1. Section II – Chest Radiology
Figure 1A
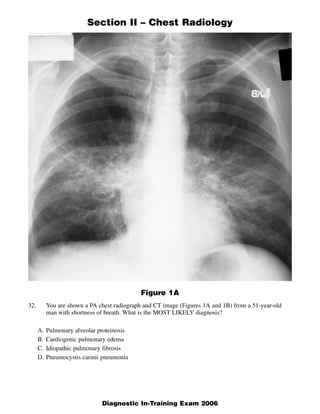
32. You are shown a PA chest radiograph and CT image (Figures 1A and 1B) from a 51-year-old
man with shortness of breath. What is the MOST LIKELY diagnosis?
A. Pulmonary alveolar proteinosis
B. Cardiogenic pulmonary edema
C. Idiopathic pulmonary fibrosis
D. Pneumocystis carinii pneumonia
1
Diagnostic In-Training Exam 2006
2. Section II – Chest Radiology
Figure 1B
2 American College of Radiology
3. Section II – Chest Radiology
Question #32
Findings: Chest radiograph demonstrates bilateral perihilar opacities. High resolution CT scan demon-
strates bilateral thin walled cysts, ground glass and reticular opacities
Rationales:
A. Incorrect. The most common radiographic manifestation of pulmonary alveolar proteinosis is
ground glass and air space opacities which are located in a perihilar distribution such as in this case.
The presence of ground glass opacities on the CT scan is consistent with pulmonary alveolar pro-
teinosis. However, septal thickening is not prominent. The combination of ground glass opacities
and septal thickening is sometimes referred to “crazy paving,” an appearance most commonly seen
in pulmonary alveolar proteinosis. The CT also demonstrates the presence of multiple relatively thin
walled cysts. Such cysts are not a feature of pulmonary alveolar proteinosis.
B. Incorrect. Although the standard radiograph is somewhat suggestive of the “butterfly” or “bats
wing” pattern identified in cardiogenic pulmonary edema, the heart is not enlarged and there is no
evidence of Kerley B lines or pleural effusions. Multiple thin walled cysts are not a feature of con-
gestive heart failure.
C. Incorrect. IPF occurs in patients between 50 and 70 years old. Radiographic findings include reticu-
lar opacities in the peripheral distribution at the lung bases. Thus, the presence of perihilar disease
in our case along with absence of disease in the subpleural basilar location lead us away from the
diagnosis.
D. Correct. In patients with PCP, the chest radiograph classically demonstrates bilateral often perihilar
reticular and ground glass opacification which may eventually become confluent and produce air
space consolidation within several days. Cysts are visible on chest radiographs in 10% of patients
although they are appreciated far more commonly on HRCT scans (33%). Cysts may occur in the
acute or post infective period and range in number, size, shape and distribution. They are commonly
multiple and have a predilection for the upper lobes. Spontaneous pneumothorax may be a feature
of PCP infection and occurs in approximately 35% of patients with cysts.
3
Diagnostic In-Training Exam 2006
4. Section II – Chest Radiology
Figure 2A
33. You are shown two images from a high-resolution CT (Figures 2A and 2B) of the chest of a 40-
year-old female smoker with a 1-year history of increasing shortness of breath. What is the
MOST LIKELY diagnosis?
A. Centrilobular emphysema
B. Lymphangioleiomyomatosis
C. Langerhans cell histiocytosis
D. Lymphocytic interstitial pneumonia
4 American College of Radiology
6. Section II – Chest Radiology
Question #33
Findings: Diffuse cystic lung disease. Lungs are uniformly involved with no evidence of architectural
distortion.
Rationales:
A. Incorrect. Centrilobular emphysema which occurs in smokers is recognized by the presence of mul-
tiple lucencies which are predominant in the upper lobes. Characteristically these areas of centrilob-
ular emphysema do not have well defined walls and therefore can be differentiated from cysts.
Upper lobe predominance is a key feature and differs from the test case in which there is diffuse
involvement.
B. Correct. Lymphangioleiomyomatosis. This disease occurs in young to middle-aged women of
reproductive age. It is characterized by the presence of cysts with well-defined thin walls measuring
1-2 mm in diameter. The distribution is usually diffuse and other features of interstitial lung disease
or fibrosis are notably absent, i.e. reticulation, small nodules, honeycombing and traction bronchiec-
tasis. There is no evidence of architectural distortion.
C. Incorrect. Langerhans cell histiocytosis does occur in smokers but is characterized by a number of
different features. Nodules up to 1 cm in diameter are common. These nodules frequently cavitate
and in the end state of the disease a cystic pattern can be noted. However, a purely cystic pattern is
extremely unusual. Upper lobe involvement predominates, and the bases, particularly the
costophrenic angles are free of disease, a feature which is not present in the test case.
D. Incorrect. CT features of lymphoid interstitial pneumonia include ground glass attenuation, cen-
trilobular and subpleural lung nodules with thickening of the interlobular septa and peribronchovas-
cular interstitium. Perivascular cysts are seen in a minority of cases. Most of these CT features are
not present in the test case. The cysts are diffuse and not perivascular in location.
6 American College of Radiology
7. Section II – Chest Radiology
Figure 3A
Figure 3B
7 American College of Radiology
8. Section II – Chest Radiology
Figure 3C
34. You are shown three CT images (Figures 3A, 3B, and 3C) of a 59-year-old man with cough and
stridor. What is the MOST LIKELY diagnosis?
A. Squamous cell papilloma
B. Carcinoid
C. Adenoid cystic carcinoma
D. Tracheobronchopathia osteochondroplastica
8
Diagnostic In-Training Exam 2006
9. Section II – Chest Radiology
Question #34
Findings: Irregular soft tissue mass with diffuse infiltration of the tracheal wall extending into the
bronchial walls of the right lung (better seen on lung windows). This irregular mass is associated with
lymphadenopathy and infiltration of adjacent mediastinal fat.
Rationales:
A. Incorrect. The most common benign tracheal tumor, this lesion usually manifests as a smooth, well-
circumscribed, soft tissue lesion measuring less than 2 cm. This would not be an appropriate choice
for this irregular mass with extension along the tracheobronchial tree with lymphadenopathy.
B. Incorrect. These also tend to be well-defined, smooth, round lesions. Carcinoid tumors arise from
neuroendocrine cells and may calcify. They may enhance vigorously with intravenous contrast. The
lack of enhancement and diffuse infiltration of the tracheobronchial walls make carcinoid tumor
highly unlikely.
C. Correct. Adenoid cystic tumors represent the most common salivary gland tumor of the trachea.
These lesions tend to grow slowly and spread submucosally. Formerly known as cylindromas
because of their tendency to create castes of the tracheal tree, adenoid cystic carcinomas have been
reclassified so as not to be confused with benign disease. Treatment is surgical resection which can
be challenging because of this tumor’s tendency to spread perineurally and escape radiologic detec-
tion.
D. Incorrect. Though the imaging might suggest an inflammatory or infectious tracheal process
because of the long-segment of airway involvement, tracheobronchopathia osteochondroplastica
(TOP) would not be a likely diagnosis here. The lack of calcification and preferential involvement
of the posterior membrane would not allow for TOP to be the preferred diagnosis.
9 American College of Radiology
10. Section II – Chest Radiology
Figure 4
35. You are shown a CT image (Figure 4) of a 63-year-old man who underwent heart transplantation
for ischemic cardiomyopathy two years ago. What is the MOST LIKELY diagnosis?
A. Bronchiolitis obliterans
B. Post-transplant lymphoproliferative disease
C. Cryptogenic organizing pneumonia
D. Bronchogenic carcinoma
10 American College of Radiology
11. Section II – Chest Radiology
Question #35
Rationales:
A. Incorrect. More commonly seen after lung transplantation, bronchiolitis obliterans usually is radi-
ographically occult. When it is seen, it may be seen as areas of air-trapping or mosaic attenuation.
Other reported findings include bronchiectasis and septal line thickening. Solitary nodule is not a
finding of bronchiolitis obliterans.
B. Incorrect. Post-transplant lymphoproliferative disease (PTLD) (after infection) is one of the most
common explanations for a solitary pulmonary nodule in the post-transplanted patient. The imaging
features include one or more smooth nodules or areas of consolidation with air bronchograms. A
single, spiculated nodule would be an unusual manifestation of PTLD.
C. Incorrect. Cryptogenic organizing pneumonia (CPO) is another finding that may be encountered in
the post-transplant patient. COP may present with peripheral consolidations (similar to chronic
eosinophilic pneumonia) or may present in a nodular form. The nodular form tends to have air bron-
chograms. A solitary nodule with spiculation would be highly unlikely for COP. In fact, a biopsy of
this nodule would likely be repeated if COP was the pathologic diagnosis, in order to exclude inade-
quate sampling as biopsy of the area adjacent to a neoplasm will result in a pathologic diagnosis of
COP.
D. Correct. As transplant patients are living longer, it has become well-accepted that transplant
immunosuppression results in an increased risk of solid-organ tumors, especially in smokers. In this
patient, smoking had contributed to his ischemic cardiomyopathy. Radiologic features of these neo-
plasms are similar to the features in a non-transplant patient. If this CT were reviewed without the
transplant history, bronchogenic neoplasm would lead the differential diagnosis. This lesion was
biopsied and this suspicion was confirmed.
11
Diagnostic In-Training Exam 2006
12. Section II – Chest Radiology
Figure 5A
Figure 5B
36. You are shown a CT image (Figure 5A) and two images from an F-18 FDG (fluorodeoxyglu-
cose) PET scan (Figure 5B) of a 71-year-old man. What is the MOST LIKELY diagnosis?
A. Benign nodule
B. Stage I lung cancer
C. Stage II lung cancer
D. Stage IV lung cancer
12 American College of Radiology
13. Section II – Chest Radiology
Question #36
Findings: A small irregularly marginated uncalcified nodule on CT shows intense activity on FDG PET
scan. In addition, there is a large focus of intense activity in the region of the right adrenal gland.
Rationales:
A. Incorrect. Benign nodules may show uptake on FDG PET scan, but rarely this intense. Benign etiol-
ogy does not explain adrenal activity.
B. Incorrect. Without the adrenal activity, this would be typical of Stage I lung cancer.
C. Incorrect. There is no adjacent nodal activity to suggest T1or2 N1 disease.
D. Correct. The adrenal gland is one of the most common sites of metastasis from bronchogenic carci-
noma and may be seen in otherwise Stage I disease. This tumor is T1N0M1 or Stage IV.
13
Diagnostic In-Training Exam 2006
14. Section II – Chest Radiology
Figure 6
37. You are shown a PA chest radiograph (Figure 6) of a 54-year-old woman with shortness of
breath and cough. What is the MOST LIKELY diagnosis?
A. Miliary tuberculosis
B. Pulmonary alveolar microlithiasis
C. Lymphangitic carcinomatosis
D. Idiopathic pulmonary hemosiderosis
14 American College of Radiology
15. Section II – Chest Radiology
Question #37
Rationales:
A. Incorrect. Miliary TB represents diffuse hematogenous spread of the tuberculin bacillus throughout
the lungs. The radiographic appearance is that of tiny 1-2 mm nodules throughout the lungs. Our
case has much more numerous micronodules than seen in miliary TB.
B. Correct. Correct. Pulmonary alveolar microlithiasis (PAM) is a rare condition of uncertain etiology.
The chest radiograph shows numerous very fine micronodules throughout both lungs, more so in the
middle and lower lung zones. The radiographic findings have been described as that of a sand-storm
like appearance. Our case has classic features seen in PAM.
C. Incorrect. Lymphangitic carcinomatosis is characterized by metastatic tumor involvement of the
lymphatic system. The typical chest radiographic findings include reticulonodular or linear opaci-
ties, septal lines and mediastinal or hilar adenopathy. These features are absent in our case.
D. Incorrect. Idiopathic pulmonary hemosiderosis is a rare disease of unknown etiology. It most com-
monly occurs in children in their first decade of life. It is seen as diffuse airspace opacities follow-
ing an episode of acute hemorrhage. As the blood products break down, there is deposition of
hemosiderin into the pulmonary interstitium and lymphatics. Thus, the radiographic findings follow-
ing repeated bouts of bleeding appear as a reticular pattern. These features are absent in our case.
15
Diagnostic In-Training Exam 2006
16. Section II – Chest Radiology
38. For which of the following is obtaining a definitive diagnosis with needle biopsy MOST
DIFFICULT?
A. Hamartoma
B. Healed granuloma
C. Lymphoma
D. Metastatic carcinoma
Question #38
Rationales:
A, C and D are Incorrect.
B is Correct. Percutaneous needle biopsy is most commonly used to biopsy intrathoracic or parenchy-
mal lesions. Either 22Gauge needles or 20 Gauge core biopsy needles are utilized. Percutaneous needle
biopsy is most commonly used to establish a diagnosis of malignancy. The sensitivity for diagnosis of
malignancy (primary and metastatic) is about 85 – 95%. Diagnosis of Lymphoma and Hamartoma is a
little more difficult and sensitivity is in the range of 50 – 65%. However, histologic diagnosis of benign
lesions such as granuloma is far more difficult. In general, granulomas that are active can be diagnosed
by needle biopsy by demonstrating a positive culture. However, healed granulomas contain necrotic
material and far fewer inflammatory cells. Thus, scant cellularity and minimal number of organisms in
a healed granuloma result in far fewer definitive diagnoses than Lymphoma, Hamartoma and
Metastasis.
16 American College of Radiology
17. Section II – Chest Radiology
39. Which one of the following is MOST frequently involved in fibrosing mediastinitis?
A. Pulmonary artery
B. Aorta
C. Left common carotid artery
D. Bronchial artery
Question #39
Rationales:
A is Correct. Fibrosing mediastinitis is a rare disorder characterized by chronic inflammation and
fibrosis of mediastinal soft tissues. There are many causes of fibrosing mediastinitis. The most frequent-
ly implicated process is infection, of which Histoplasma capsulatum is the most common cause.
Complications of fibrosis within the mediastinum lead to encasement and compression of mediastinal
structures. Those that are particularly involved include superior vena cava, trachea and bronchi, and pul-
monary artery and veins. Aorta and great vessel involvement is extremely rare.
B, C and D are Incorrect.
17
Diagnostic In-Training Exam 2006
18. Section II – Chest Radiology
40. Concerning inverse square law in chest fluoroscopy, if the patient’s entrance dose is 20 mGy/min with
the source-to-skin distance (SSD) of 65 cm and source-to-image distance (SID) of 90 cm. How much
does the entrance dose change if the SID is increased to 120 cm while maintaining similar SSD?
A. Increases by a factor of approximately 1.3
B. Remains unchanged
C. Decreases by a factor of approximately 2
D. Increases by a factor of approximately 1.8
Question #40
Rationales:
A. Incorrect. See correct answer.
B. Incorrect. See correct answer.
C. Incorrect. See correct answer.
D. Correct. According to the inverse square law, if the exposure-rate from a source is X1 at distance
d1, the exposure rate X2 at another distance d2 will be X2=X1(d1/d2)2. Therefore, Increasing the SID
requires an increased output from the X-ray tube. Using the inverse square law, you have two equa-
tions, (Xpatient90/X90)=(d90/d65)2 and (Xpatient120/X120)=(d120/d65)2. A constant dose rate is necessary
at the image intensifier at any SID since auto brightness control is being used so X90=X120. So when
you plug this into the equations and rearrange, you get (Xpatient120/Xpatient90)=(120/90)2 ≈ 1.8.
18 American College of Radiology
19. Section II – Chest Radiology
41. Which one of the following is MOST LIKELY to be associated with small cell carcinoma?
A. Brachial plexopathy
B. Hypoglycemia
C. Hyponatremia
D. Pupillary constriction
Question #41
Rationales:
A, B and D are Incorrect.
C is Correct. Small cell carcinoma is a form of lung cancer. It accounts for 15 – 20% of all lung can-
cers. It is characterized by rapid growth, early metastasis and extremely poor prognosis. It is associated
with paraneoplastic syndromes, including Cushing’s syndrome and inappropriate ADH secretion.
Inappropriate ADH secretion results in hyponatremia. Hypoglycemia, Brachial plexopathy and pupillary
constriction are not clinical features of small cell carcinoma. The most common tumor responsible for
hypoglycemia in the thorax is Solitary fibrous tumor of the pleura. Brachial plexopathy and pupillary
constriction are more likely to occur with superior sulcus tumor.
19
Diagnostic In-Training Exam 2006
20. Section II – Chest Radiology
42. Concerning pulmonary veno-occlusive disease, which of the following are characteristic
CT findings?
A. Enlarged left atrium and diffuse interstitial edema
B. Enlarged left atrium and normal lung parenchyma
C. Normal-sized left atrium and normal lung parenchyma
D. Normal-sized left atrium and diffuse interstitial edema
Question #42
Rationales:
A, B and C are Incorrect.
D is Correct. Pulmonary venoocclusive disorder is a rare disorder characterized by obliteration of
small pulmonary veins. This leads to pulmonary hypertension. The causes are many and include viral
infections, inhaled toxins and immune complex deposition within the lung to name a few. Diagnosis is
suggested in a patient with pulmonary hypertension when radiographic features demonstrate enlarged
pulmonary arteries, diffuse interstitial edema and small to normal sized left atrium.
20 American College of Radiology
21. Section II – Chest Radiology
Kerley B lines represent which one of the following?
43.
A. Dilated peripheral pulmonary veins
B. Distended capillaries
C. Distended lymphatics
D. Thickened interlobular septa
Question #43
Rationales:
A, B and C are Incorrect.
D is Correct. Kerley B lines are short horizontal lines that are visible on chest radiograph adjacent to
the costophrenic sulcus. They are approximately 1 to 2 cm long and are noted to extend to the pleural
surface. They represent thickened interlobular septa and are visible in patients with lymphangitic carci-
nomatosis and pulmonary edema.
21
Diagnostic In-Training Exam 2006
22. Section II – Chest Radiology
Which one of the following injuries is indicated by the dependent viscera sign?
44.
A. Bronchial fracture
B. Diaphragmatic rupture
C. Pulmonary laceration
D. Traumatic aortic tear
Question #44
Rationales:
A. Incorrect
B. Correct. Tear in the diaphragm results in herniation of viscera (bowel and solid organs) into the
thoracic cavity. As the injured diaphragm no longer supports these structures posteriorly, they fall to
a dependent position against the posterior ribs. Hence, the dependent viscera sign is observed in
patients with diaphragmatic injury when they lie supine for a CT scan.
C. Incorrect
D. Incorrect
22 American College of Radiology
23. Section II – Chest Radiology
Which one of the following entities can be expected to cause a pneumothorax?
45.
A. Boerhaave’s syndrome
B. Desquamative interstitial pneumonia
C. Metastatic osteogenic sarcoma
D. Ruptured bronchus within 1 cm of the carina
Question #45
Rationales:
A. Incorrect. Boerhaave’s syndrome represents perforation of esophagus following severe episodes of
vomiting. In this instance, pneumomediastinum rather than pneumothorax is the expected conse-
quence.
B. Incorrect. Recurrent pneumothorax may be associated with chronic infiltrative lung disease of any
cause, but the prevalence is particularly high in two diseases; Langerhans cell histiocytosis (histio-
cytosis x) and lymphangioleiomyomatosis. Both of these entities are characterized by the presence
of multiple lung cysts which may rupture through the visceral pleura causing a complicating pneu-
mothorax. However, pneumothorax may be seen as a complication of the late stages of other types
of infiltrative lung diseases that are associated with fibrosis and honeycombing. Desquamative inter-
stitial pneumonia is not characterized by the presence of cysts. High resolution CT frequently
demonstrates ground glass and alveolar opacities more marked in the mid and lower lung zones.
Fibrosis and honeycombing are not features and the disease responds to steroid therapy.
C. Correct. Malignant neoplasms, particularly metastatic sarcoma, are occasional causes of sponta-
neous pneumothorax. The most common tumor type is metastatic osteogenic sarcoma. The mecha-
nism for the development of pneumothorax is not clear, but it may be related to the presence of cav-
itation and subsequent rupture into the pleural space. The presence of a “spontaneous” pneumotho-
rax in a child in the setting of a primary osteogenic sarcoma should prompt a CT examination to
search for the presence of metastatic disease.
D. Incorrect. Pneumothorax which is unresponsive to chest tube drainage can be a feature of a ruptured
bronchus which is sustained following blunt trauma usually in high speed motor vehicle accidents.
However, the rupture must occur at a site in the bronchus which is contained within the mediastinal
pleura. Thus tears close to the carina produce pneumomediastinum rather than pneumothorax.
23
Diagnostic In-Training Exam 2006
24. Section II – Chest Radiology
46. Concerning cystic fibrosis, which one is TRUE?
A. Bronchiectasis is more severe in the lower lobes.
B. Sodium and chloride levels are elevated in the sweat.
C. It is heritable by dominant transmission.
D. The lung volumes are small.
Question #46
Rationales:
A. Incorrect. Bronchiectasis-- identified as parallel lines or as ring shadows larger than the accompany-
ing pulmonary artery—usually is widespread on radiographs but tends to affect mainly the upper
lobes.
B. Correct. True statement. The Sweat Test is one of the ways that diagnosis of Cystic fibrosis is
made.
C. Incorrect. Cystic fibrosis is a relatively common hereditary disorder of recessive transmission. The
disease is the most common lethal genetically transmitted disease among whites with an estimated
incidence in this group of 1 per 2,000 to 3,000 live births.
D. Incorrect. Hyperinflation is seen in about 80% of adult patients and tends to involve mainly the
lower lobes.
24 American College of Radiology
25. Section II – Chest Radiology
Concerning solitary pulmonary nodules, which one is TRUE?
47.
A. Considered benign if stable for 1 year
B. Defined as a lesion that measures less than 2 cm
C. Metastasis is the most common cause
D. Presence of fat is indicative of benign etiology
Question #47
Rationales:
A, B and C are Incorrect.
D is correct. Solitary pulmonary nodule is defined as a well circumscribed round or oval lesion meas-
uring less than 3 cm in diameter. About half of the lesion are proven to be benign, about 40% are
proven to be primary lung carcinoma and only about 10% are proven to be metastasis. A number of cri-
teria have been described to help differentiate benign from malignant nodules. However, none have
proven to be of very specific except presence of fat is suggestive of a benign lesion. Also, benign
lesions have a doubling time of less than 1 month or greater than 16 months. Thus, nodules that are sta-
ble for over a 2 year period are considered benign.
25
Diagnostic In-Training Exam 2006
26. Section II – Chest Radiology
48. A film cassette spot film is taken of the chest of a supine patient with an under-table tube on a
fluoroscopic system. How does the spot film image taken with an under-table fluoroscopy sys-
tem differ from a typical properly exposed PA chest radiography film performed using an
upright Bucky with similar kVp and cassette?
A. The spot film will have significantly lower noise.
B. The longer exposure time will cause increased cardiac motion blurring for the spot film image.
C. A larger difference in image size is seen between anterior and posterior structures in spot
film image.
D. The spot film yields lower entrance dose to patient.
Question #48
Rationales:
A. Incorrect. Since both films are properly exposed and are using the same cassette, equivalent number
of photons will be absorbed to produce the images, and they should have equivalent levels of noise.
B. Incorrect. The exposure time for the spot film should be shorter due to the shorter source-film dis-
tance.
C. Correct. The shorter source-to-image distance with the fluoroscopic system will result in a wider
beam divergence, and a larger difference in image magnification of structures on the posterior side
of the patient versus the anterior side.
D. Incorrect. Because of the shorter source-to-image distance, the entrance dose for spot film will be
greater than chest radiography.
26 American College of Radiology
27. Section II – Chest Radiology
49. Which finding is characteristic of sarcoidosis?
A. Anterior mediastinal adenopathy
B. Basilar reticular opacities
C. Peribronchovascular nodules
D. Random nodules
Question #49
Rationales:
A. Incorrect. Bilateral hilar and right paratracheal adenopathy is common. Anterior mediastinal
adenopathy / mass usually signify Lymphoma or Thymoma.
B. Incorrect. The disease in sarcoidosis tends to be predominantly upper lobe in distribution.
C. Correct. Peribronchovascular or perilymphatic nodules are typically seen in patients with sarcoido-
sis. Nodules in sarcoidosis are also noted in the subpleural location and along the interlobular septa.
D. Incorrect. Random nodules usually represent hematogenous metastasis or miliary infection, such as
Tuberculosis.
27
Diagnostic In-Training Exam 2006
28. Section II – Chest Radiology
50. Concerning the left superior vena cava, how does it communicate with the heart?
A. Enters the left atrium via the pulmonary veins
B. Enters the left atrium via the coronary sinus
C. Enters the right atrium via the sinus of Valsalva
D. Enters the right atrium via the coronary sinus
Question #50
Rationales:
A. Incorrect.
B. Incorrect. The left superior vena cava drains into the right atrium via the coronary sinus.
C. Incorrect. The sinus of Valsalva is at the root of the aorta.
D. Correct. The left superior vena cava (SVC) drains into the right atrium via the coronary sinus. A
left-sided SVC, a normal anatomic variant, is found in 0.3% of normal individuals. 80% of such
individuals also have a right-sided SVC and 60% have a left BCV connecting to the right and left
SVCs.
28 American College of Radiology
29. Section II – Chest Radiology
Concerning eosinophilic lung disease, which one is TRUE?
51.
A. Blood eosinophilia is necessary to make the diagnosis.
B. It can be caused by drugs, such as sulfonamides.
C. Chronic eosinophilic pneumonia is characterized by central opacities.
D. Loffler’s syndrome is characterized by peripheral opacities.
Question #51
Rationales: B & D ARE BOTH CORRECT
A. Incorrect. Blood eosinophilia is not necessary to make the diagnosis of eosinophilic lung disease.
The term pulmonary eosinophilia, synonymous with pulmonary infiltration with eosinophilia,
describes a group of diseases in which blood and/or tissue eosinophilia affects major airways and
lung parenchyma.
B. Correct. True statement. Eosinophilic lung diseases are a group of pulmonary disorders that are
characterized by abundant eosinophils in the pulmonary opacities. They are classified into groups
with and without a specific cause. The specific causes include drugs, such as sulfonamides, para-
sites, and fungi.
C. Incorrect. Chronic eosinophilic pneumonia has classic radiographic and chest CT findings of
peripheral, nonsegmental, homogenous alveolar opacities, often with air bronchograms.
D. Correct. Loffler’s syndrome is characterized by blood eosinophilia, absence of or mild symptoms
and signs (cough, fever, and dyspnea), one or more nonsegmental mixed interstitial and alveolar
pulmonary opacities that are transitory or migratory, and spontaneous clearing of the opacities.
29
Diagnostic In-Training Exam 2006
30. Section II – Chest Radiology
Which one of the following is characteristic of acute pulmonary emboli on CT angiography?
52.
A. Thickened, narrowed pulmonary arteries
B. Pulmonary artery webs
C. Central filling defect within the pulmonary arteries
D. Mosaic perfusion of the lung parenchyma
Question #52
Rationales:
A. Incorrect.
B. Incorrect. Webs are seen with chronic emboli and represent residual thrombus or scarring in a
recanalized vessel. Occasionally, these may calcify.
They are much easier to see on angiography or coronal reconstructions of pulmonary embolism pro-
tocol CT.
C. Correct. The railroad track sign or doughnut sign (with the clot centrally and contrast peripherally)
is a direct sign of acute pulmonary embolus on CT. Chronic pulmonary embolus tends to be eccen-
tric. Occasionally, acute pulmonary embolus may be eccentric. The margin with the lumen, in these
cases, tends to be convex as compared to chronic pulmonary embolus which has a flat or concave
margin to the lumen.
D. Incorrect. Mosaic attenuation or perfusion is a finding more commonly seen with chronic emboli.
The vessels in the darker regions are attenuated and the darker regions do not demonstrate air-trap-
ping.
30 American College of Radiology
31. Section II – Chest Radiology
Which one of the following radiographic features is seen with allergic bronchopulmonary
53.
aspergillosis?
A. Air crescent sign
B. Central bronchiectasis
C. Halo sign
D. Pleural thickening
Question #53
Rationales:
A, C and D are incorrect.
B is correct. Allergic bronchopulmonary aspergillosis is a complex hypersensitivity reaction to
aspergillus organisms colonizing the bronchial lumen. The inflammatory reaction results in cellular
infiltration and release of proteolytic enzymes which produce tissue damage in the bronchial wall.
Excessive mucus production leads to mucoid impaction of the airways. The radiographic hallmark is
central bronchiectasis. Air-crescent sign, pleural thickening, and halo sign are not features of allergic
bronchopulmonary aspergillosis.
31
Diagnostic In-Training Exam 2006
32. Section II – Chest Radiology
Which one of the following conditions demonstrates air-trapping on expiratory high resolution
54.
CT scan?
A. Churg-Strauss syndrome
B. Goodpasture’s syndrome
C. Scimitar syndrome
D. Swyer-James syndrome
Question #54
Rationales:
A. Incorrect. It is a necrotizing vasculitis that is characterized clinically by asthma, fever and
eosinophilia. Radiographic manifestation includes bilateral patchy consolidations but not air-trap-
ping.
B. Incorrect. It is an autoimmune disorder of unknown etiology that is characterized by repeated
episodes of pulmonary hemorrhage. No air-trapping is noted.
C. Incorrect. Also known as congenital pulmonary venolobar syndrome. It is a congenital anomaly that
consists of hypoplasia of the right lung and the right pulmonary artery. There is anomalous venous
drainage of the right lung into systemic venous system, usually below the diaphragm into the inferi-
or vena cava. No air-trapping is noted.
D. Correct. The syndrome is believed to be initiated by a viral bronchiolitis in childhood. It is charac-
terized by hyperlucent lobe or lung. The hyperlucency is due to bronchiolar obliteration and this
results in air-trapping on expiratory CT scan.
32 American College of Radiology
33. Section II – Chest Radiology
Which one of the following mediastinal landmarks is likely to be obliterated by a
55.
bronchogenic cyst?
A. Anterior junction line
B. Psterior junction line
C. Azygoesophageal interface
D. Descending aortic interface
Question #55
Rationales:
C. Correct. Bronchogenic cysts are congenital lesions that result from an abnormality of budding of
the tracheobronchial tree during embryologic development. They are most commonly found in the
subcarinal location and thus there presence in this location will cause obliteration of the azygoe-
sophageal interface. Azygoesophageal interface is formed by the interposition of the aerated lung
and the lateral wall of the azygous vein and esophagus.
A, B and D
Incorrect. Anterior and Posterior junction lines are longitudinal opacities that are formed by the
close apposition of the visceral and parietal layers of the pleura of both the lungs as they come
together anteriorly and posteriorly to the mediastinum. Descending aortic interface is formed by the
juxtaposition of the aerated lung and the soft tissue of the left lateral margin of the descending tho-
racic aorta.
33
Diagnostic In-Training Exam 2006
34. Section II – Chest Radiology
Concerning asbestosis, which one of the following is an expected manifestation?
56.
A. Increased lung volume
B. Upper lung nodules
C. Bronchiectasis
D. Pleural effusions
Question #56
Rationales:
A. Incorrect. Very common in the later stages of asbestosis.
B. Incorrect. Upper lung nodules are typical of silicosis and granulomatous disease, not asbestosis.
C. Incorrect. This is the most common early manifestation of asbestosis and is best demonstrated by
high resolution CT. With time, these progress to a coarse reticular pattern.
D. Correct. Pleural plaques and pleural effusions are common findings in asbestosis.
34 American College of Radiology
35. Section II – Chest Radiology
Which one is MOST likely to cause hoarseness?
57.
A. Anterior mediastinal mass
B. Aorto-pulmonary window mass
C. Right hilar mass
D. Subcarinal mass
Question #57
Rationales:
A. Incorrect
B. Correct. It is situated between the aortic arch and the left pulmonary artery. The space contains
mediastinal fat, ductus ligament, nodes and the left recurrent laryngeal nerve. Thus, mass in this
location can involve the left recurrent laryngeal nerve resulting in vocal cord abnormalities, includ-
ing hoarseness.
C. Incorrect
D. Incorrect
35
Diagnostic In-Training Exam 2006