Sgarbossa criteria for the diagnosis of st elevation myocardial infarction
•
3 recomendaciones•627 vistas

Enhancing the Sgarbossa Criteria for the Diagnosis of ST Elevation Myocardial Infarction

Recomendados
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Sgarbossa criteria for the diagnosis of st elevation myocardial infarction
Similar a Sgarbossa criteria for the diagnosis of st elevation myocardial infarction (20)
Más de Ramachandra Barik
Más de Ramachandra Barik (20)
Último
Último (20)
Sgarbossa criteria for the diagnosis of st elevation myocardial infarction
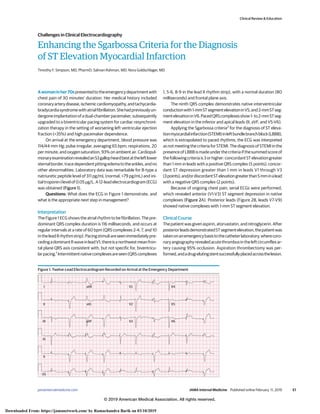
- 1. Enhancing the Sgarbossa Criteria for the Diagnosis of ST Elevation Myocardial Infarction Timothy F. Simpson, MD, PharmD; Salman Rahman, MD; Nora Goldschlager, MD Awomaninher70spresentedtotheemergencydepartmentwith chest pain of 30 minutes’ duration. Her medical history included coronaryarterydisease,ischemiccardiomyopathy,andtachycardia- bradycardiasyndromewithatrialfibrillation.Shehadpreviouslyun- dergoneimplantationofadual-chamberpacemaker,subsequently upgraded to a biventricular pacing system for cardiac resynchroni- zation therapy in the setting of worsening left ventricular ejection fraction (<35%) and high pacemaker dependence. On arrival at the emergency department, blood pressure was 114/44 mm Hg; pulse irregular, averaging 65 bpm; respirations, 20 per minute; and oxygen saturation, 93% on ambient air. Cardiopul- monaryexaminationrevealedanS3gallopheardbestattheleftlower sternalborder,tracedependentpittingedematotheankles,andno other abnormalities. Laboratory data was remarkable for B-type a natriuretic peptide level of 311 pg/mL (normal, <79 pg/mL) and ini- tialtroponinIlevelof0.05μg/L.A12-leadelectrocardiogram(ECG) was obtained (Figure 1). Questions: What does the ECG in Figure 1 demonstrate, and what is the appropriate next step in management? Interpretation The Figure 1 ECG shows the atrial rhythm to be fibrillation. The pre- dominant QRS complex duration is 116 milliseconds, and occurs at regular intervals at a rate of 60 bpm (QRS complexes 2-4, 7, and 10 intheleadIIrhythmstrip).Pacingstimuliareseenimmediatelypre- cedingadominantRwaveinleadV1;thereisanorthwestmeanfron- tal plane QRS axis consistent with, but not specific for, biventricu- larpacing.1 Intermittentnativecomplexesareseen(QRScomplexes 1, 5-6, 8-9 in the lead II rhythm strip), with a normal duration (80 milliseconds) and frontal plane axis. The ninth QRS complex demonstrates native interventricular conductionwith1-mmSTsegmentelevationinV5,and2-mmSTseg- mentelevationinV6.PacedQRScomplexesshow1-to2-mmSTseg- ment elevation in the inferior and apical leads (II, aVF, and V5-V6). Applying the Sgarbossa criteria2 for the diagnosis of ST eleva- tionmyocardialinfarction(STEMI)inleftbundlebranchblock(LBBB), which is extrapolated to paced rhythms, the ECG was interpreted as not meeting the criteria for STEMI. The diagnosis of STEMI in the presenceofLBBBismadeunderthecriteriaifthesummedscoreof thefollowingcriteriais3orhigher:concordantSTelevationgreater than 1 mm in leads with a positive QRS complex (5 points); concor- dant ST depression greater than 1 mm in leads V1 through V3 (3points);and/ordiscordantSTelevationgreaterthan5mminalead with a negative QRS complex (2 points). Because of ongoing chest pain, serial ECGs were performed, which revealed anterior (V1-V3) ST segment depression in native complexes (Figure 2A). Posterior leads (Figure 2B, leads V7-V9) showed native complexes with 1-mm ST segment elevation. Clinical Course The patient was given aspirin, atorvastatin, and nitroglycerin. After posteriorleadsdemonstratedSTsegmentelevation,thepatientwas takenonanemergencybasistothecatheterlaboratory,wherecoro- naryangiographyrevealedacutethrombusintheleftcircumflexar- tery causing 95% occlusion. Aspiration thrombectomy was per- formed,andadrug-elutingstentsuccessfullyplacedacrossthelesion. Figure 1. Twelve-Lead Electrocardiogram Recorded on Arrival at the Emergency Department aVR V1 V4 V2 V5 V3 V6 aVL aVF I II II III VI V5 Clinical Review & Education Challenges in Clinical Electrocardiography jamainternalmedicine.com (Reprinted) JAMA Internal Medicine Published online February 11, 2019 E1 © 2019 American Medical Association. All rights reserved. Downloaded From: https://jamanetwork.com/ by Ramachandra Barik on 03/10/2019
- 2. Repeat troponin measurement 4 hours after presentation showed alevelincreasedto6.12μg/L.Type1acutemyocardialinfarctionwas diagnosed on this basis in the setting of ischemic ECG changes and identificationofcoronarythrombusatangiography.3 Thepatientwas discharged with instructions to take aspirin and prescriptions for clopidogrel, atorvastatin, metoprolol, and captopril. Discussion This case highlights the challenge facing physicians in diagnosing cardiacischemiainthesettingofventricularlypacedrhythms.Italsoem- phasizestheimportanceofcloseinspectionofallECGleadsintheevalu- ation of ischemia and intentional inspection of normal His-Purkinje– conductedQRScomplexes,ifnoted,inanotherwisepacedrhythm. In this case, application of the commonly used Sgarbossa criteria2 tothepresentingECGdidnotfulfillthecriteriaforaSTEMI. Notably,thesecriteriawerederivedinasmallcohortofpatientswith conduction-system disease characterized by LBBB but no pace- maker, where they proved to have high specificity (96%) but poor sensitivity2 (36%)andthusalimitednegativepredictivevalue;meta- analysis of several validation studies show similar results.4 Since the original publication, the Sgarbossa criteria have been extrapolated to right ventricular paced rhythms where retrospec- tiveanalysisshowedsimilartestcharacteristics.5 Thefurtherextrapo- lation to biventricular paced ECGs, which have greater variability in QRS complexes owing to heterogeneity in lead placement, is yet to be validated, although studies are underway (NCT02765477). ToincreasethesensitivityoftheSgarbossacriteria,Smithetal6 tested variations of the criteria in patients with LBBB, and con- cluded that replacing the original third criterion (discordant ST el- evation>5mm)withanewcriterion(“proportionallyexcessive”dis- cordantSTelevation,definedasSTsegmentelevationamplitudeto Swaveamplituderatio>0.25,withapositivetestresultmeetingany 1 of the 3 criteria) increased sensitivity to 91% with minimal effect on specificity (98% to 90%).6 Application of this modified Sgar- Figure 2. Twelve-Lead Electrocardiograms Recorded 30 Minutes After Arrival at the Emergency Department aVR V1 V4 V2 V5 V3 V6 aVL aVF I II II III VI V5 Standard leadsA aVR V1 V7 V2 V8 V3 V9 aVL aVF I II II III VI V5 Posterior leads V7-V9B Clinical Review & Education Challenges in Clinical Electrocardiography E2 JAMA Internal Medicine Published online February 11, 2019 (Reprinted) jamainternalmedicine.com © 2019 American Medical Association. All rights reserved. Downloaded From: https://jamanetwork.com/ by Ramachandra Barik on 03/10/2019
- 3. bossacriteriontothepresentingECG(Figure1)yieldsapositivetest forSTEMI(10thQRScomplexleadV6STelevation,2.5mm;Swave elevation, 6 mm; ratio, 0.41). ThepresenceofnativeHis-Purkinjeconductioninthepresent- ing ECG (Figure 1) allows direct evaluation of the native ST seg- ment, which is altered in cardiac ischemia. Ischemic injury creates voltage gradients, inducing abnormal current flow between nor- mal and ischemic zones (so-called current of injury), which mani- fests as deviations of the ST segment. A number of ECG abnormali- ties may occur after return from ventricularly paced to normal His-Purkinjeconductedcomplexes.Mostnotablearetransientper- sistence of T-wave inversions (so-called cardiac memory or T-wave memory) that can mimic ischemic changes.7 However, ST seg- mentsremainunaffected,allowingforunimpededinterpretationand application of current consensus STEMI criteria (new ST elevation attheJpointof2mminmenor1.5mminwomeninleadsV2and/or V3 and/or of 1 mm in other contiguous chest leads or limb leads).8 ThepresenceofnativeconductionwithST-segmentelevationshould supersede application of the Sgarbossa criteria, even when the cri- teria are not met, and prompt rapid revascularization. Take-Home Points • A focused inspection of all ECG leads should be undertaken in the evaluation of cardiac ischemia. Special attention should be given to native QRS complexes if they occur in an otherwise ventricu- larly paced patient. • In validated populations Sgarbossa criteria2 are relatively specific and thus useful for diagnosing acute STEMI in the setting of con- duction disease, but have low sensitivity and thus poor negative predictive value. The criteria as modified by Smith et al6 moder- ately improve the sensitivity. • The application of Sgarbossa criteria has not yet been assessed or validated in biventricular paced rhythms. • T-wave inversions may occur after a period of abnormal ventricu- lar depolarization. ARTICLE INFORMATION Author Affiliations: Department of Medicine, University of California, San Francisco (Simpson, Rahman, Goldschlager); Division of Cardiology, Department of Medicine, Zuckerberg San Francisco General Hospital and Trauma Center, San Francisco, California (Goldschlager). Corresponding Author: Tim Simpson, MD, PharmD, University of California, San Francisco, 505 Parnassus Ave, San Francisco, CA 94131 (timothy.simpson@ucsf.edu). Published Online: February 11, 2019. doi:10.1001/jamainternmed.2018.7993 Conflict of Interest Disclosures: None reported. REFERENCES 1. Fazelifar A, Jorfi F, Haghjoo M. Electrocardio- graphic patterns in biventricular pacing delivered by second-generation cardiac resynchronization devices. Indian Pacing Electrophysiol J. 2018;18(1): 13-19. doi:10.1016/j.ipej.2017.10.007 2. Sgarbossa EB, Pinski SL, Barbagelata A, et al. Electrocardiographic diagnosis of evolving acute myocardial infarction in the presence of left bundle-branch block: GUSTO-1 (Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries) investigators. N Engl J Med. 1996;334(8):481-487. doi:10.1056/ NEJM199602223340801 3. Thygesen K, Alpert JS, Jaffe AS, et al; Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth universal definition of myocardial infarction. J Am Coll Cardiol. 2018;72(18):2231-2264. doi:10. 1016/j.jacc.2018.08.1038 4. Tabas JA, Rodriguez RM, Seligman HK, Goldschlager NF. Electrocardiographic criteria for detecting acute myocardial infarction in patients with left bundle branch block: a meta-analysis. Ann Emerg Med. 2008;52(4):329-336.e1. doi:10.1016/j. annemergmed.2007.12.006 5. Sgarbossa EB, Pinski SL, Gates KB, Wagner GS. Early electrocardiographic diagnosis of acute myocardial infarction in the presence of ventricular paced rhythm: GUSTO-I investigators. Am J Cardiol. 1996;77(5):423-424. doi:10.1016/S0002-9149(97) 89377-0 6. Smith SW, Dodd KW, Henry TD, Dvorak DM, Pearce LA. Diagnosis of ST-elevation myocardial infarction in the presence of left bundle branch block with the ST-elevation to S-wave ratio in a modified Sgarbossa rule. Ann Emerg Med. 2012;60 (6):766-776. doi:10.1016/j.annemergmed.2012.07.119 7. Shvilkin A, Huang HD, Josephson ME. Cardiac memory: diagnostic tool in the making. Circ Arrhythm Electrophysiol. 2015;8(2):475-482. doi:10.1161/CIRCEP.115.002778 8. O’Gara PT, Kushner FG, Ascheim DD, et al; American College of Cardiology Foundation/ American Heart Association Task Force on Practice Guidelines. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127(4): e362-e425. doi:10.1161/CIR.0b013e3182742cf6 Challenges in Clinical Electrocardiography Clinical Review & Education jamainternalmedicine.com (Reprinted) JAMA Internal Medicine Published online February 11, 2019 E3 © 2019 American Medical Association. All rights reserved. Downloaded From: https://jamanetwork.com/ by Ramachandra Barik on 03/10/2019