Cysts of jaws pathogenesis
•Descargar como PPTX, PDF•
41 recomendaciones•8,395 vistas

Cysts of jaws pathogenesis

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Cysts of jaws pathogenesis
Similar a Cysts of jaws pathogenesis (20)
Más de Revath Vyas Devulapalli
Más de Revath Vyas Devulapalli (14)
Último
Último (20)
Cysts of jaws pathogenesis
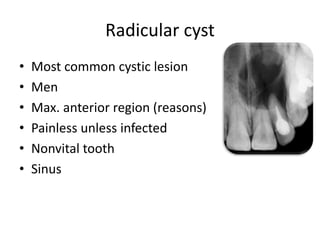
- 1. Radicular cyst • Most common cystic lesion • Men • Max. anterior region (reasons) • Painless unless infected • Nonvital tooth • Sinus
- 2. Pathogenesis • From epithelial cell rests of mallasez 3 PHASES…, • Phase of intiation • Phase of cyst formation • Growth and enlargement of the the radicular cyst
- 3. Phase of intiation o Inflammation (necrotic pulp, bacterial debris) o Bacterial endotoxins* (Aa, p. gingivalis, e. coli) o Immunoglobulins (IgG) , Langerhan’s cells o T – Lymphocytes. o Inflammatory Cytokines(IL- 1, TNF) o Increase in size decreased O2 and increased CO2 tension decreased pH proliferation of cell rests of Mallasez.
- 4. Phase of cyst formation o Release of proteolytic enzymes o Degeneration and death of cells in the center o Connective tissue breakdown along with proliferation of surrounding epithelium may result in formation of several microcysts. o Several microcysts increase in size coalase to form a single established cyst.
- 8. Phase of growth and enlargement • Lytic products of the epithelial and inflammatory cells • raise the osmotic pressure of the cyst fluid. • Cyst walls have property of semipermiable membrane • osmosis across the cyst wall • Increase in size of the cyst
- 10. • How to differentiate between a periapical granuloma and a cyst radiologically??
- 11. • Past data certainly indicate that one cannot rely on the size of the lesion to establish a diagnosis except where the radiographic lesion is 2cm in diameter or larger. • Because histologically, 1/3rd of lesions measuring 10-14 mm are proved to be granulomas and 1/3rd of the lesions less than 5mm are proved to be as cysts!!! • It means there are smaller cysts and evn larger granulomas. • Recent studies state that it may be feasible to differentiate between radicular cysts and periapical granulomas on the basis of radiographic density. (***further studies are required***)
- 12. Dentigerous cyst • Dentigerous cyst develops around an unerupted tooth by accumulation of fluid between the reduced enamel epithelium and the enamel, or between layers of reduced enamel epithelium • Now the question is how does this happen???
- 14. • pressure exerted by a potentially erupting tooth on an impacted follicle • obstructs the venous outflow • induces rapid transudation of serum across the capillary walls. • The increased hydrostatic pressure of this pooling fluid separates the follicle from the crown, with or without reduced enamel epithelium.
- 15. • With time capillary permeability is altered so as to permit the passage of greater quantities of protein above the low concentration of the pure transudate. • Other factors which increase the osmolality of cystic fluid is Glycosaminoglycons (predominantly hyaluronic acid but also appreciable amounts of heparin and chondroitin-4-sulphate)
- 16. • Why the apices of adjacent teeth are more commonly resorbed in dentigerous cyst when compared to other cysts?
- 17. • Reason is PGE2 , a prostagladin which had a role in resorption of cementum and dentin is released in higher amounts from dentigerous cyst. • This PGE2 along with PGE3 results in in resorption of bone, and consequently the enlargement of dentigerous as well as of other cysts.
- 18. • Other bone resortion factors associated with dentigerous cyst are cytokeratins, epidermal growth factors, BMP-4 , epithelial membrane antigen, Carcino embryonic antigen. • In various studies all these are found to be associated with dentigerous cyst.
- 19. • How will you differentiate between a dilated follicle and dentigerous cyst??
- 20. • Some unerupted teeth have a slightly dilated follicle in the pre-eruptive phase. This does not signify a cyst, nor even necessarily a potential cyst unless the pericoronal width is at least 3– 4mm. • After several studies it is concluded that it can be difficult to distinguish between a small dentigerous cyst and a large dental follicle despite the availability of both radiographical and histological information.
- 21. • Is there a chance of development of a dentigerous cyst from radicular cyst of a deciduous teeth??
- 22. • After several studies it was concluded that inflammatory change at the apex of a deciduous tooth may be responsible for initiating a dentigerous cyst of the permanent successor.
- 23. • Is dentigerous cyst a potential cause of ameloblastoma??
- 24. • No evidence to support such a contention. • Indeed, the fact that dentigerous cysts are rarer in South African blacks, compared with whites, whereas ameloblastomas are very much more common in blacks.
- 25. • Much of the confusion has probably arisen for two important reasons. • First, an ameloblastoma, like an OKC, may involve an unerupted tooth, particularly a third molar at the angle of the mandible, and this may be incorrectly interpreted as a dentigerous cyst on radiographs • When subsequently the lesion is removed and diagnosed histologically as an ameloblastoma, the erroneous conclusion may be reached that the ameloblastoma developed from the dentigerous cyst.
- 26. • Second possible reason for believing that many ameloblastomas develop from dentigerous cysts is that biopsies of ameloblastomas may be taken of an expanded locule lined apparently by a thin layer of epithelium. If the surgeon’s provisional diagnosis is dentigerous cyst because of the radiological picture, the pathologist may well regard such histological features as consistent with this diagnosis. When the tumour is removed entirely and a diagnosis of ameloblastoma is made, once again this may be misinterpreted as having developed from a dentigerous cyst.
- 30. Gingival cyst of adults
- 33. • A cystic lesion in which the epithelial lining shows a well-defined basal layer of columnar cells, an overlying layer that is often many cells thick and that may resemble stellate reticulum, and masses of “ghost” epithelial cell that may be in in the epithelial lining or in the fibrous capsule The “ghost” epithelial cells may become calcified. Dysplastic dentine may be laid down adjacent to the basal layer of the epithelium and in some instances the cyst is associated with an area of more extensive dental hard tissue formation resembling that of a complex or compound odontoma.
- 34. • Formation of COC is also similar to that of other cysts but the major difference is CALCIFICATIONS AND GHOST CELLS. So, here the things to be discussed are… • How these calcifications occur?? • What are these ghost cells?? • Are they associated with only COC??
- 35. • Intra-osseous lesions as generally being unilocular radiolucencies with well-circumscribed borders and variable amounts of radiopaque material being present. • epithelial lining of a calcifying odontogenic cyst appears to have the ability to induce the formation of dental tissues in the adjacent connective tissue wall;
- 36. • Ghost cells that are so characteristic a feature of the calcifying odontogenic cyst also occur in other odontogenic cysts, the craniopharyngioma and the calcifying epithelioma of Malherbe, as well as in the other odontogenic tumours • So, the mere presence of ghost cells in a lesion does not justify the diagnosis of calcifying odontogenic cyst.
- 37. • The ghost cells are enlarged, ballooned, ovoid or elongated elliptoid epithelial cells. They are eosinophilic and although the cell outlines are usually well-defined, they may sometimes be blurred so that groups of them appear fused. A few ghost cells may contain nuclear remnants but these are in various stages of degeneration and in the majority all traces of chromatin have disappeared leaving only a faint outline of the original nucleus. The ghost cells represent an abnormal type of keratinisation and have an affinity for calcification.
- 38. NASOPALATINE DUCT CYST • The epithelial-lined cysts of non-odontogenic origin had been thought to be derived from embryonic epithelial residues in the nasopalatine canal and, in the opinion of many workers, from epithelium included in lines of fusion of embryonic facial processes. (CONTROVERSIAL)
- 39. Nasolabial cyst • The only cyst of the oral regions other than the aneurysmal bone cyst to show a female preponderance.
- 40. • nasolabial cyst was considered as the soft tissue equivalent of the globulomaxillary cyst. It was therefore suggested that it arose from epithelium enclaved at the site of fusion of the globular, lateral nasal and maxillary processes. (CONTROVERSIAL).
- 41. • According another hypothesis, it is Developed from the lower anterior part of the nasolacrimal duct. • The mature nasolacrimal duct is lined by pseudostratified columnar epithelium and this is the type of epithelium usually found lining nasolabial cysts.
- 43. MEDIAN PALATINE, MEDIAN ALVEOLAR, MEDIAN MANDIBULAR AND GLOBULOMAXILLARY CYSTS
- 44. • Previously, it had been thought that these cysts developed from epithelium entrapped in the process of fusion of embryonic processes. • It is now believed that they represent posterior extension of an incisive canal cyst in the case of median palatine cyst; anterior extension in the case of median alveolar cyst; and a range of other odontogenic cysts, frequently an odontogenic keratocyst, in the case of the globulomaxillary cysts. • So, they were excluded from the 1992 WHO Classification of epithelial jaw cysts
- 45. Keratocystic odontogenic tumour • There has been a great deal of interest in the odontogenic keratocyst (OKC) since it became apparent that it may grow to a large size before it manifests clinically and that, unlike other jaw cysts, it has a particular tendency to recur following surgical treatment.
- 46. • Intiates by proliferation of cells of dental lamina • Later enlargement occurs • This enlargement depends on various factors • And the factors are…..
- 47. Rate of growth • As they tended to extend along the cancellous component of the mandible without producing noteworthy expansion of the cortical plates, they frequently reached a large size before they were diagnosed. • Few say it has fast rate of growth, and few say it has normal rate of growth
- 48. Role of osmolality in growth of the cysts • mean osmolality of the OKCs (approx 296 mOsm) • mean serum osmolality (282 mOsm) • It is strongly believed that the raised osmolalities have an important role in the expansive growth in the size of the OKC as well as other jaw cysts.
- 49. Role of inflammatory exudate in growth of the cysts • Inflammatory exudate has a negligible role in OKC enlargement. • Its cavity fluid contains low quantities of soluble protein, composed predominantly of albumin and only relatively small quantities of immunoglobulins
- 50. Role of glycosaminoglycans in growth of the cysts • Hyaluronic acid showed the highest frequency and abundance in all three cyst types. • Appreciable amounts of chondroitin-4- sulphate were also observed, particularly in the radicular cysts. • Heparin sulphate showed a higher frequency and abundance in the OKC than the other cysts.
- 51. • Mast cells were widespread in the connective tissue of all cyst types, particularly adjacent to the epithelium, and were probably the source of the heparin. • Degranulating mast cells released heparin and hydrolytic enzymes and the latter facilitated the breakdown of the glycosaminoglycans and proteoglycans.
- 52. Role of collagenolytic activity in growth of the cysts • No similar activity was demonstrable in dentigerous cysts and it was tentatively proposed that enzymatic mechanisms may be important in the growth of OKCs. • Human OKC collagenase degraded types I and II collagens at almost equal rates, but during the same time period no significant degradation of type III collagen occurred, a feature that also characterised human polymorphonuclear (PMN) type collagenase. (‘PMN-like’ characteristics)
- 53. Role of Interleukins, tumour necrosis factor, matrix metalloproteins, tenascin, fibronectin and collagen IV, myofibroblasts, parathyroid hormone related protein
- 54. • IL-1 , TNF OSTEOCLAST ACTIVATING FACTORS are found to be associated with osteolysis of OKC and other cysts • IL-1 ἀ is the principal osteolytic cytokine produced by OKCs leading to bone resorption. • MMP-1 should be regarded as a significant mediator of tissue destruction in these cysts. • MMP-2, demonstrated strongly the proteolytic activity of cyst tissue and its active role in the expansion of the cysts
- 55. • authors investigated the immunocytochemical expression of PTHrP in odontogenic cysts because of evidence that OKCs have less bone resorbing capacity than the dentigerous and radicular cysts. • It is a protein as the putative cause of the humoral hypercalcaemia of malignancy, which has potent parathormone-like activity and is a local factor which regulates cell growth and differentiation. • OKC linings expressed significantly higher levels than those of the dentigerous (P <0.003) and the radicular (P <0.003) cysts.
- 56. • What are the Possible reasons for recurrences of OKC??
- 57. • The first of these is related to their tendency to multiplicity in some patients, including the occurrence of satellite cysts which may be retained during an enucleation procedure. • Second, OKC linings are very thin and fragile, particularly when the cysts are large, and are therefore more difficult to enucleate than cysts with thick walls. • epithelial linings of OKCs had intrinsic growth potential
- 58. • OKCs may also arise from proliferations of the basal cells of the oral mucosa, often referred to as basal cell hamartias, particularly in the third molar region and ascending ramus of the mandible.
- 59. • What is the reason for scalloping , multilocular and loculated outlines in OKC ?????
- 60. • Multicentric pattern of cyst growth brought about by the proliferation of local groups of epithelial cells against the semi-solid cyst contents. • More than one epicenters of growth and with unequal growth activity • Distance between two adjacent epicenters determines the extent of locularity.
Notas del editor
- (this is the reason for arcading pattern in periapical granuloma and cyst histologically)
- It is also thought that cleft formed in between the proliferating epithelial cysts may result in intiation of a radicular cyst This small cyst is lined by proliferating epithelium Quiescent epithelium lining a mature, long-standing radicular cyst Metaplasia of cystic lining resulted in formation of mucous cells and cilited columnar cells
- In approximately 10% of radicular cysts, hyaline bodies, first described by Dewey often referred to as Rushton’s hyaline bodies, are found in the epithelial linings Only very rarely are they present in the fibrous capsule. The bodies measure up to about 0.1mm and are linear, straight or curved or of hairpin shape and sometimes they are concentrically laminated. They are brittle and frequently fracture. Circular or polycyclic bodies are also seen with a clear outer layer surrounding a central granular body. secondary enamel cuticle or probably a form of keratin or bodies of hematogenous origin formed from thrombi of venules hat got strangulated by epithelial cuffs
- Lytic products of the epithelial and inflammatory cells in the cyst cavity provided the greater numbers of smaller molecules which raised the osmotic pressure of the cyst fluid.
- What we see here are cholesterol clefts…, earlier in these plases lies hemosiderin and cholesterol.., the main source of cholesterol was from disintegrating red blood cells in a form that readily crystallises in the tissues. Other possible sourse is plasma lipids as in the case of atherosclerosis.., Once the cholesterol crystals have been deposited in the fibrous capsules of the cysts, they behave as foreign bodies and excite a foreign body, giant cell reaction (Fig. 11.14). In histological sections, the cholesterol crystals are dissolved out and clefts are seen surrounded by dense aggregations of multinucleate giant cells. The cholesterol masses are extruded from the fibrous wall by the foreign body reaction. Invariably, the path of least resistance is into the cyst cavity as the external surface of the cyst may consist of dense fibrous tissue, bone and mucosa. When the reaction reaches the epithelial lining, this ulcerates. The granulation tissue containing the cholesterol protrudes into the cyst cavity and appears macroscopically and microscopically as a ‘mural nodule’
- pressure exerted by a potentially erupting tooth on an impacted follicle obstructs the venous outflow and thereby induces rapid transudation of serum across the capillary walls. The increased hydrostatic pressure of this pooling fluid separates the follicle from the crown, with or without reduced enamel epithelium.
- While ameloblastomas, being of odontogenic epithelial origin, may theoretically arise from dentigerous cyst lining as well as any other odontogenic epithelium, the belief that it commonly arises in this situation and that the dentigerous cyst should therefore be regarded as pre-ameloblastomatous, should be viewed with caution.
- Diagram illustrating the possible pathogenesis of the lateral periodontal cyst. (a) There is expansion of the follicle on the lateral surface of the crown of the unerupted tooth. At this stage a radiograph would show what appeared to be a lateral dentigerous cyst. (b–d) The tooth erupts leaving the expanded follicle behind
- Botryoid odontogenic cyst developing from a lateral periodontal cyst. There are numerous daughter microcysts, many of which also show epithelial plaques. These plaques may be ‘pinched off’ to form granddaughter cysts. Pinched off’ plaques forming further microcysts
- Diagram illustrating the possible histogenesis of the developmental lateral periodontal cyst (a) and the gingival cyst of adults (b). The lateral periodontal cyst is formed from the reduced enamel epithelium by dilatation of the follicle before eruption of the tooth, whereas the gingival cyst of adults is derived from reduced enamel epithelium after eruption of the tooth.
- suggested that the majority of OKCs would take about 6years to recur to a clinically significant size of more than 1 cm diameter but with a wide time range, varying from 1 to 25 years.
- They have referred to the frequent observation of perforation of the overlying bone and firm adhesion of the cysts to the overlying mucosa and recommended that when the cysts were surgically removed, the overlying mucosa should be excised with them in an attempt to prevent possible recurrence or the formation of new cysts from residual basal cell proliferations.