Corynebacterium
•Descargar como PPTX, PDF•
194 recomendaciones•79,870 vistas

This document provides information on Corynebacterium, including Corynebacterium diphtheriae which causes diphtheria. It discusses the morphology, cultural characteristics, biotypes, virulence factors, pathogenesis, clinical presentation, complications, laboratory diagnosis and epidemiology of C. diphtheriae. The key points are that C. diphtheriae is a gram-positive bacillus that produces a powerful exotoxin causing diphtheria, a serious infection of the upper respiratory tract, and immunization is important for control of the disease.

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Similar a Corynebacterium
Similar a Corynebacterium (20)
Más de Guddeti Prashanth Kumar
Último
Último (20)
Corynebacterium
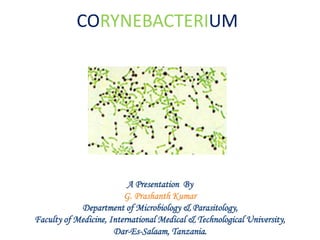
- 1. CORYNEBACTERIUM A Presentation By G. Prashanth Kumar Department of Microbiology & Parasitology, Faculty of Medicine, International Medical & Technological University, Dar-Es-Salaam, Tanzania.
- 2. INTRODUCTION • Corynebacteria / “Coryneform bacteria” – a group of non-spore forming, gram- positive bacilli, tend to be clubbed or irregularly shaped; (coryne = club) • Corynebacterium diphtheriae the causative agent of Diphtheria is the major pathogen in this group. • Other pathogenic corynebacteria are: • C. Ulcerans: Diphtheria like lessions. • Corynebacteria Causing Superficial skin infections: C. minutissimum and C. tenuis. • Diphtheriods: Normal commensals in throat, skin and conjunctiva.
- 3. HISTORY • Hippocrates provided the first clinical description of diphtheria in the 4th century B.C. • Bretonneu (1821), a French army surgeon, described the unique clinical characteristics of the disease, and used the term ‘dipht`erie’ to signify the tough leathery pseudomembrane that occurs in oropharynx and some times in nasopharynx; (diphtheros = leather)
- 4. HISTORY • The bacterium that caused diphtheria was first described by Klebs in 1883, and was cultivated by Loeffler in 1884, who applied Koch's postulates and properly identified Corynebacterium diphtheriae as the agent of the disease. • In 1884, Loeffler concluded that C. diphtheriae produced a soluble toxin, and thereby provided the first description of a bacterial exotoxin. • Roux and Yersin (1888) discovered the diphtheria exotoxin and established its pathogenic effects. • The antitoxin was described by von Behring(1890).
- 6. MORPHOLOGY • Slender Gram-positive rods, pleomorphic; easily decolousised; • 0.6-0.8μ diameter and 3-6 μ length; • Irregular swelling at one or both ends (‘club shaped’); • Non-capsulate, Non-sporing and nonmotile • Granules containing polymetaphosphate are seen in the cells; • Take up bluish purple color against lightly stained cytoplasm, when stained with Loeffler’s Methylene Blue, and hence called ‘Metachromatic granules’; • Also called, ‘volutin granules’ or ‘Babes Ernst granules’; • They are often situated at poles- ‘polar bodies’
- 7. MORPHOLOGY • Special stains for demonstrating the granules : – Albert’s stain – Neisser’s stain – Ponder’s stain • The bacilli are arranged in pairs, palisades or small groups; the bacilli lie at various angles to each other, resembling the letters, V or L; • This is called, “Chinese letter pattern” or “cuneiform pattern”;
- 8. CULTURAL CHARACTERISTICS • Aerobe and facultative anaerobe; • Optimum temperature is 370C • Growth scanty on ordinary media; • Enrichment with: blood, serum or egg is necessary for good growth; • Potassium tellurite(0.04%) acts as a ‘selective agent’, as it inhibits growth of most oral commensals and retards the growth of Candida albicans and S.aureus;
- 9. MEDIA FOR CULTIVATION • Blood agar • Loeffler’s serum slope • Tellurite blood agar • Hoyle’s tellurite lysed-blood agar • Tinsdale’s medium (cystine added to tellurite containing agar)
- 10. COLONY CHARACTERISTICS • Blood agar : small, granular and gray with irregular edges; Hemolysis may or may not present; • Loeffler’s serum slope: – Very rapid growth; – Colonies in 6-8 hrs – Initially circular white opaque colonies and acquire yellowish tint on incubation
- 11. COLONY CHARACTERISTICS • Tellurite blood agar: – Growth slow; colonies seen after 48 hrs; – The colonies are brown to black with a brown- black halo because the tellurite is reduced to metallic tellurium; – Staphylococcus also produce such colonies A diagrammatic representation
- 12. COLONY CHARACTERISTICS • Tinsdale’s medium (also contain cystine in addition to tellurite): – Grey black colonies with dark brown haloes indicate C.diphtheriae and C.ulcerans (these contain cystinase)
- 13. BIOTYPES • McLeod and Anderson classified diphtheria bacilli, based on the colony characteristics on Tellurite medium and other properties like biochemical reactions and severity of disease; • 3 biotypes : – gravis – intermedius – mitis • 4th biotype : belfanti has also been described
- 14. Feature gravis intermedius mitis Morphology shot rods, few granules some degree of pleomorphism long barred forms poor granulation Pleomorphism long curved prominent granules Pleomorphism Colony on tellurite blood agar (48 hrs) Daisy head colony (flat colony with raised dark centre and crenated edge; radial striations) Frog's egg colony (dull granular centre with glistening periphery and lighter ring near edge) Poached egg colony (shiny , flat with central elevation) Consistency of the colonies Brittle not easily emulsifiable intermediate soft, buttery easily emulsifiable Hemolysis Variable nonhemolytic hemolytic Glycogen/ starch fermentation Positive Negative Negative
- 15. OTHER FEATURES OF VARIOUS BIOTYPES • The gravis and mitis are associated with high case fatality rates; • Paralytic complications more with gravis; • Hemorrhagic complications –gravis and intermdius; • Obstruction to air passage - mitis • mitis – endemic ; gravis and intermedius- epidemic
- 16. BIOCHEMICAL REACTIONS • Hiss serum sugars – for testing fermentation reactions; • Ferment- glucose, galactose, maltose and dextrose; but not lactose, sucrose, mannitol; • Proteolytic activity is absent; • Do not hydrolyse urea; • Do not form phosphatase; • Produce cystinase (halo on Tinsdale’s medium)
- 17. RESISTANCE • Cultures remain viable for 2-3 wks at 25-300C • Destroyed by heat • Resistant to light, desiccation or freezing; • Easily destroyed by antiseptics • Susceptible to – Penicillin, erythromycin and broad spectrum antibiotics;
- 18. ANTIGENIC STRUCTURE AND TYPING • Serotyping : Antigenically heterogenous – gravis: 13 types – intermedius : 4 types – mitis : 40 types • Bacteriophage typing : 15 types • Bacteriocin typing : diphtheriocin typing
- 19. VIRULENCE FACTORS • Virulent strains of diphtheria bacilli produce a very powerful exotoxin. • The ‘virulence’ of diphtheria bacilli is due to their capacity to- – Establish infection and growing rapidly – Quickly elaborate an exotoxin • Avirulent strains are common among convalescents , contacts and carriers, particularly those with extra-faucial infection
- 20. DIPHTHERIA TOXIN • The pathognomonic effects are due to the toxin; • Almost all the gravis and intermedius strains and 80-85% of mitis strains are toxigenic • Toxin is a protein; • Mol. Wt.: 62,000 • Two fragments, A and B; • Extremely potent : – 0.1 μg lethal to guinea pig • Inactive when released
- 21. Toxin – mechanism of action • Fragment B : binds to a cell surface receptor and helps in transport of toxin into the cell; • After entering the cell, A subunit is released ; • A subunit catalyses the transfer of ‘adenosine diphosphate ribose (ADPR)’ from NAD+ • ADPR binds with the elongation factor EF 2 • “ADPR-EF2” complex is inactive protein synthesis stops abruptly necrotising and neurotoxic effects of the toxin;
- 23. PATHOGENICITY • Commonest site of infection: Upper respiratory tract (fauces, larynx,nose) • Ocassionally, other cutaneous or mucocutaneous areas ( otitic/conjunctival/ genitovulval/vaginal/ prepucial/skin) • Faucial diphtheria is the commonest type; • Sore throat is frequently the presenting symptom;
- 24. PATHOLOGY • After infection, the bacilli multiply on the mucous membrane or skin abrasion; • The toxigenic strains start producing toxin; • Diphtheria is a ‘toxemia’; • The bacteria confine to the site of entry but the exotoxin is absorbed into the mucus membrane and causes destruction of epithelium and a superficial inflammatory response;
- 25. PATHOLOGY • The toxin causes local necrotic changes; • The resulting fibrinous exudate, together with the epithelial cells, leucocytes, erythrocytes and bacteria constitute : “pseudomembrane” • Any effort to remove it will tear off capillaries beneath it and cause bleeding; • Mechanical complications are due to pseudomembrane and systemic effects are due to the toxin;
- 26. Toxin-systemic absorption • The bacilli continue to produce the toxin; • The toxin is absorbed systemically and damages heart muscle, liver, adrenals etc.; • The toxin also cause nerve damage, especially of soft palate(palatine) and eye muscles (ciliary); • Toxin absorption is negligible in case of skin infection with toxigenic strains; • Nontoxigenic strains can also produce local disease but systemic effects are absent;
- 27. CLINICAL DISEASES • Incubation period : usually 3-4 days; • Acute infection : in the form of – – Membranous tonsillitis – Nasal infection – Laryngeal infection – Skin infection –uncommon;
- 28. CLINICAL DISEASES • Characteristic feature is : ‘wash –leather’ eleveted greyish greeen membrane in the tonsils with a well defined edge surrounded by a zone of inflammation;
- 29. ‘wash –leather’ eleveted greyish greeen membrane in the tonsils Pseudomembrane
- 30. CLASSIFICATION BASED ON CLINICAL SEVERITY • Malignant or hypertoxic: – ‘Bull neck’ due to marked adenitis in neck; – Severe toxemia – Circulatory failure – Death – Paralytic squealae in survivors • Septic : ulceration, cellulitis and gangrene around pseudomembrane; • Hemorrhagic: bleeding from the edge of pseudomembrane, epistaxis, purpura etc.
- 31. Bull neck : due to cervical adenitis and edema of neck
- 32. COMPLICATIONS • Asphyxia : due to mechanical obstruction Emergency tracheostomy may be necessary; • Acute circulatory failure • Myocarditis • Postdiphtheritic paralysis- palatine(soft palate) and ciliary ( eye muscles) nerves Recovery – spontaneous and complete • Septic : pneumonia and otitis media • Relapse : in about 1% of cases
- 33. LABORATORY DIAGNOSIS • This is to confirm the clinical impression and for epidemiological purpose; • Specific treatment must never be delayed for laboratory reports, if the clinical picture is strongly suggestive of diphtheria; • Any delay may be fatal…! • Laboratory diagnosis consists of the isolation of the organism and demonstration of it’s toxicity;
- 34. LABORATORY DIAGNOSIS • Specimens : – Swabs from – nose, throat or other suspected lesions; • Smear examination: Gram stain – shows beaded rods in typical arrangement; – Difficult to differentiate from some commensal corynebacteria normally found in throat; – Albert’s stain or Neisser’s stain is useful for demonstrating the granules;
- 35. Numbers of large-sized Gram-positive rods are embedded within the pseudomembrane (Gram). LABORATORY DIAGNOSIS
- 36. LABORATORY DIAGNOSIS : CULTURE • If the swabs can not be inoculated promptly, they should be kept moistened with serum; • Inoculate on : – Loeffler’s serum slope – Tellurite blood agar or Tinsdale medium – Blood agar ( for differentiating Staphylococcal or Streptococcal pharyngitis that simulate diphtheria); • Tellurite medium is particulary useful for isolating the organism from – convalescents, contacts or carriers;
- 37. LABORATORY DIAGNOSIS : CULTURE • Processing : – Serum slope may show growth in 4-8 hrs but if negative may need to be incubated for 24 hrs; – Smear may show ‘diphtheria-like’ organisms; – By about 48 hrs, Tellurite plates will yield growth; – The isolate must be submitted for – ‘Virulence tests’ or ‘Toxigenicity tests’ before the bacteriological diagnosis is complete;
- 38. VIRULENCE TESTS • In vivo methods: – Subcutaneous test – Intracutaneous test • In vitro methods: – Elek’s gel precipitation test – Tissue culture test
- 39. SUBCUTANEOUS TEST Emulsify the growth form an overnight culture of Loeffler’s serum slope in 2-4 ml broth 0.8 ml injected subcutaneously Into two guinea pigs Protected with 500 IU of antitoxin 18-24 hrs previously Unprotected Die in 4 days if the strain is Virulent; autopsy shows Characteristic features Remain healthy Disadvantage : Death of the animal Control animal Test animal
- 40. INTRACUTANEOUS TEST 0.1 ml of emulsion broth inoculated intracutaneously in to two guinea pigs Control animal Test animal Should receive 500 IU Of antitoxin previous day Give 50 IU of antitoxin Intraperitoneally 4 hrs after skin test (To prevent death) Inflammatory reaction Progress to necrosis in 48-72 hrs NO CHANGE
- 41. INTRACUTANEOUS TEST • Animal does not die; • Rabbits may also be used; • As many as 10 strains can be tested simultaneously;
- 42. Elek’s gel precipitation test • In vitro test; • A rectangular strip of filter paper is saturated with the diphtheria antitoxin(1000 units/ml); • This strip is placed on : agar plate with 20% horse serum, while the medium is setting; • The cultures to be tested are streaked at right angles to the filter paper strip; • A positive and negative control should be put;
- 43. Incubate the plate for 24-48 hrs at 370C P T N
- 44. After incubation – line of precipitation can be observed Where the toxin and antitoxin meet at optimum conc. The lines of precipitation will indicate that the test strain is toxigenic P T N
- 45. Tissue culture test • Bacteria incorporated into an agar overlay of cell culture monolayers; • The toxin, if produced, diffuses into the cells below and kills them;
- 46. EPIDEMIOLOGY • Mainly a disease of childhood(pediatrics) in endemic areas – uncommon below 1st year; peaks at 5. • In nature, C.diphtheriae occurs in the respiratory tract, in the wounds or in the skin of the infected persons or carriers; • Transmission is by- – Droplet dissemination from cases or carriers – Direct contact – Occasionally, fomites; • Nasopharyngeal or cutaneous carriage of toxigenic or nontoxigenic strains can persist for life in healthy people;
- 47. PROPHYLAXIS • Diphtheria can be controlled by immunisation; • Types of immunisation available for diphtheria: – Active – Passive – combined • The objective of immunisation is to increase protective levels of antitoxin in circulation;
- 48. Active immunisation • Emil von Behring initiated immunisation for diphtheria in children in 1913 using toxin –antitoxin mixtures; (TAT) • These preparations were hazardous; • Danysz phenomenon: if the equivalent amounts of toxin and antitoxin were mixed all at once, the final preperation was nontoxic. But, if the same amount of toxin was added in instalments, the resultant mixture was toxic; • In 1929, Ramon introduced ‘toxoid’.
- 49. Active immunisation - toxoids • Two preparations of toxoid are available: – Formol toxoid – Adsorbed toxoid • Formal toxoid : prepared by incubating the toxin with formalin for 3-4 weeks; • Adsorbed toxoid : purified toxoid is adsorbed onto an adjuvant, either aluminium phosphate or aluminium hydroxide; this is more immunogenic;
- 50. Active immunisation - toxoids • Adsorbed toxoid –given as IM injections • Recommended vaccines: – As a trivalent preperation : DPT (adsorbed Diphtheria/Pertusis/Tetanus) – Adsorbed Diphtheria/Tetanus (DT) – Adsorbed low dose diphtheria vaccine for adults (d) – Adsorbed Tetanus/low dose diphtheria vaccine(Td) for adults; – A quadraple vaccine containing DPT+inactivated polio vaccine is also available;
- 51. Active immunisation- schedules • Primary immunisation: – 3 doses of DPT begening at 4th week of age, 8th and 12th week under Routine Immunization schedule(Govt. of Tanzania) • Booster (DPT) at 15-18 months of age; – Further booster, as ‘DT’ at – 5 years of age; • Dosage : 0.5 ml – 10-25 Lf units of toxoid - recommended for children
- 52. Active immunisation- schedules • Contraindications: – Acute febrile illness : postpone till recovery – Severe local or systemic reaction to pertusis component of DPT are likely; if they occur, immunise with DT; acellular pertusis vaccine can be added if the reaction is a local one;
- 53. Passive Immunisation • Using antitoxin or ADS(Antidiphtheritic serum); • As an emergency measure when susceptibles are exposed to infection; • Subcutaneous administration of 500-1000 units of antitoxin or ADS(Antidiphtheritic serum); • Risk of hypersensitivity as horse serum used; Historical engraving showing how the medicinal serum was obtained from immunized horses.
- 54. Combined immunisation • Administration of first dose of toxoid on one arm, while ADS is given on the other arm, to be continued by full course of active immunisation; • All cases that received prophylactic ADS should receive combined immunisation;
- 55. TREATMENT • Specific measure : prompt administration of antitoxin to neutralize the circulating toxin; – Dose: 20,000-1,00,000 units – Half the dose given IV – Antitoxin treatment is generally not indicated for cutaneous diphtheria • Antibiotics : Penicillin or Erythromycin for 14 days; • Complete bed rest; • Supportive therapy and treatment of complications • Erythromycin: for treatment of carriers.
- 57. C.ULCERANS –Resembles gravis biotype of C.diphtheriae –Liquify gelatin, ferment trehalose slowly, does not reduce nitrates; –Produce two types of toxins; –Guinea pigs: lesions similar to those of C.diphtheirae; –Cause infection in cows; –Human infections may be transmitted through cow’s milk; –Diphtheria antitoxin is protective;
- 58. OTHER CORYNEBACTERIA • Arcanobacterium(C.hemolyticum): – pharyngitis and skin ulcers • C.jakeium: – cutaneous and blood stream infections in immunocompromised; multi resistant; • C.pseudotuberculosis: Preisz Nocord bacillus – Pseudotubeculosis in sheep and lymphadenitis in horses; • C.minutissimum: – Erythrasma, affecting axilla and groin • C.tenuis: pigmented nodules around axillary and pubic hair shafts. • C.parvum: an immunomodulator agent
- 59. DIPHTHEROIDS • Resemble C.diphtheriae and mistaken for them; • Common commensals of nose, throat, nasopharynx, skin, urinary tract and conjunctiva • Produce no exotoxin; • Stain more uniformly, few or no metachromatic granules and tend to be arranged in palisades; • Can produce disease in immunocompromised; • Have been isolated in infections such as endocarditis of prosthetic valves, lung abscess and UTI; • Sensitive to Vancomycin; • Ex. C.pseudodiphtheriticum – throat • C.xerosus : conjunctival sac