oxygen delivery or uptake in the lungs, blood, or tissues.

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (20)
Similar a Respiration upload4
Similar a Respiration upload4 (20)
Más de Physiology Lectures
Último
Último (20)
Respiration upload4
- 2. Respiratory Response to High Altitude Plus, increased: No. of RBCs, diffusing capacity of the lungs, vascularity of the peripheral tissues, ability of tissue cells to use O2 (despite low Po2)
- 3. Respiratory Response to High Altitude Hypoxemia causes hyperventilation Hyperventilation causes decrease in Pco2 & respiratory alkalosis (RA) These 2 inhibit CNS respiratory centre (‘offsetting’ ++ drive of hypoxemia) Body’s solution: Renal HCO3- excretion increased – RA resolved (via increased excretion of CSF HCO3-) Hyperventilation now will not be ‘offset’ because now, O2 is the drive* via PCR!
- 4. Acute Mountain Sickness Symptoms due to hypoxia and RA Headache, fatigue, dizziness, nausea, palpitations, and insomnia Pulmonary & cerebral edema are serious Prevention: Acclimatization Treatment: Acetazolamide
- 5. Respiratory Response to Exercise CNS influences respiratory response Anticipatory increase in ventilation at exercise onset Leads to an initial decrease in Pco2 Afterwards, the increased Pco2 ‘matches’ the ventilation rate
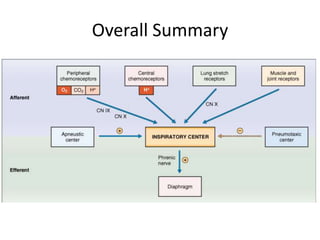
- 6. Summary
- 7. Periodic Breathing Person breathes deeply (short interval) - then breathes slightly or not at all for an additional interval Cycle repeating itself over and over Cheyne-Stokes breathing slowly waxing and waning respiration occurring about every 40 to 60 secs
- 8. Hypoxemia
- 9. Hypoxia & O2 therapy Decreased O2 delivery to the tissues Causes: Inadequate oxygenation of blood in lungs (extrinsic reasons) Oxygen deficiency in atmosphere Hypoventilation (neuromuscular disorders) Disease of the lung itself Abnormal V/Q Damaged respiratory membrane Decreased compliance etc Venous-to-arterial shunts (“right-to-left” cardiac shunts) Inadequate O2 transport to tissues by blood Anemia or abnormal hemoglobin General circulatory deficiency Localized circulatory deficiency (peripheral, cerebral, coronary vessels) Tissue edema Inadequate tissue capability of using O2 Cyanide poisoning Vitamin-B deficiency (Beri-beri)
- 10. Hypoxia Hypoxic hypoxia PO 2 of the arterial blood is reduced; Anemic hypoxia Arterial PO 2 is normal but amount of Hb reduced Stagnant or ischemic hypoxia Blood flow to a tissue is so low that adequate O2 is not delivered (despite normal PO2 & Hb) Histotoxic hypoxia Tissue cells cannot make use of the O2 supplied
- 11. Hypoxia Signs Cyanosis Tachypnea (rate) & Hyperpnea (depth) Tachycardia
- 12. Respiratory Control Dysfunction Cheyne-stokes breathing Biot’s breathing Ondine’s curse Sleep-Apnea syndromes Obstructed apnea Non-obstructed (central) apnea
- 13. CLINICAL CASES
- 14. Nitrogen NarcosisRaptures of the Depth! At sea-level pressure, nitrogen has no significant effect on bodily function But at high pressures (deep sea diving) – varying degrees of narcosis Mild narcosis appear is about 120 feet (jovial, no-cares) At 150- 200 feet, diver becomes drowsy At 200 – 250 feet, strength wanes considerably, & diver often becomes too clumsy to perform the work required Beyond 250 feet, the diver usually becomes almost useless
- 15. Oxygen Toxicity When Po2 in blood rises above 100 mm Hg Amount of O2 dissolved in blood increases markedly Delivery of O2 to tissues increases Symptoms: Nausea, muscle twitchings, dizziness, disturbances of vision, irritability, & disorientation Brain seizures – coma Oxygen free radical accumulationcauses toxicity (superoxides hydrogen peroxide)*
- 16. Oxygen Toxicity Acute Exposure to very high Po2 for prolonged periods of time Symptoms develop as mentioned Chronic Exposure to moderately high Po2 doesn’t lead to tissue symptoms But lung passageway congestion, sore throat, substernal distress, pulmonary edema, and atelectasisbegin to develop* In infants with RDS O2 therapy leads to Chronic condition characterized by lungs cycts & densities (bronchopulmonary dysplasia) + retinopathy of prematurity (retrolentalfibroplasia)
- 17. Hyperbaric O2 therapy Intense oxidizing properties of high-pressure oxygen (hyperbaric oxygen) can have valuable therapeutic effects Especially use in infectious conditions caused by organisms that thrive in anaerobic conditions Gas gangrene (clostridial organisms) Also useful in decompression sickness, arterial gas embolism, CO poisoning, osteomyelitis, and MI
- 18. CO2 toxicity At very high Pco2 – CO2 depresses respiratory centres
- 19. Decompression Sickness Nitrogen dissolves in body fluids Nitrogen is not metabolized in body Hence to remove it – one needs to exhale it! In high pressure scenarios: Alveolar PN2 is high – so is tissue PN2 High P in blood gases AND outside body maintains the dissolved state of N2 in tissues Sudden drop in P may cause bubbles to form – escape of N2 from tissues* (decompression)
- 20. Decompression Sickness Symptoms are mostly due to bubble embolism Pain in joints (‘bends’) CNS symptoms: Dizziness (5% cases) Paralysis* or collapse and unconsciousness in 3% cases Respiratory symptoms (‘chokes’) caused by massive numbers of microbubbles plugging lungs capillaries; Leading to serious shortness of breath, severe pulmonary edema & may be death Prevention Divers to ascend slowly Tank Decompression
- 21. Asthma Disease of airway inflammation and airflow obstruction Characterized presence of intermittent symptoms: wheezing, chest tightness, shortness of breath (dyspnea), and cough together with demonstrable bronchial hyperresponsiveness Pathophysiology Airway resistance increases due to airway inflammation, smooth muscle hyperresponsiveness, and airway narrowing, small-caliber peripheral airways are the site of increased resistance This is worsened by the superimposed mucus hypersecretion and by any additional bronchoconstrictor stimuli
- 22. Asthma Contd.. Pathophysiology Airway obstruction occurs diffusely but not homogeneously As a result, variability in V/Q mismatch occurs Areas of low & high V/Q ratios exist Low V/Q ratio regions - contributes to hypoxemia Pure shunt is unusual in asthma Arterial CO2 tension is usually normal to low (due to increased ventilation seen with asthma exacerbations) Hypercapnia - late and ominous sign!
- 23. Asthma – Symptoms & Signs Cough wheezing Dyspnea & Chest tightness Tachypnea and tachycardia Pulsus paradoxus Hypoxemia Hypercapnia and respiratory acidosis (severe asthma) Obstructive defects by pulmonary function testing: Normal between attacks (mild asthma) During attacks: Decreased FEV1, FEV1/FVC, peak expiratory flow rates Bronchial hyperresponsiveness 20% decrease in FEV1 in response to a provoking factor OR 20% increase in the FEV1 in response to an inhaled bronchodilating
- 24. COPD Chronic bronchitis Productive cough for 3 months of the year for 2 consecutive years Productive cough Wheezing Inspiratory and expiratory coarse crackles Tachycardia Imaging: increased lung volumes with relatively depressed diaphragms consistent with hyperinflation Pulmonary function tests: FEV1, FVC, and the FEV1/FVC – all reduced Blood gases: hypoxemia is common (abnormal V/Q) Polycythemia present
- 25. COPD Emphysema Abnormal permanent enlargement of the airspaces distal to the terminal bronchioles, accompanied by destruction of their walls Decreased breath sounds Tachycardia Imaging: hyperinflation Pulmonary function tests: all reduced Blood gases: may be normal (but exercise induces decreased Po2) Polycythemia present
- 27. Clinical Scenarios Restrictive Lung Disease (Interstitial Lung Disease) A category of extrapulmonary, pleural, or parenchymal respiratory diseases that: Restrict lung expansion Decreased lung volume Increased work of breathing Inadequate ventilation and/or oxygenation Pulmonary function test demonstrates a decrease in the forced vital capacity
- 28. Non-Respiratory Functions of Lungs Immune Acid base balance Blood reservoir Conversion of precursor molecules
- 29. Respiratory Function Tests Max. voluntary ventilation Respiratory responses to CO2 Forced vital capacity Diffusion capacity FRC & VC Blood gases
Notas del editor
- *This plus the example of respiratory acidosis (in COPD) are examples whereby hypoxia is the drive of ventilation via PCR
- Acute Altitude Sickness The initial phase of ascent to high altitude is associated with a constellation of complaints, including headache, fatigue, dizziness, nausea, palpitations, and insomnia. The symptoms are attributable to the initial hypoxia and respiratory alkalosis, which abate when the adaptive responses are established. Many AMS symptoms are caused by hypoxia-induced cerebral blood vessel dilation, which puts pressure on adjacent neuronal tissue. The hypoxia-induced cerebral dilation accounts for the headache, dizziness, nausea, and sleep disturbance. Dehydration can exacerbate these symptoms. The most serious symptoms of AMS are a result of edema (abnormal fluid accumulation) in the lungs and brain. Severe hypoxia causes endothelial cells to become leaky. The edema that is the most life threatening is pulmonary edema. The problem arises because of the oxygen paradox (i.e., hypoxia causes blood vessels to dilate in systemic circulation but causes vasoconstriction in the pulmonary circulation). The hypoxia-induced pulmonary vasoconstriction increases pulmonary vascular resistance. The heart trying to pump blood through ‘water-soaked lungs’ further complicates the situation. As the lungs fill up with water, victims become increasingly short of breath and often spit up foamy blood. Severe pulmonary edema causes death as a result of heart failure.AMS can be avoided with care. One precaution is to avoid caffeine and alcohol, which tend to exacerbate AMS. A second precaution is to ascend the mountain slowly. Most AMS occurs following a rapid ascent. The third precaution of high-altitude climbing is to follow the climbers‘ ‘golden rule’: climb high and sleep low, meaning that a climber should stay a few days at base camp to acclimatize, then climb slowly to a higher camp, and return to base camp for the night. This procedure is repeated a few times, each time extending the time spent at higher altitudes to let the body acclimatize to the lower oxygen tension. The general rule is not to ascend more than 300 m (1,000 feet) per day to sleep. This means a climber can climb from 3,000 m (10,000 feet) to 4,500 m (15,000 feet) in one day, but then descend back to 3,300 m (11, 000 feet) to sleep. This explains why climbers need to spend days and/or weeks at a time to acclimatize before they can reach a high peak.Acetazolamide may help speed up the acclimatization process and can treat mild cases of altitude sickness. It reduces fluid formation and helps reduce the severity of cerebral edema. The drug also forces the kidneys to excrete bicarbonate, the base form of carbon dioxide, thus counteracting the effects of hyperventilation that occurs at altitude.
- Discuss O2 therapy with causes
- Uploaded document
- The mechanism of the narcotic effect is believed to be the same as that of most other gas anesthetics. That is, it dissolves in the fatty substances in neuronal membranes and, because of its physical effect on altering ionic conductance through the membranes, reduces neuronal excitability.Divers breath a mixture of air as follows:MOD: max. operating depthMIX: misture of O2/Helium
- *these are normally formed as well, but are neutralized by cellular anti-oxidant agents; however at very high tissue Po2, the whole system gets saturated with oxygen free radicals…
- *The reason for this effect in the lungs butnot in other tissues is that the air spaces of the lungsare directly exposed to the high oxygen pressure, butoxygen is delivered to the other body tissues at almostnormal Po2 because of the hemoglobin-oxygen buffersystem.
- Table shows dissolution of N2 at varying degrees of depth*as wud happen in sudden ascend of a diver
- *paralysis may be temporary, but in some instances, damage is permanentTable shown: Decompression tables have been prepared by the U.S. Navy that detail procedures for safe decompression.Data given is for a diver who has been breathing air and has been on the sea bottom for 60 minutes at a depth of 190 feet is decompressed.